(UroToday.com) The 2025 SESAUA annual meeting featured a bladder cancer session and a presentation by Jonathan Ryan discussing the assessment of hematuria screening disparities using the All of Us database. Disparities in survival for bladder and kidney cancer based on gender and insurance status have been previously well documented.
Microhematuria can be an early indicator of genitourinary malignancy, yet many patients do not receive a full evaluation. Thus, the gap between a microhematuria diagnosis and complete evaluation remains poorly understood among racial groups. The goal of this study presented at SESAUA 2025 was to assess the impact of racial and gender disparities in the evaluation of hematuria using the All of Us prospective clinico-genomic database composed of a diverse population.
This study used version 8 of the All of Us database, which is a nationwide prospective cohort of men accrued from May 2018 to October 2023. To include a group of patients who were evaluated for hematuria, the investigators included patients with >3 RBC/HPF on urinalysis or those with a diagnosis code of gross hematuria in the database. They also excluded patients with other likely causes, for example, those who were pregnant at the time of urinalysis, had a UTI at urinalysis, or had a prior history of bladder, kidney, or ureter cancer or urolithiasis before the urinalysis was completed. Patients were categorized based on the current 2020 AUA guidelines: low risk (3-10 RBC on urinalysis), moderate risk (11-25 RBC on urinalysis), and high risk (>25 RBC on urinalysis or a diagnosis code of gross hematuria). All possible genitourinary imaging was included: (i) CT urogram, (ii) MRI urogram, and (iii) renal/bladder ultrasound.
A total of 17,541 patients were eligible for inclusion: 49% white, 17% black, 21% Hispanic, and 12.3% other race. A full breakdown of the baseline characteristics is highlighted in the following table:
Stratified by low, intermediate, and high risk patients, the following highlights the utilization of cystoscopy, genitourinary imaging, and both cystoscopy and imaging for each race/ethnicity:
On univariable analysis, women had lower screening rates than men for cystoscopy (OR 0.39, 95% CI 0.34, 0.44), genitourinary imaging (OR 0.79, 95% CI 0.73, 0.85), and both (OR 0.51, 95% CI 0.43, 0.61). Generally, minorities had lower overall screening rates for cystoscopy, imaging, and combined modalities: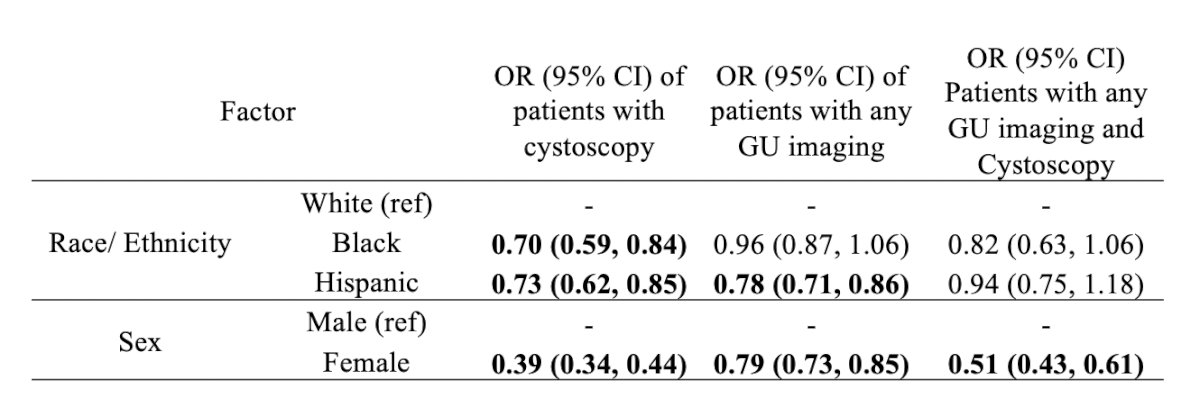
The results of the multivariable analysis show continued gender disparities and are highlighted in the following table: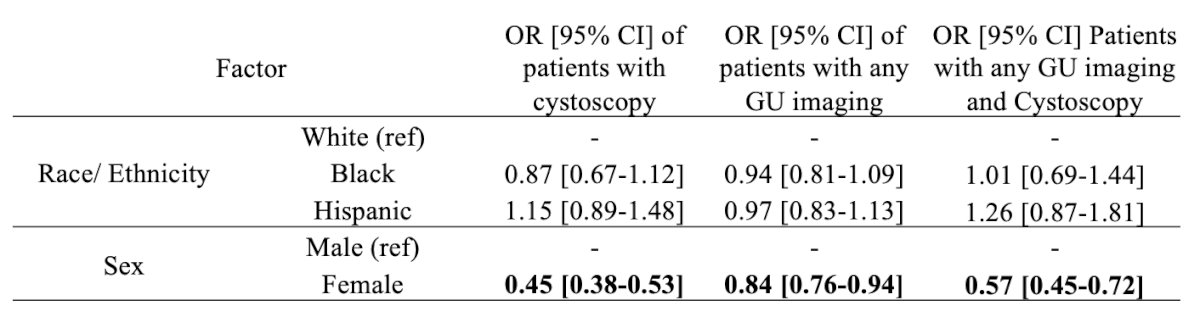
Jonathan Ryan concluded his presentation discussing the assessment of hematuria screening disparities using the All of Us database with the following take-home points:
- This is the largest and most diverse prospective cohort study evaluating disparities in hematuria evaluation
- All minority groups experience disparities in hematuria evaluation compared to White patients
- These disparities are largely influenced by social determinants of health factors, with insurance status being the most significant factor.
- This study confirmed previous findings that women are less likely to undergo hematuria evaluation.
- Among high-risk patients (>25 RBCs on HPF or gross hematuria), Hispanics are particularly less likely to receive initial diagnostic tests or a comprehensive evaluation with both cystoscopy and imaging.
- Improving guideline adherence and addressing social determinants of health are essential to mitigating these disparities.
Presented by: Jonathan Ryan, Nova Southeastern University College of Allopathic Medicine (NSU MD), Davie, FL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Southeastern Section of the American Urological Association (SESAUA) 2025 Annual Meeting, Nashville, TN, Wed, Mar 12 – Sat, Mar 15, 2025.