(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress was host to a radioligand therapeutics proffered paper session. Dr. Karolien Goffin discussed the previously presented trials by Drs. Kim Chi and Jeremie Calais:
- A Randomized Phase II study of 177Lu-PSMA-617 versus Docetaxel in Patients with Metastatic Castration-resistant Prostate Cancer (mCRPC) and PSMA-positive Disease: Canadian Cancer Trials Group (CCTG) Study PR.21
- 177Lutetium-PSMA Therapy Neoadjuvant to Stereotactic Ablative Radiotherapy for Recurrent Oligo-metastatic Hormone Sensitive Prostate Cancer: A Randomized Phase 2 Trial (LUNAR)
She noted that these two phase II studies evaluated radioligand therapy in different clinical settings along the prostate cancer treatment spectrum. These studies complement existing phase 2/3 data on the use of 177Lu-PSMA radioligand therapy in prostate cancer.
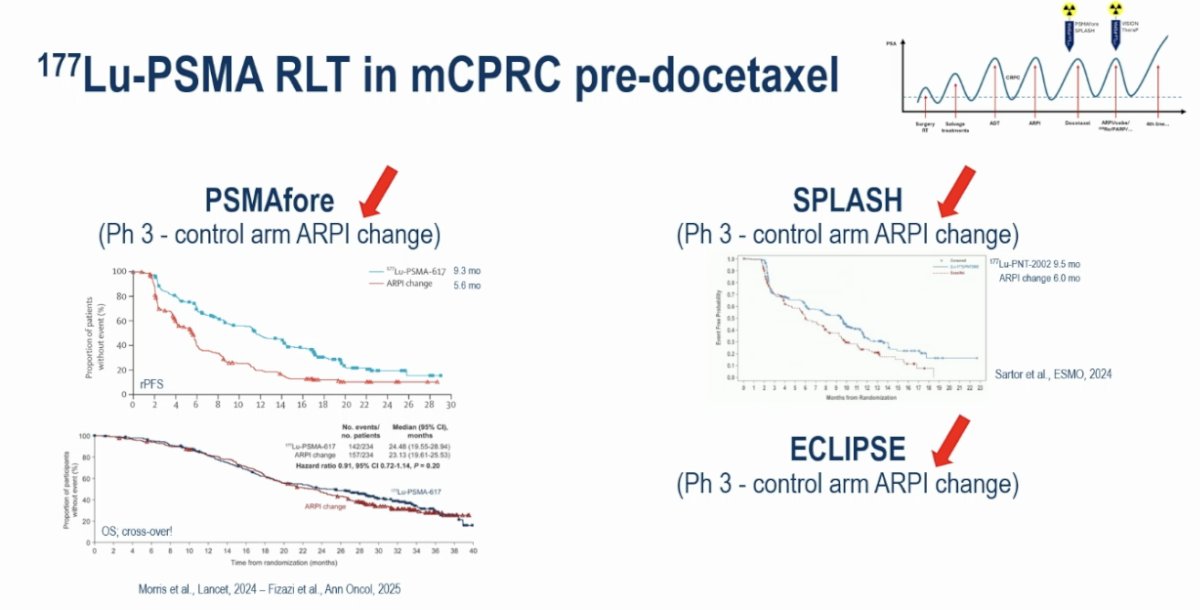
In the phase III PSMAfore study, the use of 177Lu-PSMA-617 in the pre-docetaxel, post-androgen receptor pathway inhibitor (ARPI) setting was associated with a significant radiographic progression-free survival (rPFS) benefit (median: 9.3 vs 5.6 months; HR: 0.41, p<0.001), compared to an ARPI switch. This rPFS benefit, however, did not translate into an overall survival benefit.1 Consistent results were observed in similarly designed trials (SPLASH and ECLIPSE),2,3 all of which included an ARPI switch control arm. However, Dr. Goffin argued that this is no longer a standard of care option for mCRPC patients who progress with an ARPI. Such patients typically receive docetaxel after failing an ARPI.
