(UroToday.com) The 2025 South Central AUA annual meeting included a session on urothelial carcinoma, featuring a presentation from Dr. Renil Titus discussing oncological and surgical outcomes of endoscopic therapy compared to surgical resection of upper tract urothelial carcinoma stratified by tumor grade. Treatment with endoscopic or surgical resection of upper tract urothelial carcinoma is risk-stratified based on histological, radiographic, and clinical findings. Alternative approaches due to chronic kidney disease or for solitary kidneys where radical nephroureterectomy is unfavourable include endoscopic ablation or segmental ureterectomy. However, oncological outcomes of endoscopic treatment versus surgical resection (radical nephroureterectomy or segmental ureterectomy) are not well defined. Dr. Titus and colleagues queried the American College of Surgeons - National Cancer Database (ACS-NCDB) to compare the overall survival and surgical outcomes of endoscopic treatment to surgical resection for localized upper tract urothelial carcinoma stratified by grade – high and low.
This study was a retrospective cohort study using the ACS-NCDB dataset, including patients 18-90 years old who were diagnosed with localized urothelial carcinoma of the renal pelvis and ureter from 2004 to 2021, defined as ICD-0-3 codes C65.9 and C66.9 with histology code 8120/3. The primary outcome was overall survival in patients undergoing endoscopic treatment to surgical resection stratified by histologic grade. Secondary outcomes included:
- Surgical outcomes
- Mortality post-operatively
- Length of hospital stay
- 30-day readmission rate
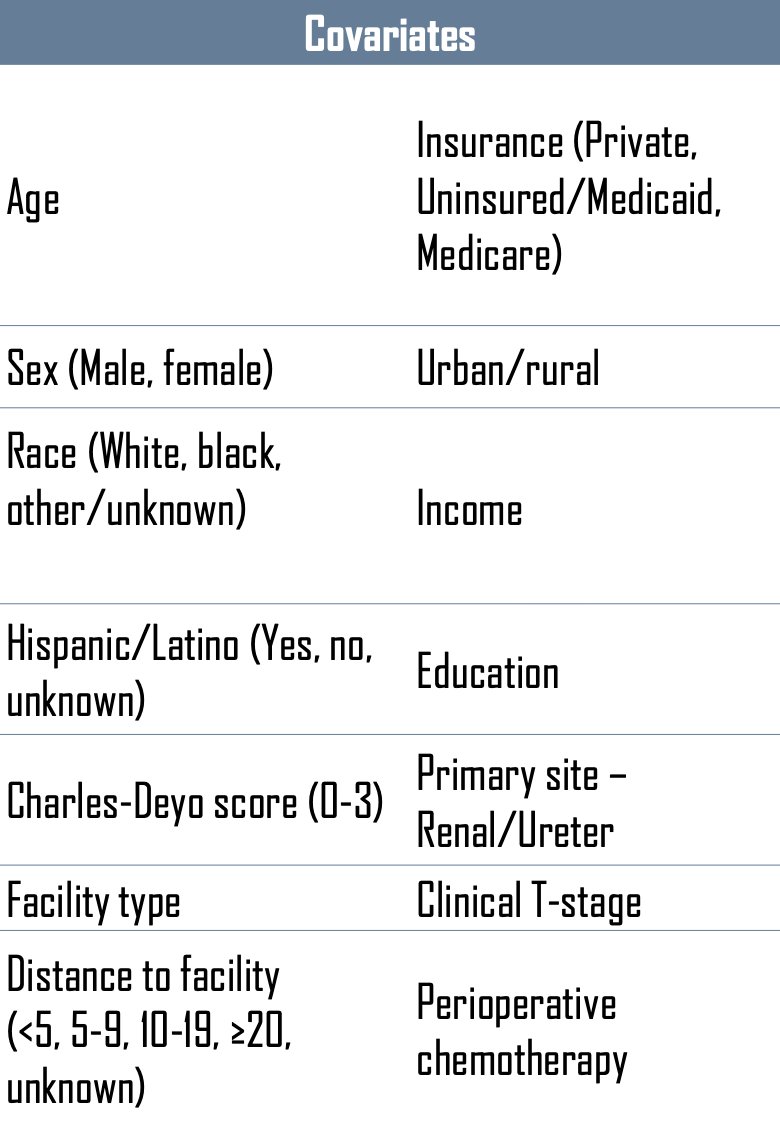
The investigators balanced for granular facility-, patient-, cancer- and procedure-related confounders by propensity score matching with a 1:1 ratio between the endoscopic treatment and surgical resection cohorts with a caliper of 0.004. The covariates were as follows:
Adjusted Kaplan-Meier survival analysis and multivariable Cox proportional hazards regression were used to evaluate the association between treatment and overall survival.
