(UroToday.com) The Interdisciplinary Genitourinary Cancer Forum 2025, held between June 19 – 21, 2025 held in St. Petersburg, Florida, United States, was host to the Prostate Cancer Session 7: Non-metastatic Castration Resistant Prostate Cancer (nmCRPC). Dr. Shereif Gamie discussed the impact of molecular targeted imaging on Non-metastatic Castration Resistant Prostate Cancer.
Dr. Gamie began by highlighting the “ostic” component of diagnostic PET/CT and PET/MRI imaging, emphasizing their power in targeting diverse molecular processes. These modalities can assess glucose metabolism using FDG, detect the density of prostate-specific membrane antigen (PSMA) receptors via C11 acetate or PSMA tracers, and evaluate skeletal osteoblastic activity through NaF bone PET/CT. Additionally, PET imaging can target somatostatin receptors with Ga-68 Dotatate, and amyloid tangles in Alzheimer’s disease using Amyvid. This underscores the versatility of PET-based diagnostics in visualizing specific biological targets.
There is an evolving role of prostate-related molecular targeted radioligand imaging. However, the definitions of castration-resistant prostate cancer (CRPC) across major guidelines differ. According to the NCCN guidelines, CRPC is defined as clinical, radiographic, or biochemical progression despite castrate levels of serum testosterone (<50 ng/dL). The EAU/ESTRO/SIOG further specify progression types, including biochemical progression (PSA >2 ng/mL above nadir with two consecutive 50% increases one week apart) or radiologic progression (≥2 new bone lesions or a new soft tissue lesion per RECIST criteria). The AUA definition includes rising PSA despite surgical or medical castration, with or without radiologic evidence of metastasis or prior docetaxel therapy, and specifies PSA progression as >2 ng/mL above nadir with at least a 25% rise.1-3
