(UroToday.com) The 2025 South Central AUA annual meeting included a session on kidney cancer, featuring a presentation from Dr. Emily Elliott discussing the efficacy and safety of cytoreductive nephrectomy following immune checkpoint inhibitor combination regimen in metastatic renal cell carcinoma (RCC). Cytoreductive nephrectomy had been the standard of care in metastatic RCC for nearly 20 years prior to systemic therapy. However, the randomized CARMENA trial demonstrated sunitinib alone was noninferior to cytoreductive nephrectomy followed by sunitinib in metastatic RCC patients with intermediate to poor risk disease.1
The immune checkpoint inhibitor combination regimen has become the initial standard of care for metastatic RCC, given its significant survival benefit over sunitinib. Importantly, deferred nephrectomy has not been evaluated in a large randomized study to date. This study assessed the role of cytoreductive nephrectomy in metastatic RCC patients who received immune checkpoint inhibitor combinations at a single institution.
This was a single-center retrospective study of metastatic RCC patients who underwent cytoreductive nephrectomy following immune checkpoint inhibitor combinations from July 2017 to June 2023. Objective response rates were assessed per RECIST version 1.1, and progression-free survival and overall survival were estimated using the Kaplan-Meier method. Adverse events were graded and recorded per CTCAE version 5.0.
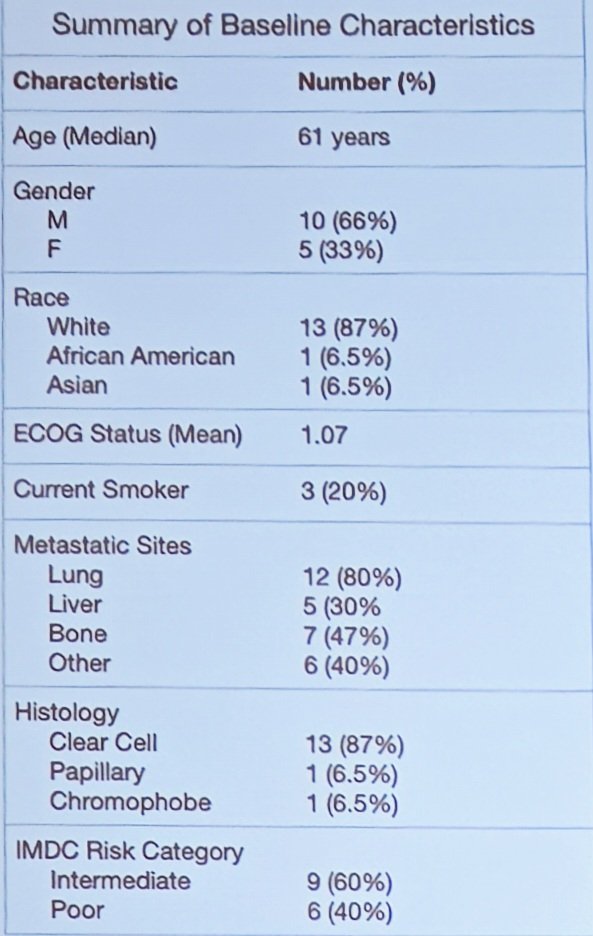
Fifteen patients with metastatic RCC were included, with a median age of 61 years. Over half (n = 8) of patients had an ECOG performance status of 1. Clear cell was the most common histology (n = 13), with the remaining being papillary (n = 1) or chromophobe (n =1). Four patients had sarcomatoid and/or rhabdoid features. Nine patients had IMDC intermediate risk, and 6 patients had IMDC poor risk disease:
The breakdown of treatment is noted in the following pie chart: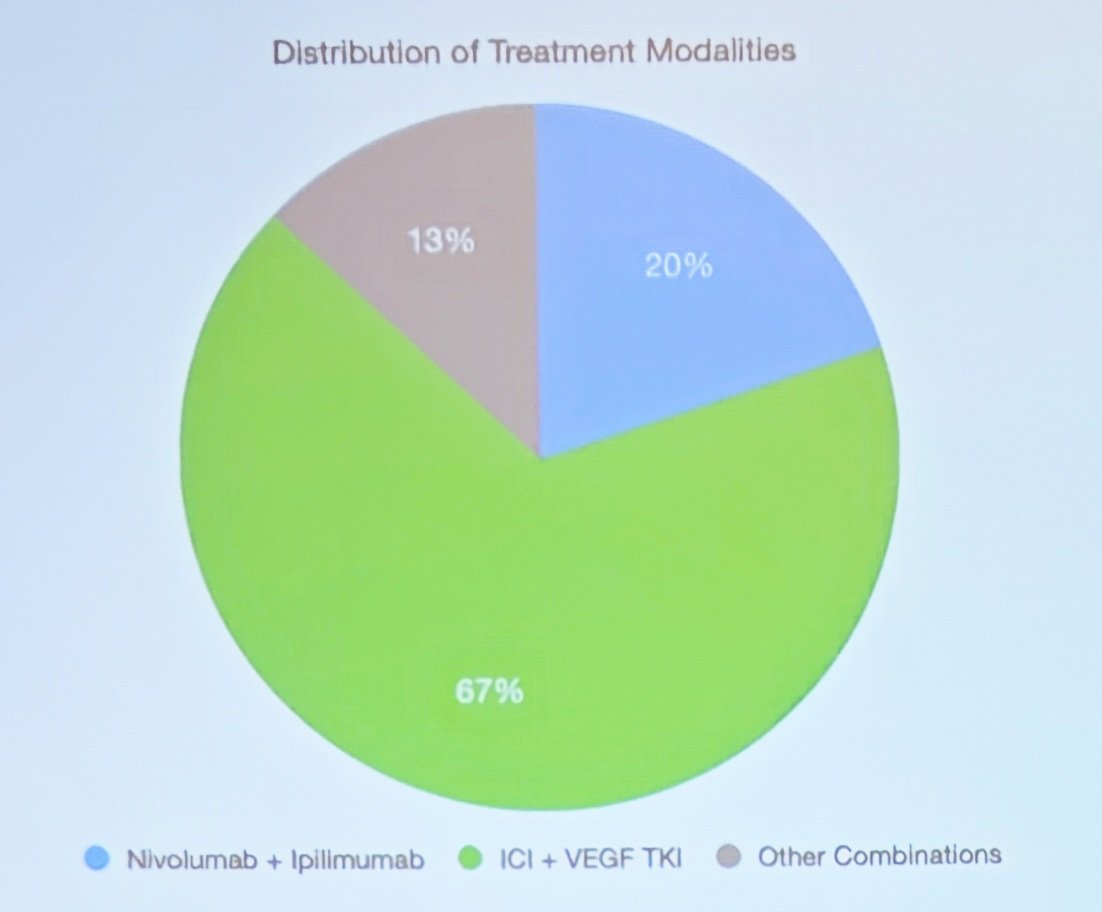
All patients achieved sustained partial response or better before planned deferred cytoreductive nephrectomy, with a mean time to nephrectomy of 11.28 months. At data cutoff, five patients experienced disease progression, while one patient died due to disease progression from subsequent therapy. Median progression-free survival was 50.1 months, and median overall survival was 52.8 months. No major surgical complications were observed, and one grade 3 systemic treatment-related adverse event (autoimmune hepatitis) was observed.
Dr. Elliott concluded his presentation discussing the efficacy and safety of cytoreductive nephrectomy following an immune checkpoint inhibitor combination regimen in metastatic RCC with the following take-home points:
- These findings indicate that deferred cytoreductive nephrectomy following systemic treatment with an immune checkpoint inhibitor combination regimen is clinically feasible in metastatic RCC patients with intermediate to poor risk disease
- While the study is small, retrospective in nature, and single-center, the median overall survival of 52.8 months was consistent with findings in the CARMENA post-hoc analysis
- Minimal systemic therapy or surgery-related treatment disruption was observed
- These findings underscore the safety, practicality, and potential benefit of deferred nephrectomy after immune checkpoint inhibitor-based systemic treatment
- Further prospective studies are warranted to establish the optimal timing and patient population to benefit
Presented by: Emily Elliott, University of Kansas Department of Urology, Kansas City, MO
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References:
- Mejean A, Ravaud A, Thezenas S, et al. Sunitinib alone or after nephrectomy in metastatic renal cell carcinoma. N Engl J Med 2018 Aug 2;379(5):417-427.