This leads us to the CCTG PR21 trial, which was an open-label, randomized, phase II trial that randomized eligible patients 1:1 to:
- 177Lu-PSMA-617 7.4 GBq IV every 6 weeks x 6 cycles
- Docetaxel 75 mg/m2 every 3 weeks x 12 cycles
The key eligibility criteria were as follows:
- Chemotherapy-naïve mCRPC progressing after an ARPI
- PSMA PET positive disease (i.e., uptake >liver)
- Excluded if >50% of extra-osseous lesions or >5 cm soft tissue lesions were PSMA negative
199 patients were randomized to 177Lu-PSMA-617 (n=100) or docetaxel (n=99). Thirty-eight patients crossed over from 177Lu-PSMA-617 to docetaxel versus 56 from docetaxel to 177Lu-PSMA-617.
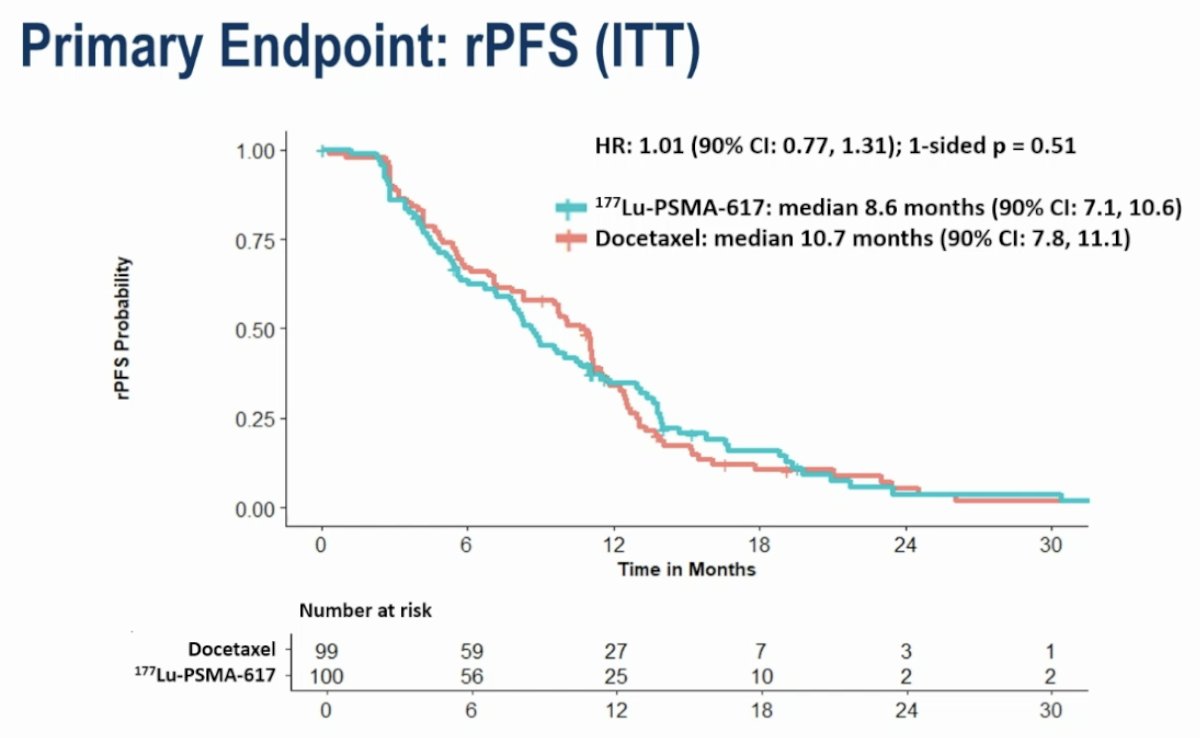
From an efficacy standpoint, there was no difference in rPFS between the two arms. The median rPFS values were 8.6 and 10.7 months for the 177Lu-PSMA-617 and docetaxel arms, respectively (HR: 1.01, 95% CI: 0.77–1.31, p=0.51).