PSMA is a transmembrane glycoprotein highly expressed on prostate cancer cells. The PSMA protein has both extracellular and intracellular domains, enabling it to serve as a target for various imaging and therapeutic strategies. Antibodies such as J591 bind to the extracellular domain, while 7E11 targets the intracellular portion. Radioligands can be designed to bind PSMA through a pharmacophore linked to a radiolabeled group via spacers, allowing targeted imaging or therapy. Multimeric approaches may enhance binding affinity and specificity by engaging multiple receptors simultaneously, as illustrated below.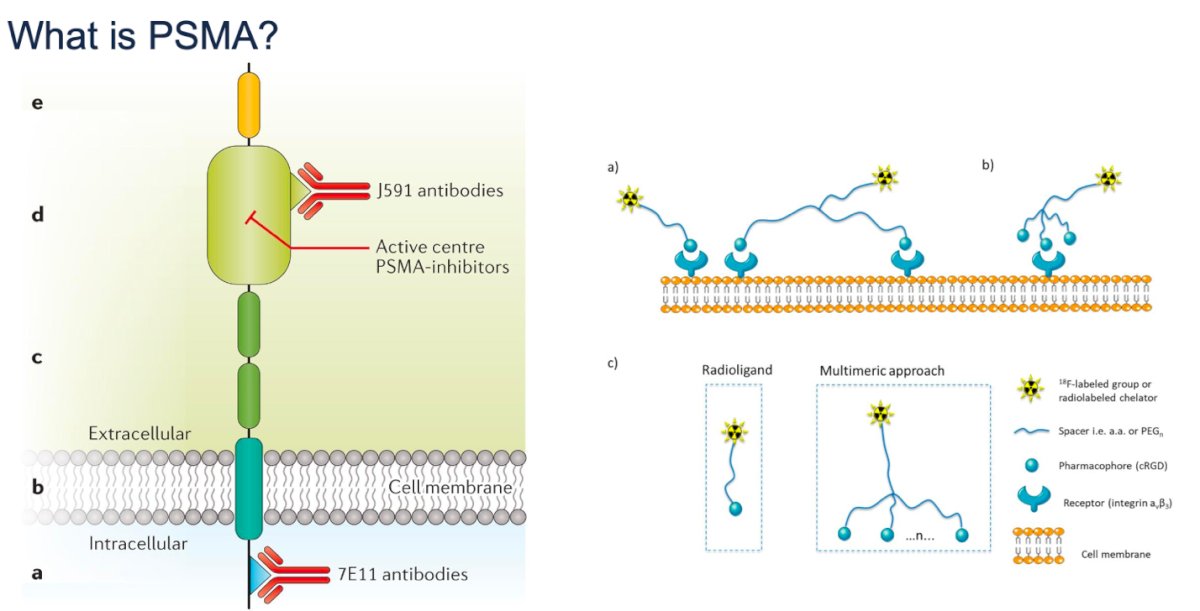
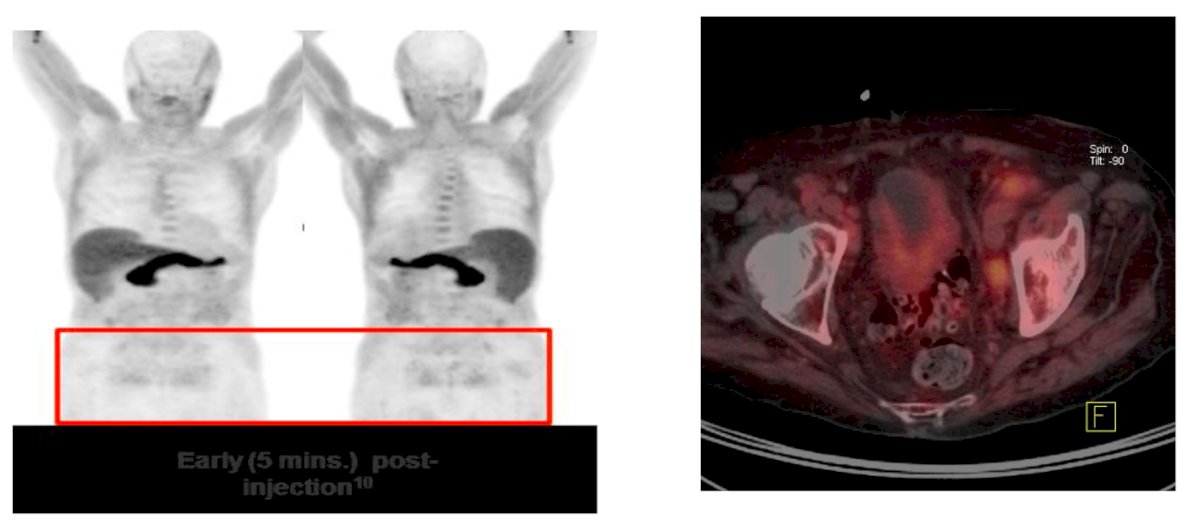
Dr. Gamie discussed ProstaScint, a diagnostic imaging agent that uses Indium-111-labeled capromab pendetide, a monoclonal antibody that targets an intracellular epitope of PSMA expressed on prostate epithelial cells. Once bound, the radiolabeled antibody allows for imaging of prostate cancer. Although innovative for its time, ProstaScint has limitations due to its intracellular binding site (requiring membrane compromise) and relatively low resolution. The image shows whole-body scans highlighting areas of radiotracer uptake and fusion imaging (CT/SPECT), indicating potential prostate cancer localization.
Moreover, androgen receptor (AR) signaling inversely correlates with PSMA expression in preclinical models. Treatment with androgens like testosterone or DHT suppresses PSMA levels, while androgen deprivation or AR inhibition increases PSMA expression, an effect that can be visualized and quantified using PET imaging with radiolabeled anti-PSMA antibodies like ⁶⁴Cu-J591 as shown below.4
The discovery of PSMA was based on its selective expression in prostatic tissues, as shown by reactivity with the monoclonal antibody 7E11-C5. This antibody demonstrated high binding to prostate cancer foci, metastases, benign prostatic hyperplasia, and normal prostate tissue, while showing no reactivity in non-prostatic tumors or normal human organs. In contrast, the 9H10-A4 antibody showed no such reactivity, highlighting the specificity of 7E11-C5 and supporting PSMA as a highly prostate-restricted target for imaging and therapy.