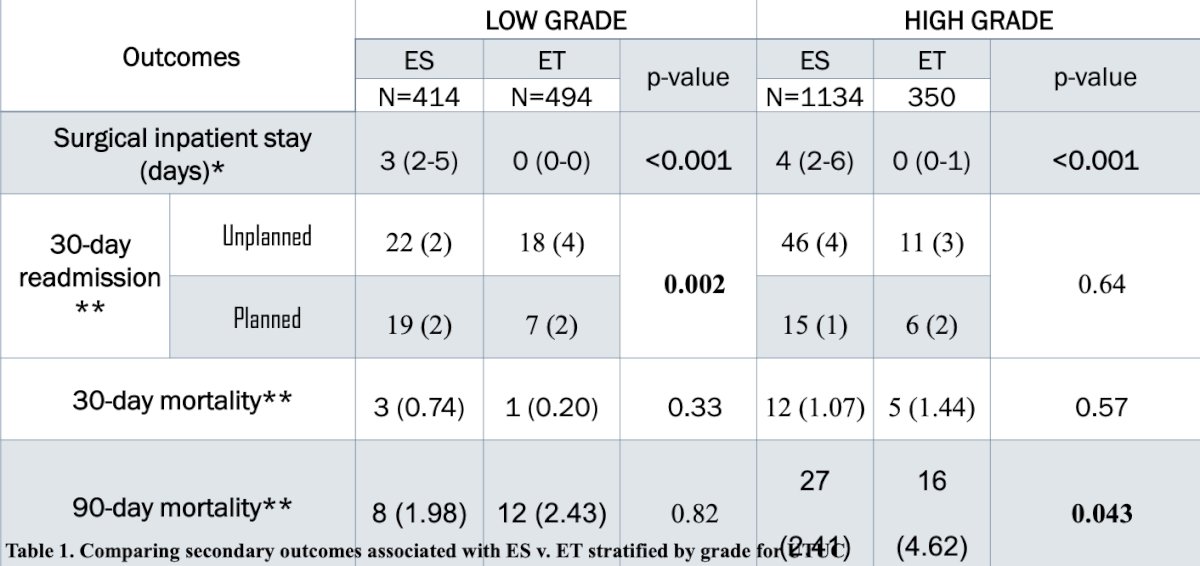
There were 34,750 patients identified, including 1,654 (4.76%) in the endoscopic treatment arm and 33,096 (95.24%) in the surgical resection arm. After propensity score matching, 844 endoscopic treatment patients were compared to 1,548 surgical resection patients. In patients with low grade upper tract urothelial carcinoma (n = 950), endoscopic treatment was associated with no significant difference in all-cause mortality compared to surgical resection (HR 0.93, 95% CI 0.77-1.13; 5-year survival: 61.8% versus 68.5% p = 0.08). In patients with high grade upper tract urothelial carcinoma (n = 1,563), surgical resection as compared to endoscopic treatment was associated with a decreased risk of all-cause mortality (HR 0.51, 95% CI 0.44-0.61; 5-year survival: 51.2% versus 34.0% p < 0.001). The following table compares post-surgical outcomes between endoscopic treatment and surgical resection:
Dr. Titus concluded his presentation discussing oncological and surgical outcomes of endoscopic therapy compared to surgical resection of upper tract urothelial carcinoma stratified by tumor grade with the following take home points:
- Endoscopic therapy should be used with caution in patients with high grade upper tract urothelial carcinoma, who were found to have a detectably greater risk of all-cause mortality, as well as short term post operative mortality
- In low risk grade patients, there was no difference in overall survival associated with these two treatment modalities
- These data are limited by potential residual confounding related to the selection of endoscopic therapy in patients with greater comorbidities
Presented by: Renil Titus, Houston Methodist Hospital, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.