(UroToday.com) The 2025 South Central AUA annual meeting included a session on bladder cancer, featuring a keynote lecture from Dr. Badrinath Konety discussing the clinical management of non-muscle invasive bladder cancer. Dr. Konety started his presentation by defining BCG unresponsive disease as being at least one of the following:
- Persistent or recurrent CIS alone or with recurrent Ta/T1 disease within 12 months of completion of adequate BCG therapy
- Recurrent high-grade Ta/T1 disease within 6 months of completion of adequate BCG therapy
- All BCG refractory tumors
Additionally, the FDA has set several efficacy thresholds for clinical trials, including a complete response rate of 40% and 30% disease free survival benefit at 12 months. In both intermediate risk and high risk (BCG naïve and BCG unresponsive) disease, there have been a plethora of completed or ongoing clinical trials:

Secondary to many failed therapies (ie. vicinium, valrubicin, heated mitomycin C, etc), there has been a push by stakeholders for novel therapies and combinations. These emerging therapies include:
- Systemic therapy +/- BCG:
- Pembrolizumab
- Sasanlimab + BCG
- Durvalumab + BCG
- Device based/gels:
- TAR 200
- TAR 210
- Mitomycin gel
- Gemcitabine + docetaxel gel
- Gene therapies:
- Nadofaragene firadenovec
- Cretostimogene grenadenorepvec
- Detalimogene veroplasmid
- Other:
- Gemcitabine + docetaxel
- TARA 002
- AU-011 virus drug conjugate
The approval for pembrolizumab in BCG unresponsive disease was based on the KEYNOTE-057 trial.1 Patients received intravenous pembrolizumab 200 mg every 3 weeks for up to 24 months or until patients had evidence of centrally-confirmed disease persistence, recurrence, or progression or unacceptable drug-related toxicity. Overall, among 101 patients, 64% of patients had CIS-only disease, and the 3-month complete response rate, defined as absence of high-risk non muscle invasive bladder cancer or progressive disease, was 41%:
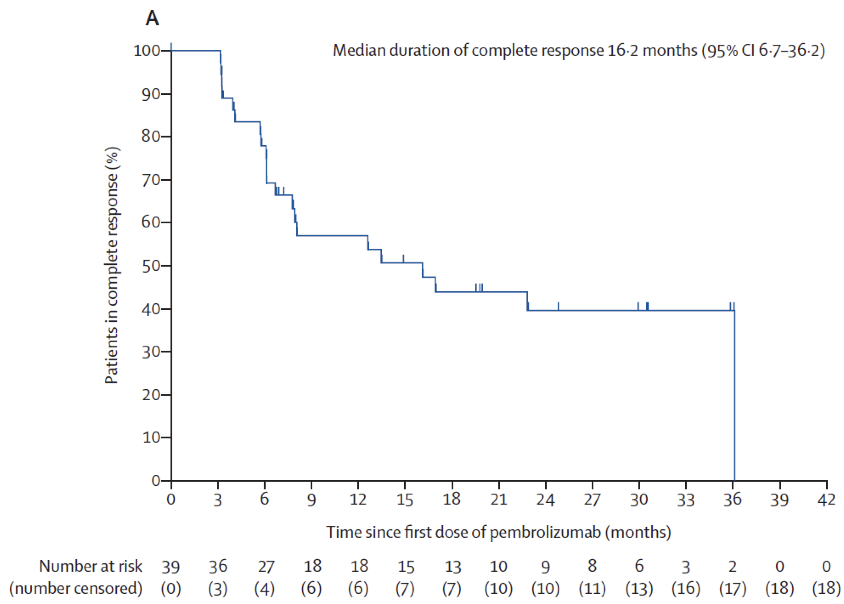
Moreover, 46% of complete responses were maintained at 12 months, 28% of complete responses were ongoing at 36.4 months, 13% of patients had a grade 3 or higher adverse event, and 66% of patients had any adverse event.