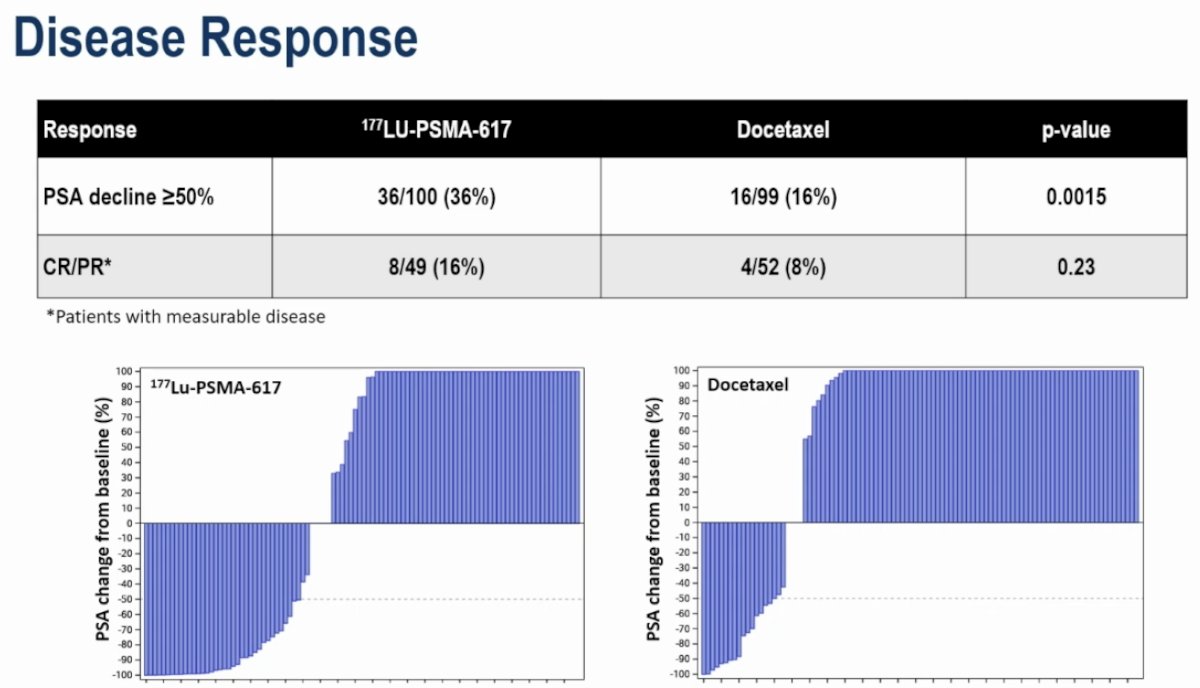
Disease response rates favored 177Lu-PSMA-617:
- PSA50 response: 36% vs 16% (p=0.0015)
- Complete or partial response: 16% vs 8% (p=0.23)
Notably, OS favored patients initially randomized to the docetaxel arm (HR: 1.64, 95% CI: 1.14–2.35, p=0.02). The median OS were 14.3 and 18.2 months, respectively, in favor of initial randomization to docetaxel (i.e., docetaxel 177Lu-PSMA-617):
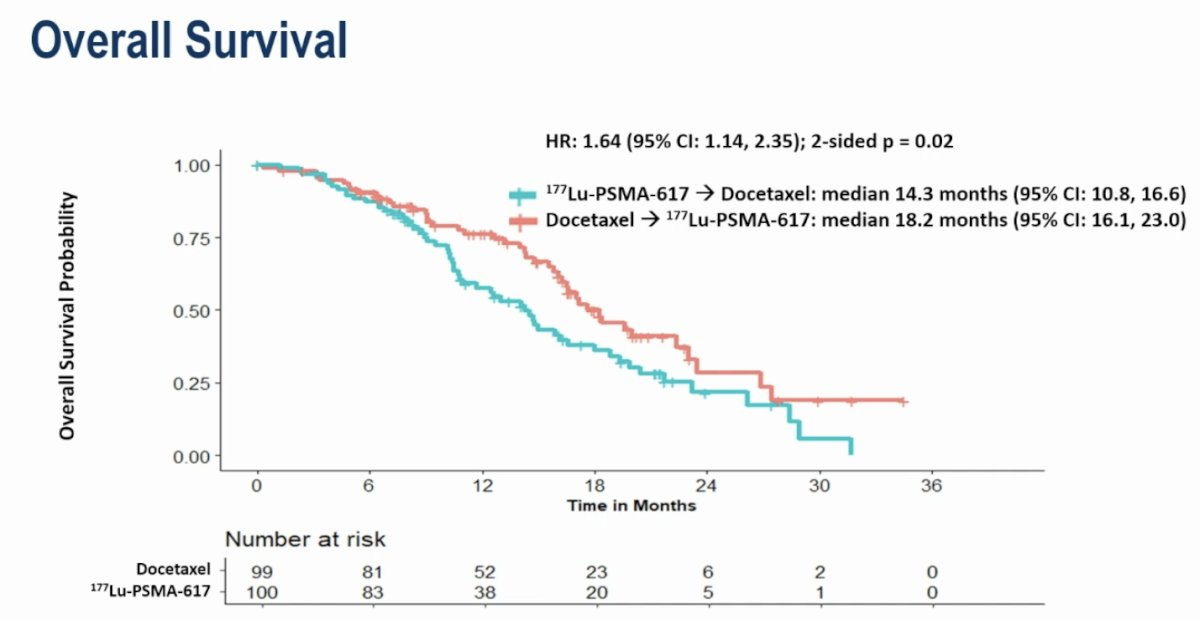
Were these OS differences due to the fact that a higher number of patients crossed over from docetaxel to 177Lu-PSMA-617 arm (n=56) versus 177Lu-PSMA-617 to docetaxel (n=38)? Did a higher number of patients in the docetaxel arm receive further treatment lines? How do we select the patients best appropriate for docetaxel as 2nd line treatment following an ARPI? Many questions remain unanswered.
Dr. Goffin noted that the PSMA-based inclusion criteria were different than those for PSMAfore. PSMA PET positivity was defined as uptake greater than that of the liver, with patients excluded if >50% of extra-osseous lesions or >5 cm soft tissue lesion were PSMA negative. Notably, however, 98% of patients would have been VISION eligible based on the radiographic findings.
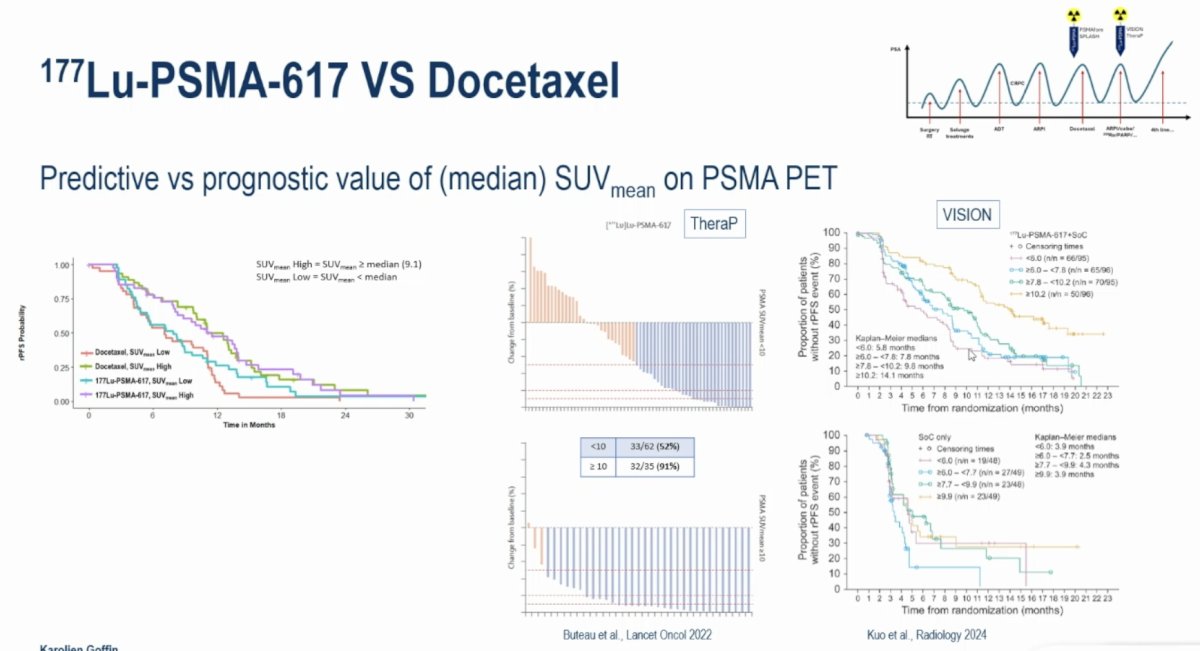
The median SUVmean was prognostic, but not predictive for rPFS. As seen below, patients with SUVmean high disease had worse rPFS outcomes, compared to SUVmean low disease, in both treatment arms. Furthermore, patients with SUVmean high disease did not derive a preferential benefit from 177Lu-PSMA-617 therapy, confirming that SUVmean was not predictive in this setting. This is in contrast to previously published data from VISION and TheraP that have demonstrated the predictive value of PSMA SUVmean.4,5
