(UroToday.com) The Interdisciplinary Genitourinary Cancer Forum 2025, held between June 19 – 21, 2025 held in St. Petersburg, Florida, United States, was host to the Prostate Cancer Session 3: Androgen Deprivation Therapy. Dr. Robert Reiter discussed neoadjuvant management strategies for high-risk prostate cancer.
The goals of neoadjuvant studies are many, beginning with the establishment of baseline clinical efficacy of a drug or combination of drugs. These trials assess key clinical endpoints such as pathologic complete or near-complete response (minimal residual disease), whether a drug influences biochemical recurrence-free survival, and if it affects metastasis-free survival. Additionally, they offer a valuable platform for translational endpoints, enabling the investigation of pharmacodynamic and pharmacokinetic endpoints including target presence, drug delivery to the target, and on-target drug effects. Importantly, neoadjuvant studies allow researchers to build upon preclinical findings, test adaptive resistance mechanisms, and evaluate co-targeting strategies using both pathologic and clinical efficacy outcomes. Moreover, these trials are the first opportunity for in vivo in-human target experiments to test different hypotheses.
Dr. Reiter explained that doublet therapy with ADT plus an ARPI was originally developed for second-line treatment in mCRPC, and later advanced to the M0 biochemical recurrence (BCR) space. He posed the question of whether these therapies could be moved even earlier, into the neoadjuvant setting. He noted that there have been numerous attempts to introduce hormonal therapies earlier for patients with high-risk localized disease, with many of the trials aiming to assess pathologic complete response (pCR) as the primary endpoint.
Dr. Reiter noted that increasing exposure to androgen pathway inhibitors, whether in doublet or triplet combinations, has consistently led to higher rates of pathologic complete response (pCR) and minimal residual disease (MRD) across most trials, regardless of the agents used. He emphasized that this pattern supports a treatment-response relationship, with more intensive or prolonged therapy driving deeper responses. The critical next step, he stated, is to determine whether these pathologic responses correlate with longer-term oncologic outcomes such as metastasis-free survival (MFS). The table below summarizes PSA and pathologic outcomes across multiple neoadjuvant trials.
A recent paper from Brigham and Women’s Hospital addressed whether pathologic endpoints from neoadjuvant studies, such as pCR or MRD can serve as valid surrogates for clinically meaningful outcomes like MFS or overall survival (OS). In a pooled analysis of five neoadjuvant trials involving 218 patients with unfavorable intermediate- or high-risk prostate cancer, patients received 6 months of ADT plus at least one ARPI, with a subset undergoing both neoadjuvant and adjuvant therapy for a total of one year. The primary endpoint was metastasis-free survival (defined as extra-pelvic disease), while pathologic endpoints included a pCR rate of 11% (24 patients) and MRD also in 11% of patients.1
Looking at predictors of failure for MFS, this study reported that patients with 2–3 high-risk features (e.g., Gleason ≥9, cT3+, PSA ≥20 ng/mL) had a significantly higher risk of metastasis compared to those with only unfavorable intermediate-risk disease. Specifically, these high-risk patients exhibited a 50% probability of developing metastases within 5 to 6 years, underscoring the importance of early risk stratification and potential intensification of therapy in this subgroup.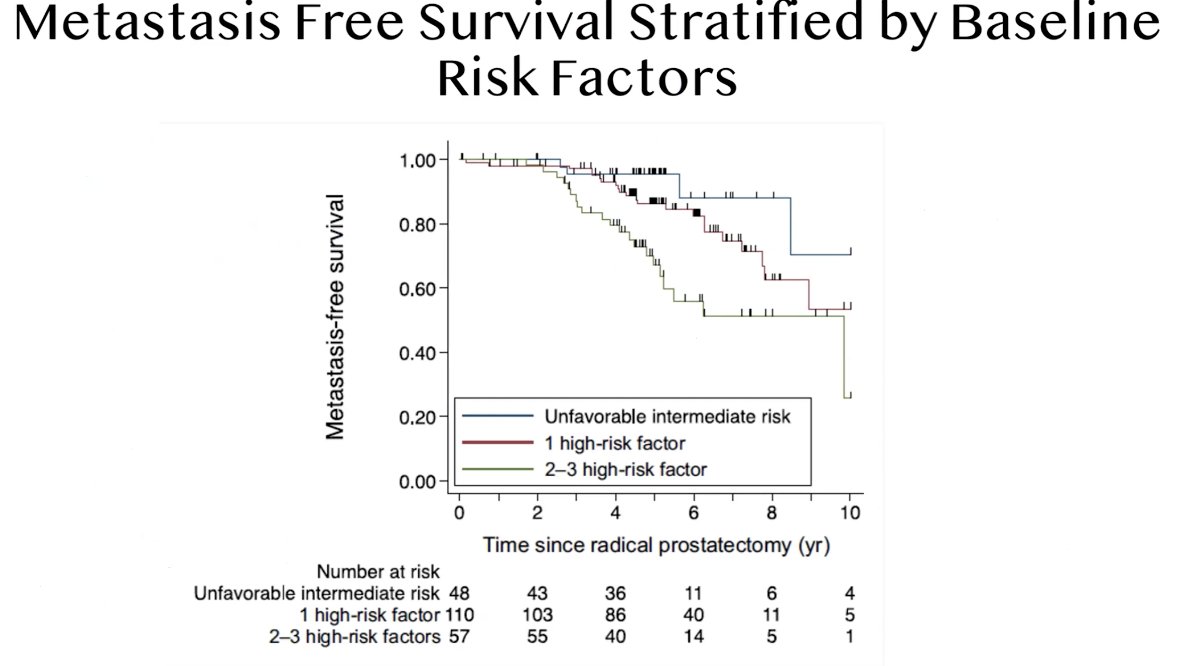
