(UroToday.com) The 2025 South Central AUA annual meeting included a session on kidney cancer, featuring a presentation from Dr. Horst Emanuel Lagos Beitz discussing the identification of predictive risk factors to refine the indication of adjuvant therapy in intermediate localized and locally advanced renal cell carcinoma (RCC) patients. Pembrolizumab is indicated as adjuvant therapy for RCC patients with adverse clinical and histopathologic characteristics based on results from the KEYNOTE 426 trial.1,2 However, outcomes vary within this group, and identifying patients with lower recurrence risk could reduce unnecessary treatment and adverse effects. This is particularly relevant in resource-limited settings where access to immunotherapy is financially restrictive. The goal of the current study was to identify predictive factors associated with recurrence to optimize patient selection for adjuvant therapy while maintaining oncological outcomes in intermediate- and high-risk localized and locally advanced RCC patients.
A retrospective analysis of 113 intermediate-risk localized and locally advanced RCC patients was conducted. Clinical and histopathologic variables were analyzed using univariate and multivariate statistical methods to identify recurrence predictors. The primary outcome was recurrence-free survival at a median follow-up of 60.5 months. Kaplan-Meier and Cox regression analyses assessed time-to-recurrence differences between subgroups.
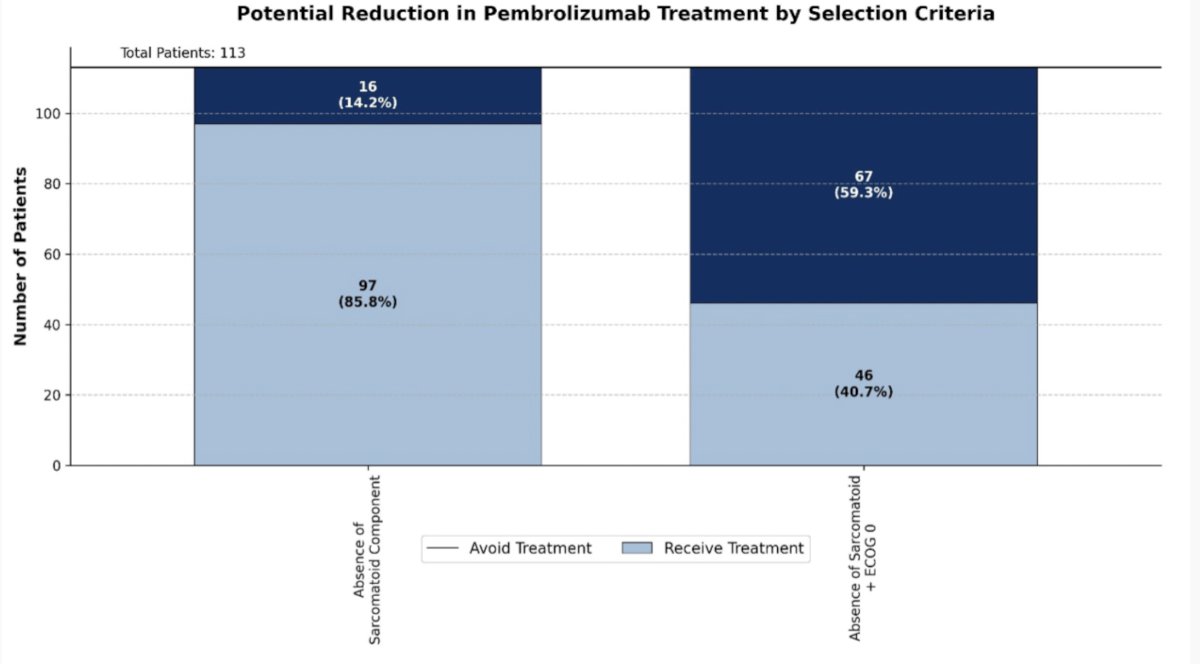
The recurrence rate in intermediate-risk patients was 21.2%. Univariate analysis revealed that sarcomatoid component significantly increased recurrence risk (OR 5.063, 95% CI 1.657-15.471; p = 0.002), with recurrence in 50% of patients with sarcomatoid features versus 16.5% without. Multivariate logistic regression confirmed sarcomatoid component as the strongest predictor (OR 8.814, 95% CI: 1.921-40.444; p = 0.005), while ECOG 0 status was protective (OR 0.215, 95% CI: 0.055-0.844; p = 0.028) for recurrence. Kaplan-Meier analysis demonstrated significantly worse recurrence free survival in patients with sarcomatoid features (Breslow χ² = 10.95, p = 0.001), with median time-to-recurrence of 81.0 months (95% CI 25.2-136.8) versus 225.0 months in those without. Cox regression further validated sarcomatoid component as the sole independent predictor of recurrence (HR 2.730, 95% CI 1.100-6.776, p = 0.030). Using sarcomatoid absence as a selection criterion would allow 85.8% of intermediate-risk patients to avoid pembrolizumab, with a number needed to treat of 6.1 to prevent one recurrence:
Dr. Beitz concluded his presentation discussing the identification of predictive risk factors to refine the indication of adjuvant therapy in intermediate localized and locally advanced RCC patients with the following take home points:
- Sarcomatoid histology was the most powerful predictor of recurrence in intermediate-risk RCC patients, conferring a nearly nine-fold increased risk
- Kaplan-Meier and Cox regression confirmed significantly shorter time to recurrence in affected patients
- Implementing sarcomatoid status as a selection criterion could substantially reduce pembrolizumab use, lowering costs and adverse effects while maintaining oncological outcomes
- All high-risk patients should receive adjuvant therapy, as no predictive recurrence factors were identified in this group
- Prospective validation in larger cohorts is warranted
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References:
- Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med 2019;380(12):1116-1127.
- Powles T, Plimack ER, Soulieres D, et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomized, open-label, phase 3 trial. Lancet Oncol. 2020 Dec;21(12):1563-1573.