PSMA and PSA, both markers, show high positivity in normal prostate, benign prostatic hyperplasia (BPH), and prostate intraepithelial neoplasia (PIN). However, PSMA shows relatively higher expression in metastatic settings: lymph node (91%) and bone (100%), than PSA (94% and 57%, respectively). While PSA has a higher mean percentage of positive cells in most tissues, PSMA demonstrates more consistent detection in metastatic sites, noted Dr Gamie.5
Furthermore, PSMA expression intensity appears to correlate with Gleason score; in the same study, patients with Gleason 8–10 tumors exhibited the highest mean percentage of PSMA-positive cells (62%) and the highest stain index (161).5
Additionally, PSMA is expressed in the neovasculature of several non-prostatic malignancies, including bladder, kidney, and lung cancers, as illustrated below.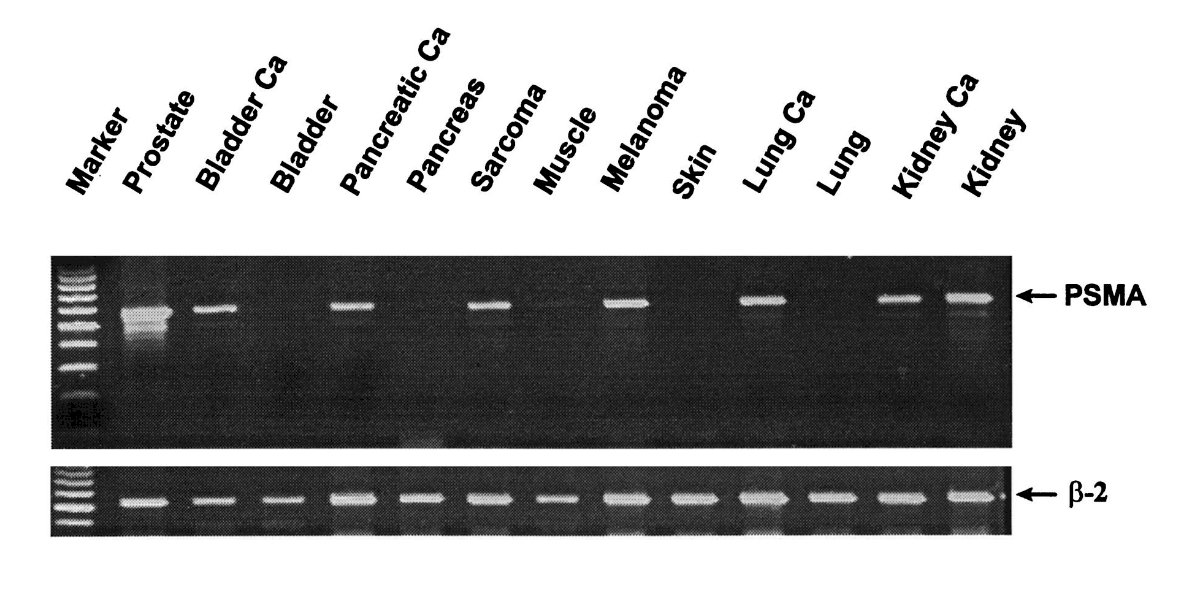
Higher PSMA expression at diagnosis has been associated with worse recurrence-free survival. In a study assessing oncological outcomes according to PSMA level at diagnosis, patients with no PSMA expression had a 5-year RFS of 88.2%, compared to 74.2% with low, 67.7% with medium, and 26.8% with high PSMA expression, supporting its potential role as a prognostic biomarker.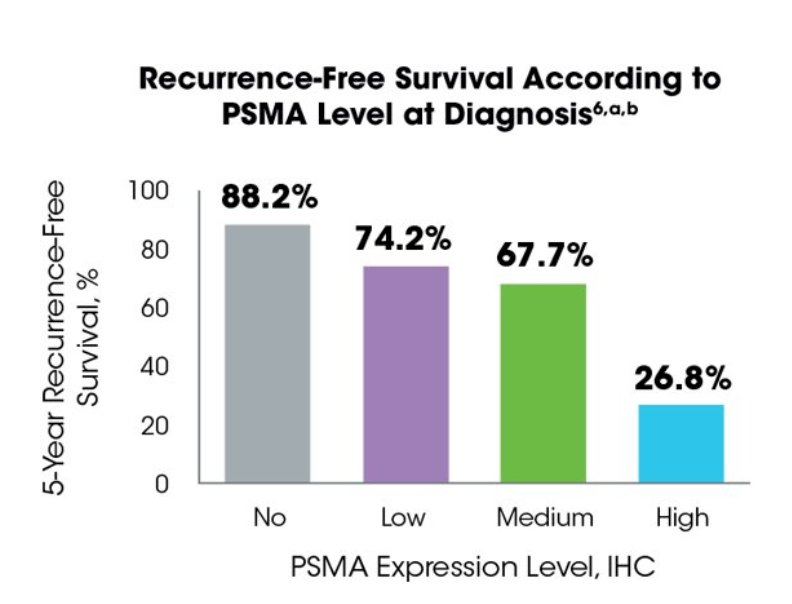
Various radiotracers can be used for prostate cancer imaging, with PSMA-based tracers demonstrating superior lesion detection compared to [¹⁸F]FDG and choline-based agents [¹⁸F]Choline and [11C] Choline.![Various radiotracers can be used for prostate cancer imaging, with PSMA-based tracers demonstrating superior lesion detection compared to [¹⁸F]FDG and choline-based agents [¹⁸F]Choline and [11C] Choline.](/images/com-doc-importer/220-interdisciplinary-gu-cancer-forum-2025/interdisciplinary-gu-cancer-forum-2025-impact-of-molecular-targeted-imaging-on-nmcrpc/image-7.jpg)
FDG PET/CT Scan
FDG PET/CT has limited sensitivity in prostate cancer due to typically low glucose metabolism in most tumors, but it can be useful in advanced or aggressive cases particularly in neuroendocrine or dedifferentiated disease where higher FDG uptake is observed.