Moreover, residual cancer burden (RCB) was found to be prognostic for metastasis-free survival, with data supporting pathologic response as a potential surrogate for both MFS and overall survival. Patients who achieved a pCR or nearly complete response (RCB-1) had only a 10% risk of developing metastases over a 10-year period. In contrast, those with minimal response to neoadjuvant therapy classified as RCB-2 or RCB-3 had significantly worse outcomes, highlighting the importance of achieving a strong pathologic response in the neoadjuvant setting.1
Dr. Reiter discussed the design of the ongoing Phase III PROTEUS trial, which evaluates the role of apalutamide in combination with ADT in the neoadjuvant and adjuvant settings for patients undergoing radical prostatectomy (RP). The study includes patients with high-risk or locally advanced prostate cancer, randomized 1:1 to receive either apalutamide + ADT or ADT + placebo across six preoperative cycles. Postoperatively, patients continue on the same assigned treatment through cycle 12.
After treatment completion, patients are monitored every 3 months until biochemical failure, defined as two consecutive rises in PSA with the second value ≥0.2 ng/mL. The study’s co-primary endpoints are metastasis-free survival (MFS) and pathologic response, including complete and near-complete responses. The study has not been reported yet, but hopefully we will see results soon.

The GUNS (Genomic Umbrella Neoadjuvant Study) is a precision medicine trial enrolling patients with high-risk localized prostate cancer (HRLPCa) and assigning them to treatment arms based on tumor genomic profiling. The primary endpoint is minimal residual disease (MRD <5 mm residual cancer burden). Patients initially receive 8 weeks of LHRHa + apalutamide, followed by assignment to one of four sub-protocols based on molecular alterations.2
- AR-high tumors without targeted alterations (SPOP, T2E, FOXA1), randomized to LHRHa + Apalutamide (APA) vs. LHRHa + APA + ABI;
- Tumors with loss of tumor suppressors (PTEN, RB1, TP53), receiving LHRHa + ABI ± docetaxel;
- DNA damage repair-deficient tumors treated with LHRHa + ABI + niraparib (PARPi); and
- Immunogenic tumors (MMRd or CDK12-altered) treated with LHRHa + APA + atezolizumab. This design aims to match therapies to genomic features to optimize response.

Early results from the GUNS trial demonstrate the feasibility of conducting a genomic umbrella study in high-risk localized prostate cancer. Among 130 patients, genomic profiling was successfully performed on 113 pre-treatment biopsies (~87%), with the remainder being non-evaluable. The most common alterations included TMPRSS2-ERG fusions (31%), FOXA1 alterations (23%), SPOP alterations (13% mostly SP1 subtype), TP53 mutations (14%), PTEN loss (12%), and BRCA2 mutations (9%).
These findings highlight the practicality of stratifying patients based on distinct molecular alterations, supporting the implementation of genomically driven neoadjuvant trial designs. The distribution of actionable mutations also provides a framework for testing targeted therapies within defined molecular subgroups.
Early findings from the GUNS trial in patients with AR-activated tumors specifically those harboring SPOP mutations or FOXA1 alterations suggest that triplet neoadjuvant therapy (ARPI + abiraterone + ADT) may yield superior responses compared to doublet therapy. Patients receiving triplet therapy showed a significantly higher rate of MRD at 43% versus 13% with doublet therapy (p = 0.012; OR = 5.9), although no pathologic complete responses (pCR) were observed in either group. These results support the potential benefit of intensifying neoadjuvant hormonal therapy in genomically defined AR-driven prostate cancers.
Lastly, Dr Reiter discussed the Lutectomy trial, led in Australia, which is a neoadjuvant study evaluating the role of 177Lu-PSMA-617 in patients with high-risk localized prostate cancer. Eligible participants include men with biopsy-proven prostate cancer and high-risk features such as PSA >20 ng/mL, ISUP grade group 3–5, cT2 or higher disease, and/or N1 nodal involvement, without distant metastases, but high PSMA uptake (SUVmax >20) on PSMA PET imaging.
The study enrolled 20 men, with the first 10 receiving a single cycle and the next 10 receiving two cycles of 5 GBq 177Lu-PSMA-617, spaced 6 weeks apart. After treatment, patients undergo a second PSMA PET scan followed by radical prostatectomy with pelvic lymph node dissection. The primary endpoint is dosimetry, measuring the absorbed radiation dose to the tumor. Secondary endpoints include imaging and biochemical responses, pathological outcomes, surgical safety, and quality of life measures.

Early results from the Lutectomy trial showed promising PSA responses, with several patients achieving a PSA90 decline. Notably, patients who received two cycles of ^177Lu-PSMA-617 demonstrated greater PSA reductions compared to those who received a single cycle. One patient achieved a near-complete pathologic response, suggesting potential tumor eradication prior to surgery.3
Although these are still early findings from the first trial of its kind in this neoadjuvant setting, they underscore the feasibility and potential of theranostic approaches for high-risk localized prostate cancer. Based on these encouraging results, a follow-up trial is now being planned at UCLA to further investigate the efficacy and role of LuPSMA in this context.
Dr. Reiter concluded his presentation with the following key points:
- The role of neoadjuvant or adjuvant ADT/ARPI in high-risk localized prostate cancer remains unclear.
- Ongoing trials such as PROTEUS are evaluating whether pathologic response can serve as a surrogate for metastasis-free survival and are expected to provide high-level evidence to guide clinical decision-making.
- Neoadjuvant studies represent a powerful platform to evaluate novel drug combinations in genetically or genomically defined patient subsets. The field eagerly awaits results from ongoing efforts like the GUNS trial.
- The integration of theranostics (Lu-PSMA) with surgery is an exciting frontier. Although still in its early stages, this approach holds promise for the future of personalized prostate cancer care.
Presented by: Robert Reiter, MD, MBA, Chief of Urologic Oncology and Assistant Dean for Innovation at Geffen School of Medicine at UCLA, Los Angeles, California.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Interdisciplinary Genitourinary Cancer Forum 2025, between June 19 – 22, 2025 in St. Petersburg, Florida, United States
Related content: Neoadjuvant and Adjuvant ARPIs in High-Risk Localized Prostate Cancer - Robert Reiter
Reference:
- Ravi P, Kwak L, Acosta AM, Rastogi S, Xie W, Abdelnaser A, Einstein DJ, Chang P, Wagner AA, McKay RR, Kibel AS, Taplin ME. Long-term Outcomes and Prognostic Impact of Residual Cancer Burden After Intensified Neoadjuvant Therapy in High-risk Prostate Cancer. Eur Urol. 2025 Jun;87(6):643-650. doi: 10.1016/j.eururo.2025.01.015. Epub 2025 Feb 7. PMID: 39920004.
- Sayyid RK, Fleshner NE. Lessons from the ACDC-RP trial: Clinical trial design for radical prostatectomy neoadjuvant therapy trials. Oncotarget. 2024 Sep 30;15:660-661. doi: 10.18632/oncotarget.28648. PMID: 39347713; PMCID: PMC11441411.
- Eapen RS, Buteau JP, Jackson P, Mitchell C, Oon SF, Alghazo O, McIntosh L, Dhiantravan N, Scalzo MJ, O'Brien J, Sandhu S, Azad AA, Williams SG, Sharma G, Haskali MB, Bressel M, Chen K, Jenjitranant P, McVey A, Moon D, Lawrentschuk N, Neeson PJ, Murphy DG, Hofman MS. Administering [177Lu]Lu-PSMA-617 Prior to Radical Prostatectomy in Men with High-risk Localised Prostate Cancer (LuTectomy): A Single-centre, Single-arm, Phase 1/2 Study. Eur Urol. 2024 Mar;85(3):217-226. doi: 10.1016/j.eururo.2023.08.026. Epub 2023 Oct 26. PMID: 37891072.