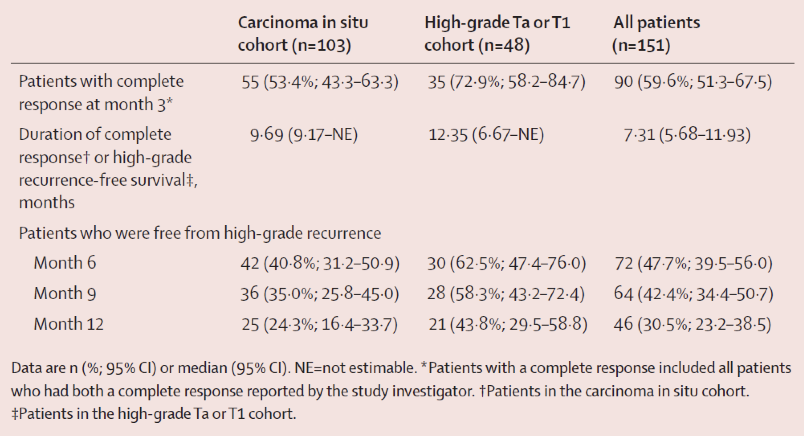
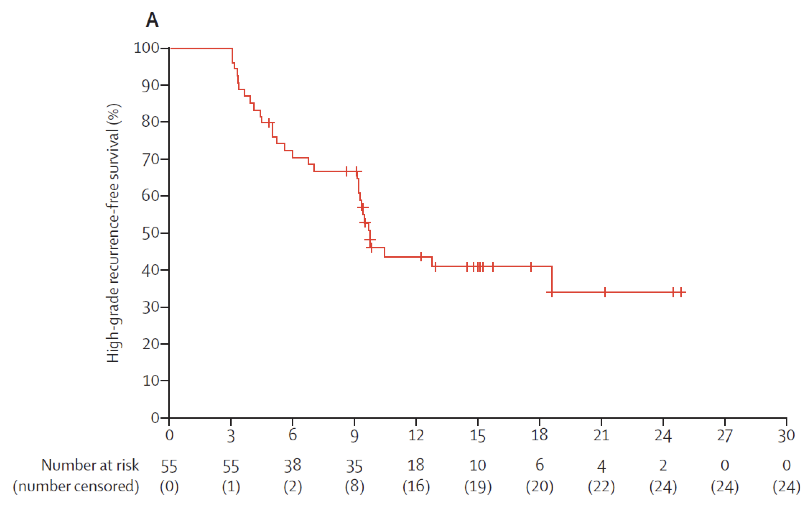
Next, Dr. Konety discussed nadofaragene firadenovec, which was assessed in a phase 3, multicenter, open-label, repeat-dose study across 33 centers in the United States of 151 patients with BCG-unresponsive NMIBC.2 This study met its primary endpoint with 53% of patients with CIS +/- papillary disease achieving a complete response at three months, with 24% maintaining this response by 12 months. Patients with high-grade Ta/T1 tumors achieved 73% and 44% high-grade recurrence-free survivals at three and 12 months, respectively:
In 2024, 5 year follow-up data of this trial were published.3 Over a median follow-up of 50.8 months (IQR 39.1-60.0), among patients with CIS, 5.8% (95% CI 2.2-12.2) were high grade recurrence free at month 57, and 15% (95% CI 6.1-27.8) of patients with high-grade Ta/T1 were high grade recurrence free at month 57:
Among patients with CIS, 49% of patients had their bladder intact, as well as 59% of patients with high grade Ta/T1 disease. Overall survival at 60 months was 80% (71.0, 86.0): 76% (64.6-84.5) and 86% (70.9-93.5) in the CIS and Ta/T1 cohorts, respectively. Additionally, only 5 patients (4 with CIS and 1 with Ta/T1) experienced clinical progression to muscle-invasive disease.
The Quilt 3032 trial4 led to the approval of N-803 (nogapendekin alfa inbakicept: ANKTIVA®), which is an interleukin-15 superagonist (IL-15) that promotes activation and proliferation of natural killer cells, CD8+ T cells, and memory T cells without expanding immunosuppressive T-reg cells. N-803 synergizes with BCG to elicit durable complete responses and has recently been FDA-approved for BCG-unresponsive NMIBC CIS, with or without papillary tumors. In this trial, over a median follow up of 23.9 months, the complete response rate was 71% and the median duration of response was 26.6 months. Based on these results, the FDA granted breakthrough approval of N-803 in April 2024. Updated data from the AUA 2024 showed no difference between >12 or <12 months of prior BCG, which included re-induction in patients who had <T1 disease at 3 months.
Next, Dr. Konety discussed cretostimogene grenadenorepvec, which is an oncolytic immunotherapy designed to selectively replicate in bladder cancer cells with Rb-E2F pathway alterations, commonly found in BCG-unresponsive high risk NMIBC. In addition, cretostimogene also expresses GM-CSF, adding to local and systemic cancer control:

BOND-003 is a phase 3 trial of cretostimogene monotherapy for BCG-unresponsive high-risk NMIBC with CIS. The trial is a single-arm, open-label, intravesical administration of cretostimogene monotherapy for patients with pathologically confirmed BCG-unresponsive high-risk NMIBC with CIS +/- Ta/T1. The endpoints for the trial are complete response at any time, complete response at 12 months, duration of response, progression free survival, and recurrence free survival. Results from BOND-003 (n = 105) included a 75.2% (95% CI 65% - 83%) complete response rate at any time based on central review. This is in the context of all patients having active disease at baseline prior to enrollment and having received adequate BCG therapy as per the FDA 2018 Guidance on BCG-unresponsive NMIBC. Cretostimogene also showed durable response over time:
- 12 month landmark complete response rate: 46.4% (95% CI 36.9, 56.1)
- 24 month landmark complete response rate: 41.8% (95% CI 32.5, 51.6)
- 96.6% free from progression to muscle invasive bladder cancer at month 24
- 84.5% avoided radical cystectomy by month 24
- Among radical cystectomies, 82.4% (14/17) were T0 or non muscle invasive bladder cancer
- All complete responses were centrally confirmed
The SunRISe-1 trial was published in July 2025 in Journal of Clinical Oncology5 and subsequently led to FDA approval of TAR-200 monotherapy on September 9, 2025, for BCG-unresponsive CIS with or without papillary disease. In the SunRISe-1 trial (cohort 2: TAR-200 monotherapy, CIS only), complete response rate and median duration of response were 82.4% (95% CI, 72.6 to 89.8) and 25.8 months (95% CI, 8.3 to not estimable), respectively. Rates of grade ≥3 treatment-related adverse events were 12.9%, and of serious treatment-related adverse events were 5.9%:
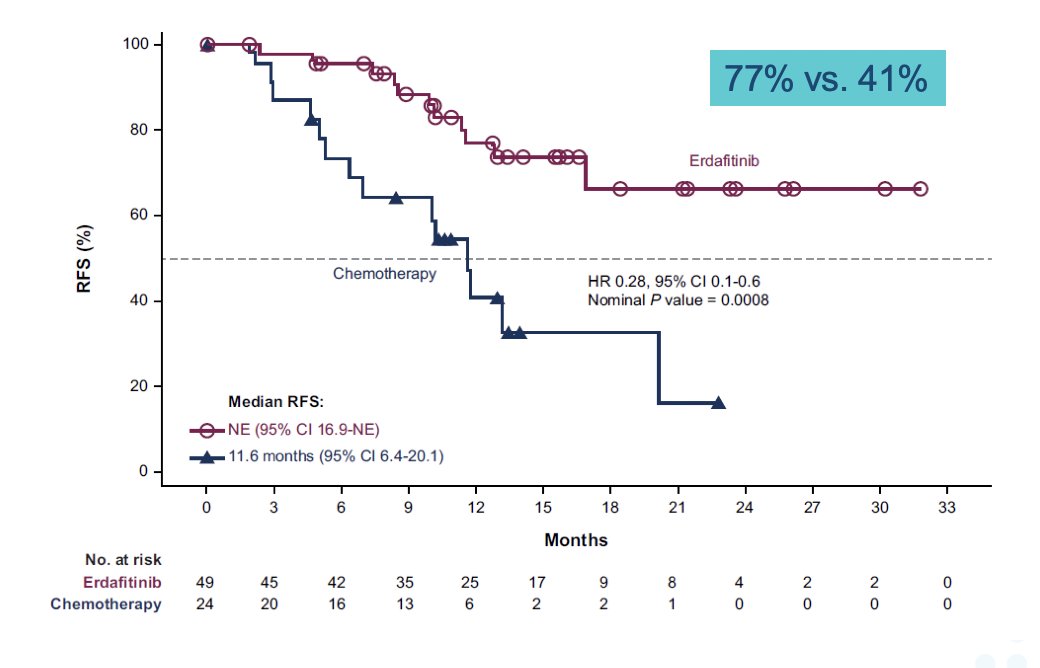
THOR 2 evaluated the activity of oral erdafitinib, a selective pan-FGFR tyrosine kinase inhibitor, versus intravesical chemotherapy in patients with high-risk NMIBC and select FGFR3/2 alterations following recurrence after BCG treatment. There were 73 patients randomized 2:1 to erdafitinib (n = 49) and chemotherapy (n = 24). Over a median follow-up for recurrence free survival of 13.4 months in both groups, the median recurrence free survival was not reached for erdafitinib (95% CI 16.9 months-NE) and was 11.6 months (95% CI 6.4-20.1 months) for chemotherapy (HR 0.28, 95% CI 0.10-0.60):
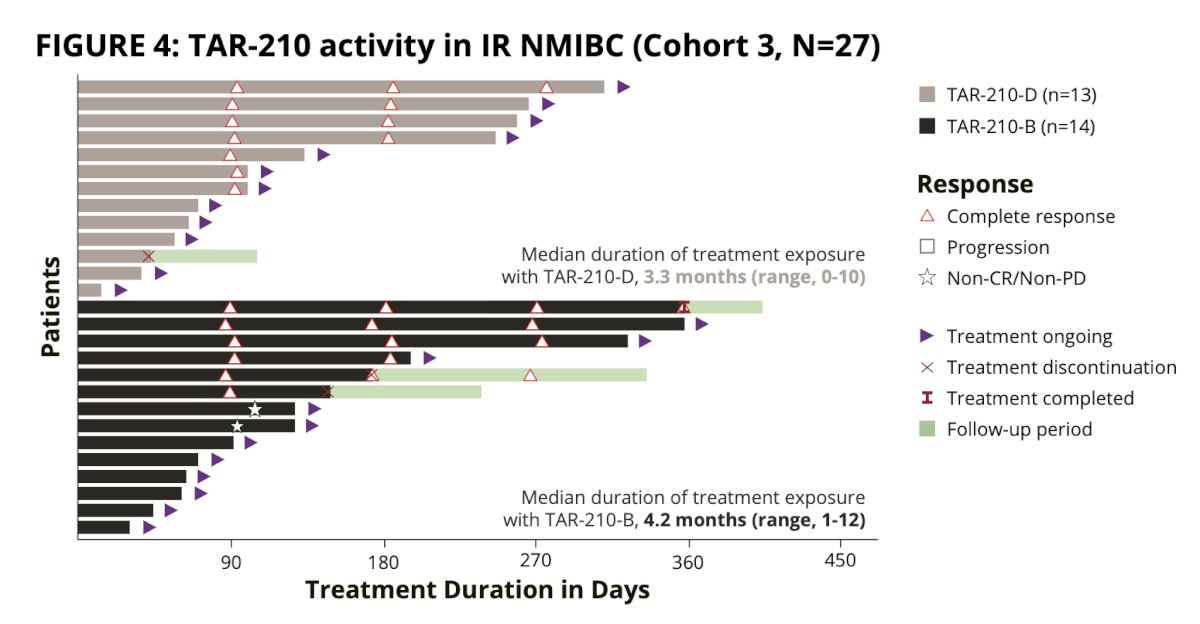
Initially presented at EAU 2024, Dr. Konety discussed a phase I trial of TAR-210, a novel intravesical drug delivery system designed to provide local, continuous release of erdafitinib within the bladder while limiting systemic toxicities. Cohort 1 patients had recurrent, BCG-experienced high-risk non–muscle-invasive bladder cancer (high-grade Ta/T1; papillary only) and refused or were ineligible for radical cystectomy. Cohort 3 patients had recurrent, intermediate-risk non–muscle-invasive bladder cancer (Ta/T1) with a history of only low-grade papillary disease. Before treatment, Cohort 1 patients must have all visible disease resected, whereas Cohort 3 require the presence of visible tumors. TAR-210 systems with two different erdafitinib release rates were evaluated. Response was assessed every 3 months with continued treatment for up to 1 year if recurrence-free (Cohort 1) or in complete response (Cohort 3).
In cohort 1, 11 patients had response assessment, and 9 were recurrence free (recurrence free rate of 82%):
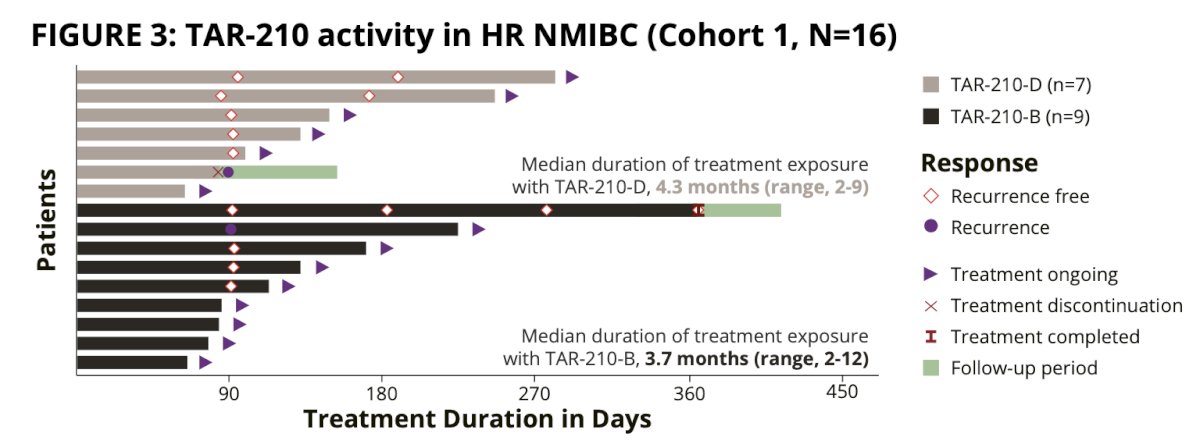
Median recurrence-free survival in Cohort 1 was non-estimable 95% CI 2.96 months to non estimable. In cohort 3, 15 patients had a response assessment, and 13 achieved a complete response (rate: 87%):
This phase I trial paved the way for the MoonRISe-1 for patients with intermediate risk non-muscle invasive bladder cancer, as well as FGFR2/3 alterations by central or local tissue or urine testing. Patients (n = 540) are randomized 1:1 to TAR-210 versus investigator’s choice of intravesical chemotherapy (mitomycin C or gemcitabine). The primary endpoint is disease-free survival, and the trial design for MoonRISe-1 is as follows:

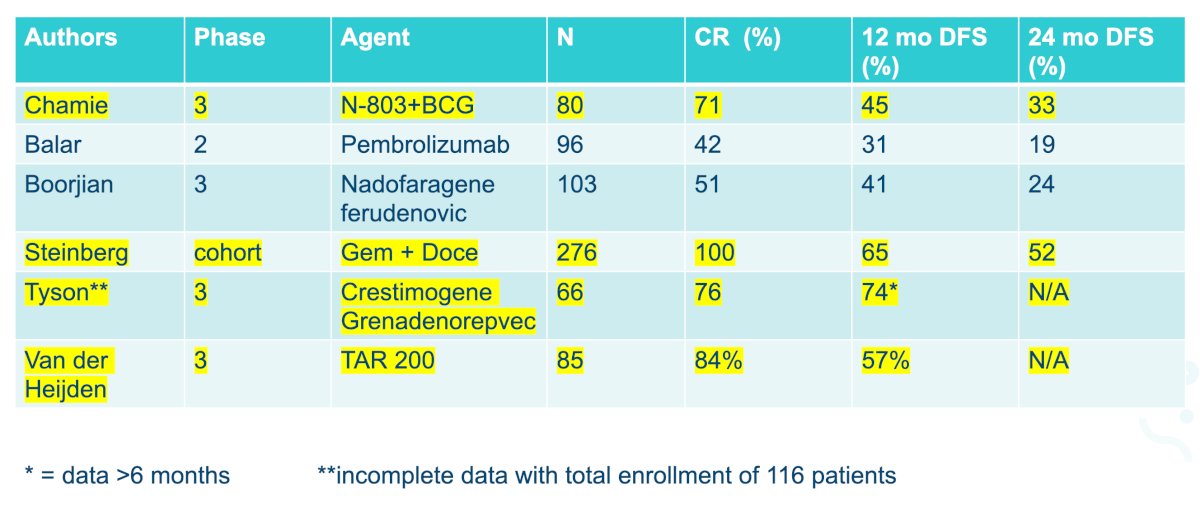
Dr. Konety provided the following table showing a comparison of therapies among BCG unresponsive options:
Dr. Konety concluded this portion of his presentation discussing BCG-unresponsive treatment options with the following take home messages:
- First generation treatment has a ~40% complete response rate
- Second generation treatment has a ~70% complete response rate
- 12 month duration of response is ~20% to ~50%
- Device based/targeted treatment has a ~80% complete response rate
- Systemic immunotherapy has a higher toxicity trade off
- Gene therapies appear to have the least intense schedule and toxicity

For the remaining portion of his talk, Dr. Konety discussed treatment options in the BCG-naïve non muscle invasive bladder cancer setting. In the randomized controlled ATLAS study, patients with newly diagnosed or recurrent low-grade intermediate-risk non-muscle-invasive bladder cancer were randomized to 6 weekly intravesical instillations of UGN-102 (n = 142) or TURBT (n = 140):7

The 3 month complete response rate for UGN-102 was 65% compared to 64% for TURBT, and the 15 month disease free survival for UGN-102 was 72% compared to 50% for TURBT: 
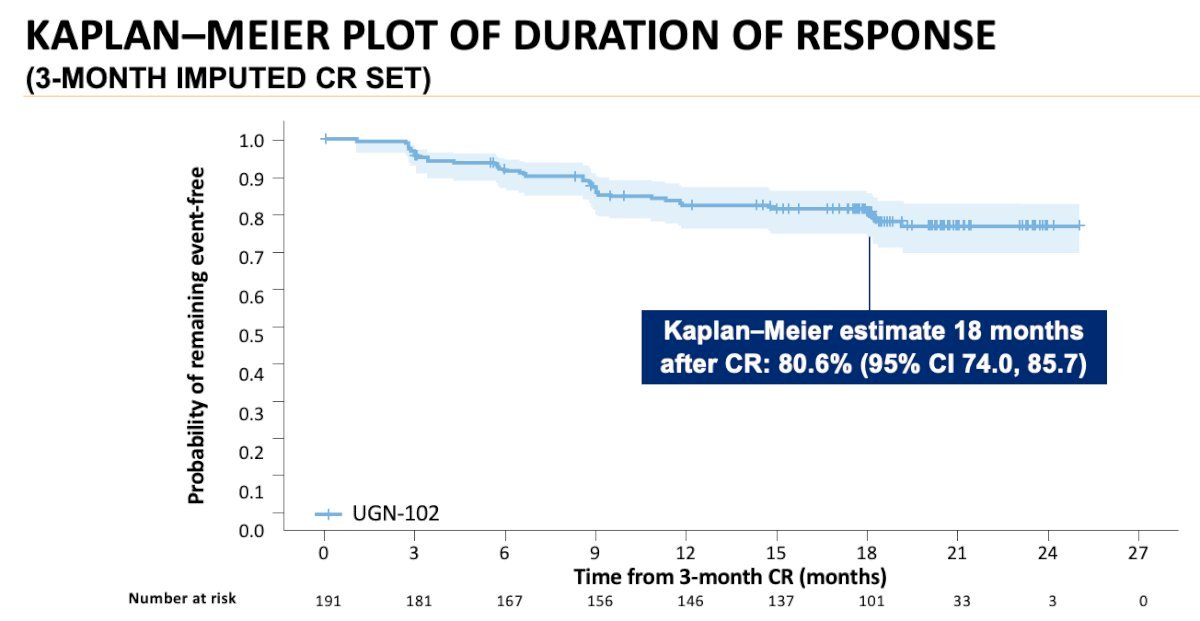
Also assessing UGN-102 was the single-arm ENVISION trial,8 where patients with recurrent low-grade intermediate risk non muscle invasive bladder cancer received 6 weekly intravesical instillations of UGN-102 (n = 240). Patients achieving complete response (negative cystoscopic examination, cytology, and for-cause biopsy) underwent regular surveillance until recurrence, progression, or death. Patients who remained disease-free were planned for long-term follow-up (up to 5 years). Conversely, patients without a complete response at 3 months were offered standard of care therapy. The primary endpoint was 3-months complete response. Of 240 patients enrolled, 228 (95%) received all 6 planned doses. The 3-months complete response rate was 80% (95% CI 74–84.5%), with an 81% (95% CI 74–86%) probability of a maintained response at 12 months. The median duration of response was not estimable over a median 13.9-month follow-up period:
Based on the results from ENVISION, on June 12, 2025, the FDA approved mitomycin for intravesical solution (Zusduri; formerly UGN-102) for the treatment of adult patients with recurrent low-grade intermediate-risk non–muscle invasive bladder cancer.