 11C-CholinePET/CT Scan
11C-CholinePET/CT Scan
11C-Choline PET/CT was one of the earlier PET tracers used for prostate cancer imaging, particularly useful in detecting biochemical recurrence. It leverages increased cell membrane turnover and choline kinase activity in tumor cells. However, its limitations include relatively low sensitivity for low PSA disease, physiological uptake in benign prostatic hyperplasia and the liver, and a short half-life requiring an on-site cyclotron.

¹⁸F-Fluciclovine (Axumin) PET/CT is an FDA-approved imaging modality for detecting recurrent prostate cancer in patients with rising PSA after initial therapy. This synthetic amino acid analog targets amino acid transporters upregulated in prostate cancer cells. A key advantage is minimal urinary excretion, allowing for clearer pelvic imaging compared to other tracers. It is particularly useful in identifying recurrence in prostate/prostate bed and regional lymph nodes. However, its sensitivity declines at low PSA levels, and it lacks the specificity and lesion-to-background contrast of PSMA-based imaging
 +PSMA PET/CT Scan
+PSMA PET/CT ScanPSMA has physiologic tracer uptake in the salivary glands, liver, and kidneys. Despite this, PSMA PET/CT offers excellent sensitivity for detecting prostate cancer recurrence, as shown by the clear visualization of pelvic lymph node metastasis and local recurrence in the images below. The high tumor-to-background contrast makes PSMA PET/CT a valuable tool for precise localization of disease, even at low PSA levels. Moreover 18F labelled PSMA could be use as radioligand therapy.

PSMA PET/CT is gaining relevance in the initial staging of prostate cancer, enabling precise localization of intraprostatic lesions. This may inform lesion-targeted procedures by urologists and lesion-specific boost strategies by radiation oncologists. As molecular imaging becomes more integrated into early management, further research is needed to clarify its clinical utility and potential to personalize local treatment approaches.
