(UroToday.com) The 2025 South Central AUA annual meeting included a session on kidney cancer, featuring a presentation from Dr. Emily Leding discussing cytoreductive nephrectomy after immune checkpoint inhibitor therapy in metastatic renal cell carcinoma (RCC). The role of cytoreductive nephrectomy in the management of metastatic RCC has evolved with immune checkpoint inhibitors as first-line therapy. While emerging evidence suggests post-immune checkpoint inhibitor cytoreductive nephrectomy may offer survival benefit for select patients, the safety, perioperative risks, and surgical outcomes remain unclear. Immune checkpoint inhibitors are known to cause immune-related adverse events that could impact surgical outcomes, including delayed wound healing, increased risk of thromboembolic events, and higher perioperative complication rates. Understanding these risks is critical for optimizing patient selection and perioperative care strategies. This study aimed to evaluate the safety and perioperative outcomes of post-immune checkpoint inhibitor cytoreductive nephrectomy, with a focus on complication rates, recovery parameters, and early oncologic outcomes in patients with metastatic RCC.
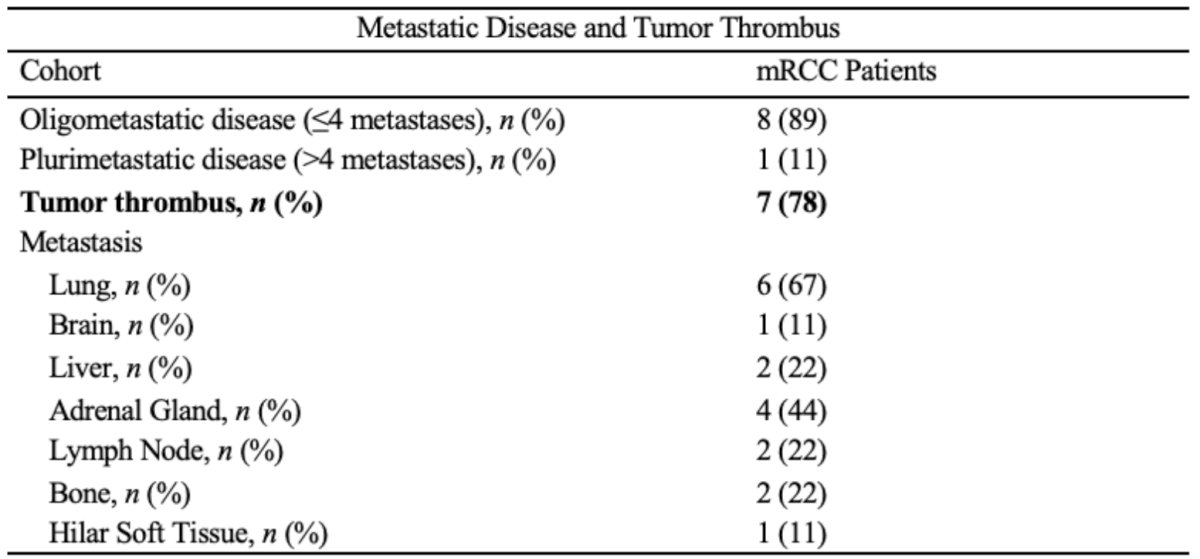
A total of 11 patients were evaluated at the University of Arkansas for Medical Sciences following the approval of immunotherapy in April 2018. The cohort includes 9 patients who underwent post-immune checkpoint inhibitor cytoreductive nephrectomy and two patients who received immune checkpoint inhibitors for nonmetastatic, locally unresectable tumors before later being referred for surgery. Lung metastases were observed in 6 patients (67%), oligometastatic disease (<4 metastases) was present in 8 patients (89%), and 7 (78%) had IVC tumor thrombus:
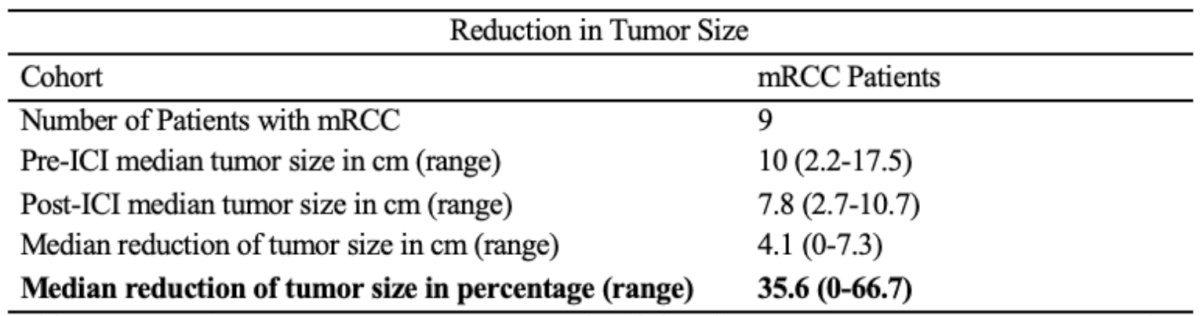