Next, Dr. Konety discussed the use of gemcitabine + docetaxel in high risk, BCG naïve patients. The Iowa experience with high risk disease included treatment of 107 BCG-naïve patients.9 The 1 year recurrence free survival rate was 85%, the 2 year recurrence free survival rate was 82%, the 1 year high grade recurrence free survival rate was 87%, and the 2 year high grade recurrence free survival rate was 84%. One patient underwent a radical cystectomy secondary to end stage lower urinary tract symptoms:
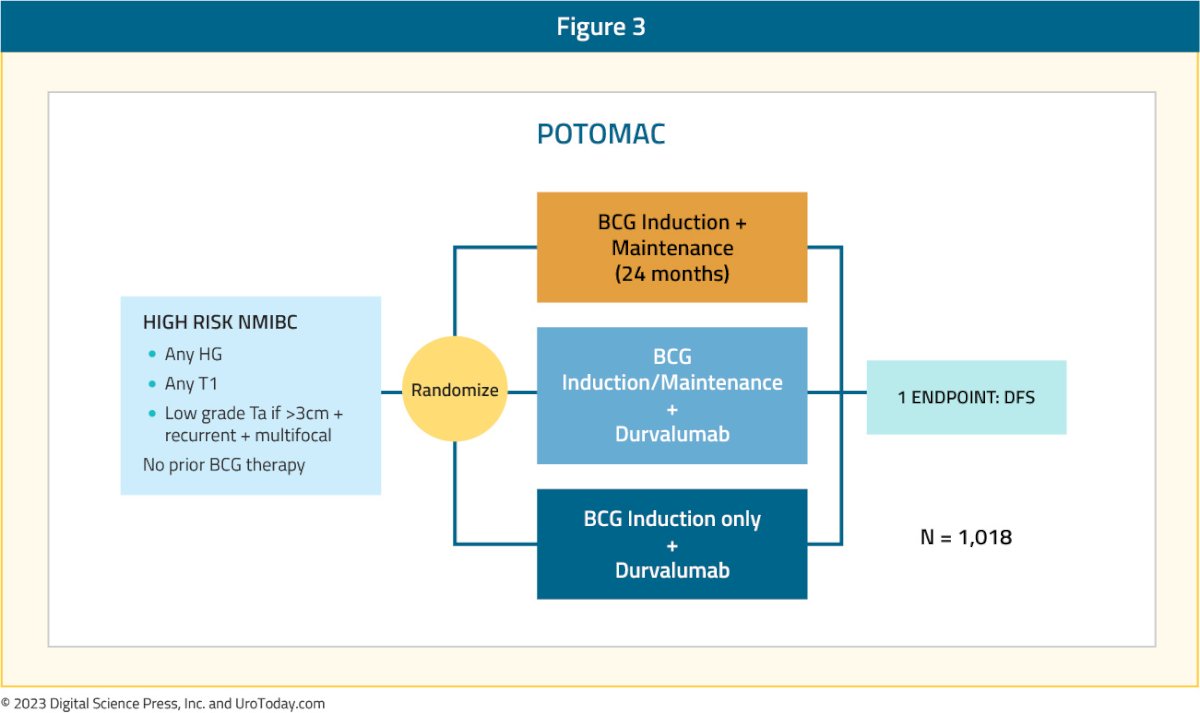
With regards to future perspectives, the BRIDGE trial has a primary objective of evaluating whether gemcitabine + docetaxel is non-inferior to BCG for event free survival in BCG naïve patients. The primary endpoint will be event free survival, while also assessing cystectomy free survival, progression free survival, and safety/toxicity. Dr. Konety notes that BCG induces PD-L1 expression, with higher PD-L1 expression found in BCG non-responders, thus providing the rationale for combining BCG with other immunotherapy agents. The POTOMAC trial is randomizing 1,018 BCG-naïve patients to (i) BCG induction + maintenance for 24 months versus (ii) BCG induction + maintenance + durvalumab versus (iii) BCG induction only + durvalumab, with a primary endpoint of disease free survival:
Finally, Dr. Konety discussed the recently published CREST trial,10 assessing sasanlimab + BCG in BCG-naïve, high risk non muscle invasive bladder cancer. Arm A received sasanlimab administered subcutaneously combined with BCG induction and maintenance, Arm B received sasanlimab with BCG induction only, and Arm C received BCG induction and maintenance alone. The primary endpoint was event-free survival, defined as recurrence of high-grade disease, progressive disease, persistence of CIS, or death from any cause:

The risk of experiencing an event free survival event was 32% lower with sasanlimab + BCG compared to BCG induction and maintenance alone (stratified HR 0.68, 95% CI 0.49–0.94; 1-sided p-value: 0.0095). When comparing Arm B versus Arm C, event free survival was not significantly different between sasanlimab + BCG induction and BCG induction + maintenance, underscoring the importance of BCG maintenance therapy in high-risk NMIBC:
Dr. Konety concluded this portion of his presentation discussing BCG-naïve treatment options with the following take home messages:
- The BCG shortage is prompting a search for alternative treatment modalities
- Gemcitabine + docetaxel appears to work well intravesically and is cheap
- Therapies work by disease type: CIS versus Ta/T1
- Primary chemoablation – is this a real thing?
- BCG augmentation appears to work, but maintenance therapy is required
- Do we need maintenance use of novel drugs?
- Cost may be considerable for treatment: ~$11,000 - $60,000 per dose
Presented by: Badrinath Konety, MD, Allina Health Cancer Institute, Minneapolis, MN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 South Central American Urological Association (AUA) Annual Meeting, Orlando, FL, Wed, Sept 10 – Sat, Sept 13, 2025.
References:
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021 Jan;22(1):107-117.
- Narayan VM, Boorjian SA, Alemozaffar M, et al. Efficacy of intravesical nadofaragene firadenovec for patients with Bacillus Calmette-Guerin-Unresponsive Nonmuscle-Invasive Bladder Cancer: 5-year follow-up from a phase 3 trial. J Urol. 2024 Jul;212(1):74-86.
- Chamie K, Chang SS, Kramolowsky E, et al. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022; 2(1).
- Daneshmand S, Van der Heijden MS, Jacob JM, et al. TAR-200 for Bacillus Calmette-Guerin-Unresponsive High-Risk Non-Muscle-Invasive Bladder Cancer: Results from the Phase IIb SunRISe-1 Study. J Clin Oncol. 2025 Jul 30 [Epub ahead of print].
- Catto JWF, Tran B, Roupret M, et al. Erdafitinib in BCG-treated high-risk non-muscle invasive bladder cancer. Ann Oncol. 2024;35(1):98-105.
- Prasad SM, Huang WC, Shore ND, et al. Treatment of low-grade intermediate-risk nonmuscle-invasive bladder cancer with UGN-102 +/- transurethral resection of bladder tumor compared to transurethral resection of bladder tumor monotherapy: A randomized, controlled, phase 3 trial (ATLAS). J Urol. 2023 Oct;210(4):619-629.
- Prasad SM, Shishkov D, Vladimirov Mihaylov N, et al. Primary Chemoablation of Recurrent Low-Grade Intermediate-Risk Nonmuscle-Invasive Bladder Cancer with UGN-102: A Single-Arm, Open-Label, Phase 3 Trial (ENVISION). J Urol. 2025 Feb;213(2):205-216.
- McElree IM, Steinberg RL, Martin AC, et al. Sequential intravesical gemcitabine and docetaxel for bacillus Calmette-Guerin-naïve high-risk nonmuscle-invasive bladder cancer. J Urol. 2022 Sep;208(3):589-599.
- Shore ND, Powles TB, Bedke J, et al. Sasanlimab plus BCG in BCG-naïve, high-risk non-muscle invasive bladder cancer: The randomized phase 3 CREST trial. Nat Med. 2025 Aug;31(8):2806-2814.