Dr. Gamie further discussed emerging molecular imaging approaches, including [¹⁸F]-fluorodihydrotestosterone ([¹⁸F]FDHT) PET, which directly targets the androgen receptor. This modality holds promise as both a prognostic and predictive biomarker in metastatic castration-resistant prostate cancer (mCRPC), potentially offering real-time insights into AR expression and guiding therapy selection in advanced disease.![Dr. Gamie further discussed emerging molecular imaging approaches, including [¹⁸F]-fluorodihydrotestosterone ([¹⁸F]FDHT) PET, which directly targets the androgen receptor. This modality holds promise as both a prognostic and predictive biomarker in metastatic castration-resistant prostate cancer (mCRPC), potentially offering real-time insights into AR expression and guiding therapy selection in advanced disease.](/images/com-doc-importer/220-interdisciplinary-gu-cancer-forum-2025/interdisciplinary-gu-cancer-forum-2025-impact-of-molecular-targeted-imaging-on-nmcrpc/image-12.jpg)
Dr. Gamie also addressed the potential role of hybrid PSMA PET/MRI in initial prostate cancer staging. By combining the functional sensitivity of PSMA PET with the superior anatomical resolution of MRI, this modality may enhance lesion detection, improve local staging, and inform lesion-targeted approaches.

Theranostics PSMA-targeting ligand is used for both diagnostic imaging and targeted therapy. For diagnostics, PSMA ligands are labeled with imaging radionuclides such as gallium-68 or fluorine-18. For treatment, the same ligands are coupled to therapeutic radionuclides like lutetium-177 (¹⁷⁷Lu), allowing for selective delivery of cytotoxic radiation to PSMA-expressing cancer cells. Once bound, the radioligand is internalized, causing double-stranded DNA damage and cell death as illustrated below.
Radiation safety remains a critical consideration in theranostic applications. 177Lu emits both beta and low-energy gamma radiation, necessitating protective measures such as plastic shielding for beta particles and lead shielding for gamma emissions. With a half-life of 6.7 days, it offers logistical advantages.
Radioligand therapy currently used in the advanced mCRPC setting. However, as research progresses, there is growing interest in moving 177Lu-PSMA earlier in the disease course even potentially into the primary treatment setting. Ongoing trials aim to explore its integration alongside or in place of standard treatments such as surgery, radiation, or systemic therapy in high-risk or oligometastatic disease.

Dr. Gamie concluded the presentation by emphasizing the continuum of PSMA-based molecular imaging and therapy across all stages of prostate cancer care. From initial staging and assessment of PSMA expression using PSMA PET, to therapy with radioligands like 177Lu-PSMA-617, and through post-treatment imaging and long-term follow-up, this theranostic model enables precise, personalized management. He highlighted how dosimetry, efficacy monitoring, and safety assessments are all integrated into a single pathway, reinforcing the value of PSMA as both a diagnostic and therapeutic target in prostate cancer.
Presented by: Shereif H. Gamie, MD, PhD, Director, PET/CT - Molecular Imaging, Professor of Clinical Radiology – University of California, San Diego. San Diego, CA.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Interdisciplinary Genitourinary Cancer Forum 2025, between June 19 – 22, 2025, in St. Petersburg, Florida, United States
Related content: Theranostics in nmCRPC: From PSMA PET Imaging to Lutetium-177 Therapy - Sherief Gamie
Reference:
- Mohler JL, Antonarakis ES, Armstrong AJ, D’Amico AV, Davis BJ, Dorff T, et al. Prostate cancer, version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019;17(5):479–505.
- Cornford P, Bellmunt J, Bolla M, Briers E, De Santis M, Gross T, et al. EAU–EANM–ESTRO–ESUR–SIOG Guidelines on prostate cancer. Eur Urol. 2017;71(4):618–29.
- Cookson MS, Lowrance WT, Murad MH, Kibel AS. Castration-resistant prostate cancer: AUA guideline. J Urol. 2013;190(2):429–38.
- Evans MJ, Smith-Jones PM, Wongvipat J, Navarro V, Kim S, Bander NH, Larson SM, Sawyers CL. Noninvasive measurement of androgen receptor signaling with a positron-emitting radiopharmaceutical that targets prostate-specific membrane antigen. Proc Natl Acad Sci U S A. 2011 Jun 7;108(23):9578-82. doi: 10.1073/pnas.1106383108. Epub 2011 May 23. PMID: 21606347; PMCID: PMC3111331.
- Wright GL Jr, et al. Expression of prostate-specific membrane antigen in normal, benign, and malignant prostate tissues. Urol Oncol. 1995