Clinical response to immune checkpoint inhibitor therapy was assessed by comparing pre- and post-treatment imaging, while intraoperative and postoperative outcomes were analyzed for all patients. Following immune checkpoint inhibitor therapy, the median decrease in radiographically enhancing primary tumor size was 4.1 (range: 0-7.3) cm. All metastatic lesions either decreased in size or remained stable:
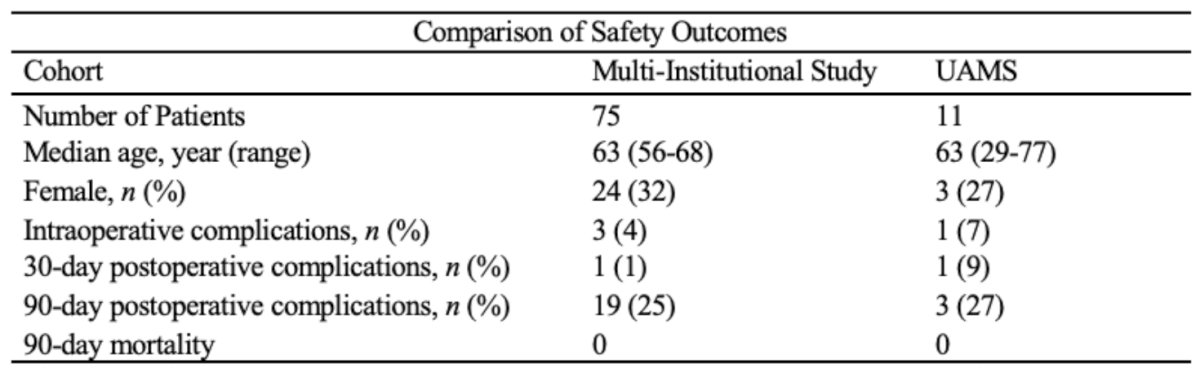
One intraoperative complication (9%) occurred due to pulseless electrical activity following IVC clamp release after cavotomy (Clavien IV). One patient (9%) experienced a 30-day complication (pancreatic fistula, Clavien III), and three patients (27%) experienced a 90-day complication (segmental pulmonary embolism, postoperative seroma, pancreatic fistula; all Clavien III). No patients died within 90-days.
Dr. Leding concluded her presentation discussing cytoreductive nephrectomy after immune checkpoint inhibitor therapy in metastatic RCC with the following take home points:
- Reduction in tumor size suggests that immune checkpoint inhibitor is associated with measurable preoperative tumor shrinkage
- Post-immune checkpoint inhibitor cytoreductive nephrectomy should only be pursued when surgical morbidity risk is low
- The intraoperative pulseless electrical activity and pancreatic fistula can also occur in locally advanced cases despite immune checkpoint inhibitor treatment
- Post-immune checkpoint inhibitor cytoreductive nephrectomy may be a safe and feasible treatment strategy in appropriately selected patients, with low rates of major intraoperative or post-operative complications, compared to upfront surgery for locally advanced tumors
- These results align with multi-institutional studies, suggesting cytoreductive nephrectomy remains a viable option for patients whose metastatic lesions respond to therapy but still have residual primary tumor in the kidney1
Presented by: Emily Leding, University of Arkansas for Medical Sciences, Little Rock, AR
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References: