(UroToday.com) The 2026 American Society for Radiation Oncology (ASTRO) Multidisciplinary Radiopharmaceutical Therapy Symposium (MRPTS) held in Palm Desert, California, between February 17th and 18th, 2026, was host to the Plenary Session II. Dr. Siju George delivered a talk titled: Toward Consensus in Lu-177 RPT Dosimetry: Comparing Multi-Timepoint and Single-Timepoint Imaging in Clinical Implementation.
Dr. George began by outlining the objective of the study: to evaluate the dosimetric accuracy and operational implications of multi-timepoint (MTP) versus single-timepoint (STP) imaging protocols for Lu-177–based radiopharmaceutical therapy across all treatment cycles.
Dr. George emphasized the rationale for patient-specific dosimetry, highlighting that it enables truly personalized treatment by tailoring radiation delivery to the individual patient’s disease burden and normal tissue tolerance. He underscores that this approach helps minimize risk to organs at risk (OARs), supports broader and more comprehensive disease coverage, and enhances tumor control through more synergistic and strategic treatment planning. Importantly, patient-specific dosimetry may also allow for safer dose escalation or even reduction in ADT duration, potentially improving both efficacy and quality of life.
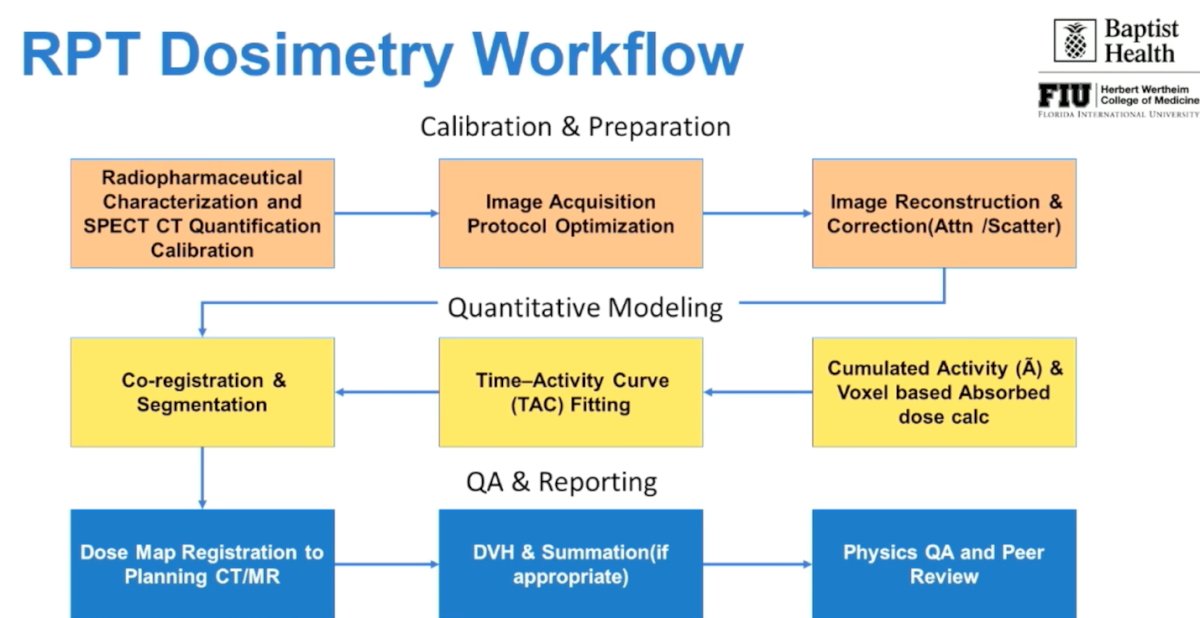
Dr. George then described a structured RPT dosimetry workflow beginning with calibration and preparation, including radiopharmaceutical characterization and SPECT/CT quantification calibration, followed by optimization of image acquisition protocols and appropriate image reconstruction with attenuation and scatter correction. He outlined the quantitative modeling phase, which involves co-registration and segmentation, time–activity curve (TAC) fitting, and calculation of cumulated activity and voxel-based absorbed dose. Finally, he emphasized the importance of QA and reporting, including dose map registration to planning CT/MR, DVH generation and summation when appropriate, and formal physics QA with peer review to ensure accuracy and reproducibility.
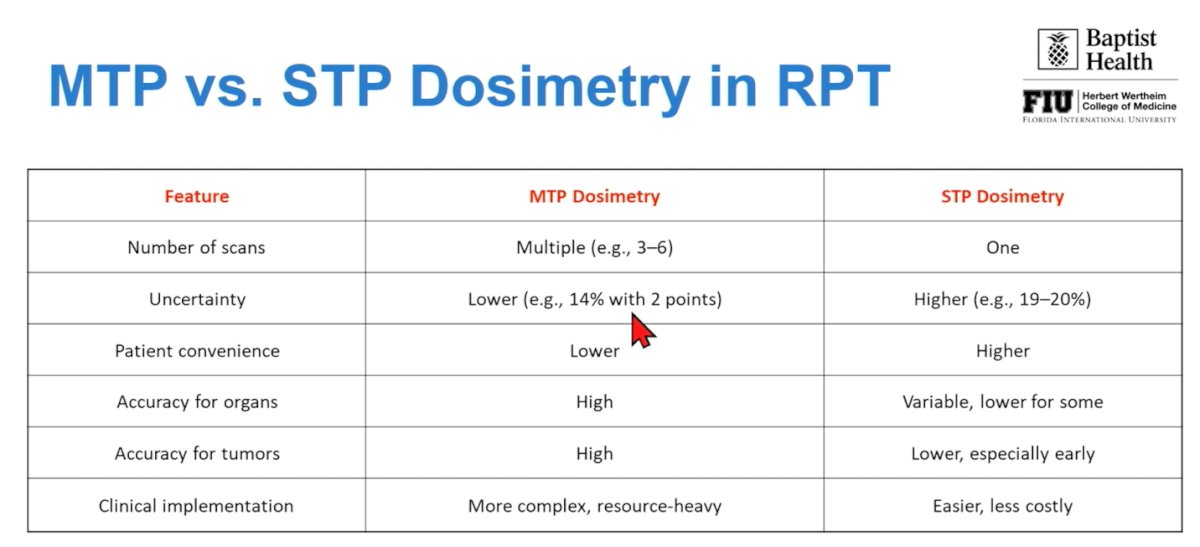
Accurate, patient-specific dosimetry is critical to optimize tumor radiation delivery while minimizing exposure to organs at risk. In this comparison, multi-time-point (MTP) dosimetry, requiring multiple post-treatment scans (typically 3–6)—demonstrated lower uncertainty and higher accuracy for both organ and tumor dose estimation. However, this approach is resource-intensive, less convenient for patients, and more complex to implement in routine clinical practice.
By contrast, STP dosimetry simplifies workflow, requires only one scan, and improves patient convenience, but at the cost of higher uncertainty and potentially lower accuracy, particularly for early tumor dose assessment. The study directly evaluated MTP versus STP dosimetry across treatment cycles to better understand trade-offs in feasibility, precision, and clinical integration, aiming to identify a practical yet reliable dosimetric strategy that could support broader real-world adoption of RPT.
Dr. George explained that patients undergoing Lu-177 PSMA therapy received both MTP and STP imaging during each treatment cycle to allow direct intra-patient comparison.
Under the MTP protocol, quantitative SPECT/CT scans were performed at 4, 48, 72, and 96 to 106 hours post-infusion as illustrated below. The STP protocol consisted of a single quantitative scan obtained at either 72 or 96 hours, with independent dose estimates calculated from each timepoint. Dosimetry analyses were performed using MIM SurePlan MRT software. Time-activity curves were generated for both approaches, and absorbed doses were calculated for tumor volumes and critical organs. STP-derived dose estimates were then compared against the corresponding MTP results for each treatment cycle to assess accuracy.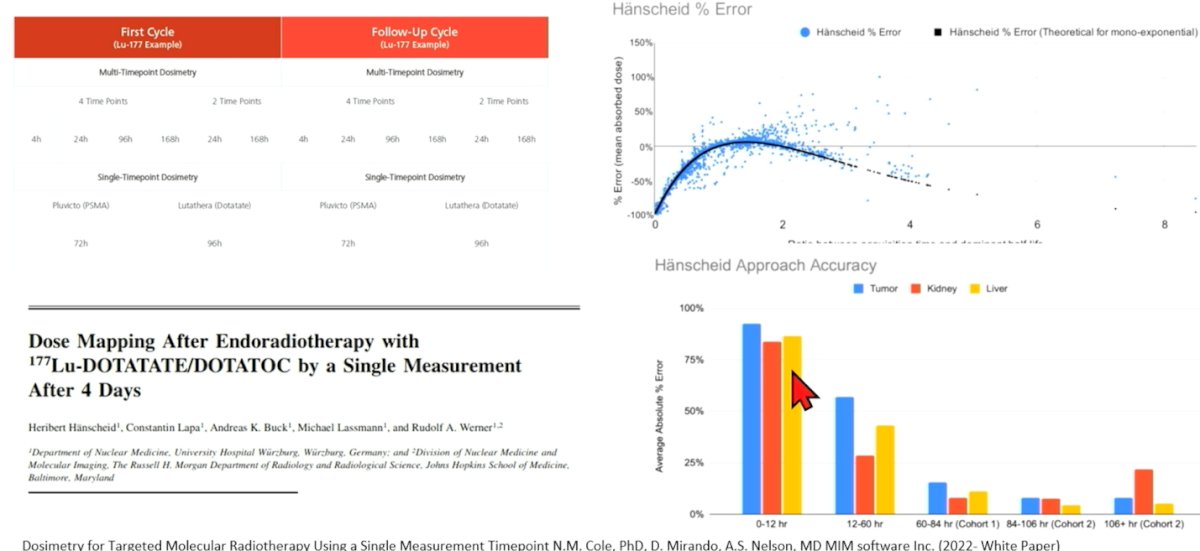
Additionally, key technical differences further distinguish MTP from STP dosimetry (shown below). MTP relies on exponential time–activity curve (TAC) fitting across multiple imaging time points, enabling voxel-wise absorbed dose calculations (Gy) and time-integrated activity measurements with high software-driven accuracy. In contrast, STP typically assumes mono-exponential clearance kinetics and provides an estimated absorbed dose based on a single acquisition, often using simplified or manual workflows that may reduce precision. Moreover, comparison to EQD2 modeling is more robust with MTP, whereas STP approaches are less feasible or potentially less valid when biologically adaptive modeling is required.

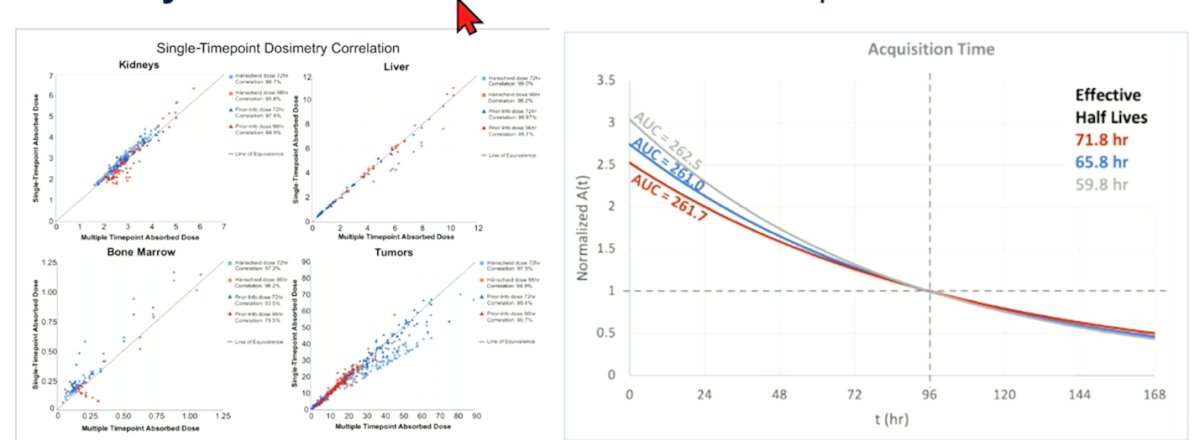
Dr. George reported that MTP dosimetry provided the most accurate and comprehensive dose assessments across all treatment cycles and served as the reference standard; however, this approach is logistically demanding for both patients and clinical departments. In contrast, STP imaging performed at 72 or 96 hours produced dose estimates with greater uncertainty compared to MTP-derived values, highlighting the trade-off between practicality and precision in routine RPT implementation.
Importantly, incorporating a second time point, for example, at 4 and 96 hours, reduced uncertainty to approximately 14%, bringing estimates closer to the reference standard. While STP protocols decreased patient burden and reduced resource utilization, they introduced greater variability, particularly in lesions with atypical clearance kinetics. These results are consistent with prior modeling studies and highlight the trade-off between operational feasibility and dosimetric precision.1-3
Importantly, the investigators proposed a hybrid imaging strategy to balance accuracy with feasibility. In cycle 1, MTP imaging was performed at approximately 4–24, 48–72, and 72–106 hours post-infusion to establish patient-specific kinetics and serve as the reference for dosimetry. For subsequent cycles (cycles 2–6), a STP scan at 72–106 hours post-infusion was recommended, leveraging prior kinetic data while substantially reducing patient and departmental burden. This approach aims to preserve dosimetric reliability while improving workflow efficiency and real-world implementability.
Lastly, he addressed combination strategies, highlighting that integrating External Beam Radiation Therapy (EBRT) with Lu-177–PSMA may increase tumor biologically effective dose (BED) without a proportional increase in toxicity, thereby supporting individualized rather than fixed-activity treatment approaches. He emphasized that patient-specific dosimetry consistently demonstrates substantial inter-patient dose variability, reinforcing the need for adaptive treatment planning and closer safety monitoring. Importantly, real-world dosimetry data may help bridge current evidence gaps and directly inform clinical decision-making, including whether to continue, escalate, or discontinue therapy.
Dr. George concluded his presentation with the following key points:
- Multi-timepoint imaging remains the reference standard for Lu-177 radiopharmaceutical therapy dosimetry.
- Carefully selected single timepoints can provide acceptable accuracy and may be a reasonable alternative in resource-constrained settings.
- Routine dual-timepoint imaging represents a practical compromise, enabling broader adoption of patient-specific dosimetry with minimal loss of precision.
Presented by: Siju George, PhD, Herbert Wertheim College of Medicine, Florida International University, Miami, FL.
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society for Radiation Oncology (ASTRO) Multidisciplinary Radiopharmaceutical Therapy Symposium (MRPTS) held in Palm Desert, California, between February 17th and 18th, 2026.
References:- Cole et al. (2022, MIM Software White Paper): https://go.mimsoftware.com/single-timepoint-dosimetry-white-paper
- Peters SMB, Mink MCT, Privé BM, de Bakker M, de Lange F, Muselaers CHJ, Mehra N, Witjes JA, Gotthardt M, Nagarajah J, Konijnenberg MW. Optimization of the radiation dosimetry protocol in Lutetium-177-PSMA therapy: toward clinical implementation. EJNMMI Res. 2023 Jan 24;13(1):6. doi: 10.1186/s13550-023-00952-z. PMID: 36692682; PMCID: PMC9873880.
- George SC, Samuel EJJ. Developments in 177Lu-based radiopharmaceutical therapy and dosimetry. Front Chem. 2023 Jul 31;11:1218670. doi: 10.3389/fchem.2023.1218670. Erratum in: Front Chem. 2024 Apr 17;12:1410803. doi: 10.3389/fchem.2024.1410803. PMID: 37583569; PMCID: PMC10424930.