(UroToday.com) The 2025 South Central AUA annual meeting included a session on prostate cancer, featuring a presentation from Dr. Arnold Palacios discussing the role for an intraoperative steep Trendelenburg break during robot-assisted laparoscopic radical prostatectomies (RALP). Notably, steep Trendelenburg positioning may increase the risk of position-related complications in patients undergoing a RALP. An intraoperative break in steep Trendelenburg could potentially decrease the risk of these complications. In this study, Dr. Palacios and colleagues assessed the perioperative outcomes observed in patients undergoing a RALP at their institution and evaluated the impact a steep Trendelenburg break had on positioning-related complications.
This was a retrospective chart review performed on patients who underwent a RALP at Creighton University between January 1, 2017, and August 31, 2023. Patients undergoing multiple concomitant surgeries were excluded from the study. Patients who underwent a steep Trendelenburg break were identified and compared to those who did not undergo a steep Trendelenburg break via univariate analysis using the Kruskal-Wallis test for continuous variables and χ2 test for categorical variables. A Trendelenburg break was undertaken at the discretion of the anesthesia team around the 4-hour mark during a non-critical portion of the procedure. The patient was leveled to zero-degree tilt in the supine position for 15 minutes, then placed in steep Trendelenburg once again, and the case continued in a standard fashion:
Overall, 239 RALPs were included in the study, of which 11 underwent Trendelenburg break. No differences were observed in baseline patient demographics or pathologic characteristics. Patients undergoing a Trendelenburg break were more likely to have increased operating time (438 versus 311 min; p = 0.0025), increased time in steep Trendelenburg (376 versus 256 min; p = 0.0025), and undergo intraoperative suturing of the dorsal venous complex rather than vascular control with the robotic stapler (p = 0.0015). No differences in other major perioperative outcomes were identified, and no positioning-related complications were observed. The lone ocular complication was conjunctivitis, managed appropriately: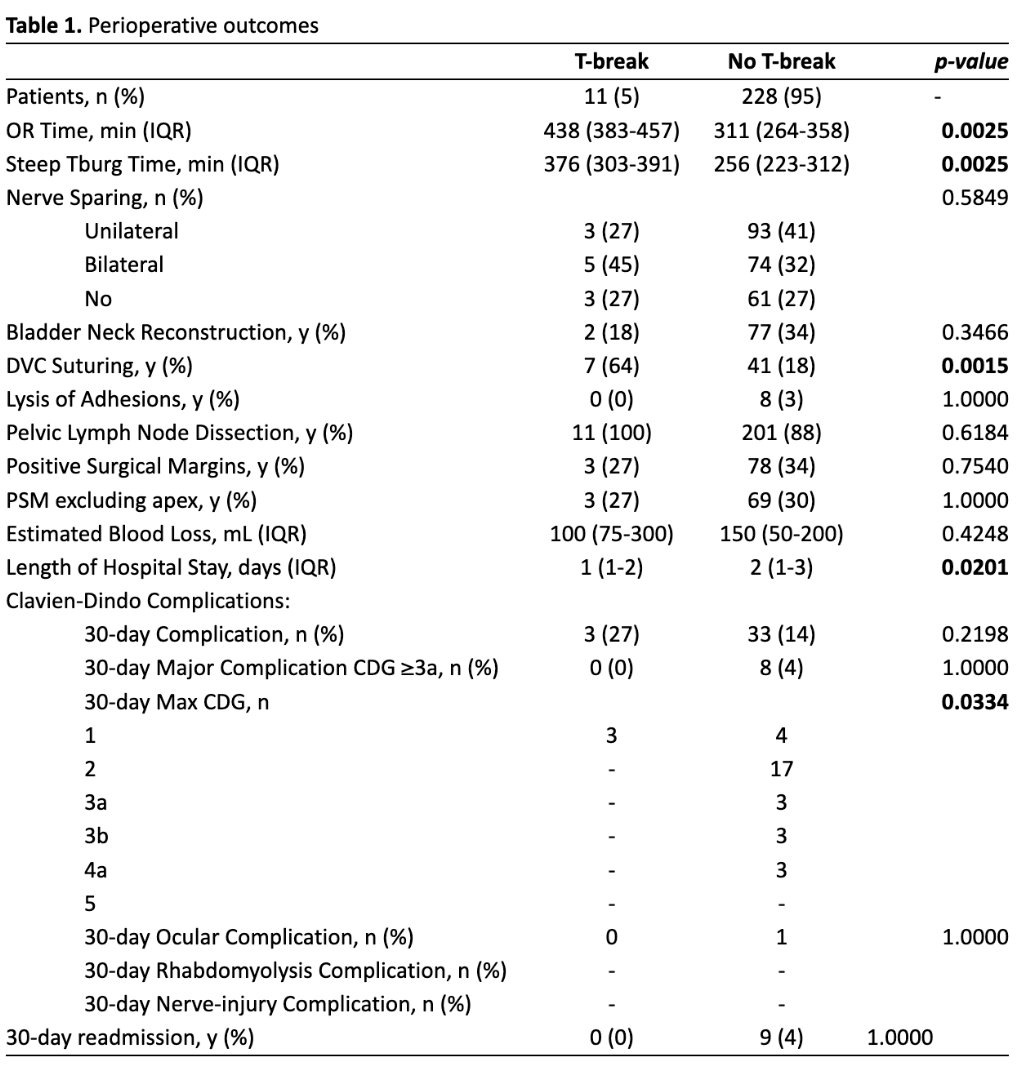
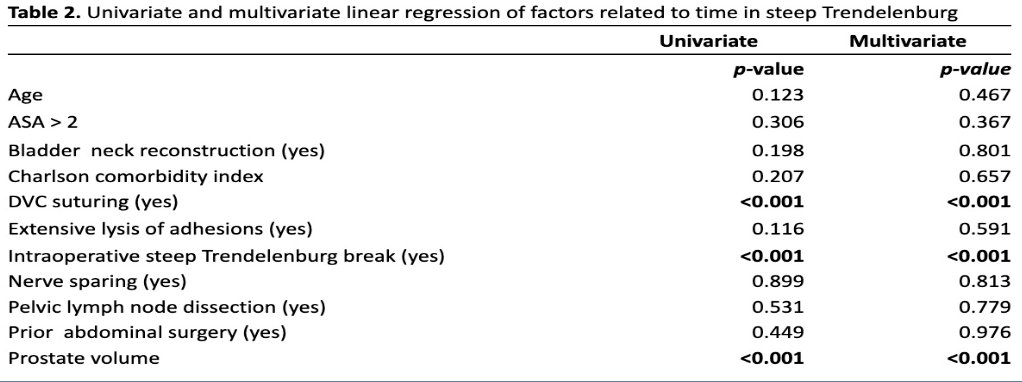
Factors associated with increased time in steep Trendelenburg include: suturing of the dorsal venous complex, Trendelenburg break, and prostate volume:
Dr. Palacios concluded his presentation discussing the role of an intraoperative steep Trendelenburg break during robot-assisted laparoscopic radical prostatectomies with the following take-home points:
- In this study, positioning-related complications were rare in patients undergoing a RALP
- Adoption of a 15-minute intraoperative Trendelenburg break did not impact 30-day complication rate and may discourage trainee case involvement, as it prolongs operating time without any apparent added benefit to the patient
Presented by: Arnold Palacios, MD, Creighton University, Omaha, NE
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.