Next, moving on to discuss the LUNAR trial presented by Dr. Calais, this was a phase II trial that evaluated whether adding 177Lu-PSMA-PNT2002 to stereotactic body radiotherapy (SBRT) can prolong PFS in patients with oligometastatic, recurrent hormone-sensitive prostate cancer. Ninety patients with 1-5 PSMA PET–positive lesions were randomized 1:1 to receive either SBRT alone or two cycles of 177Lu-PNT2002 followed by SBRT.
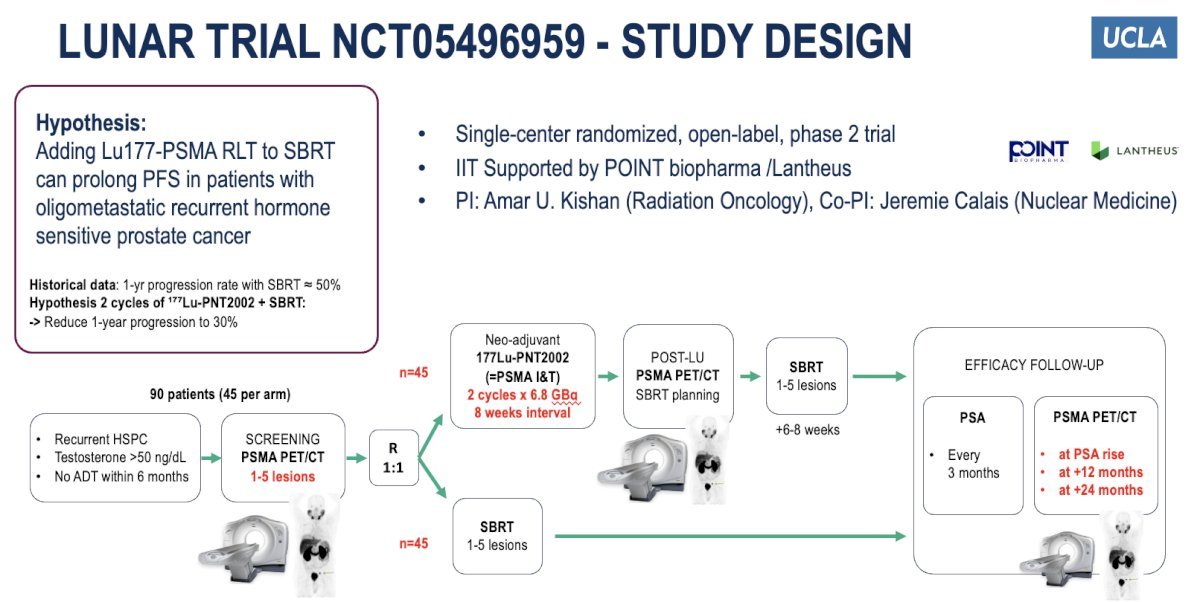
A PSA decline was observed in 71% of patients receiving 2 cycles of 177Lu-PNT2002, compared to 52% of patients in the SBRT only arm. She argued that PSMA PET/CT should be the imaging modality of choice when selecting patients for MDT, as 69% and 76% of patients in the control and experimental arms had no evidence of metastases on conventional imaging (cN0M0).
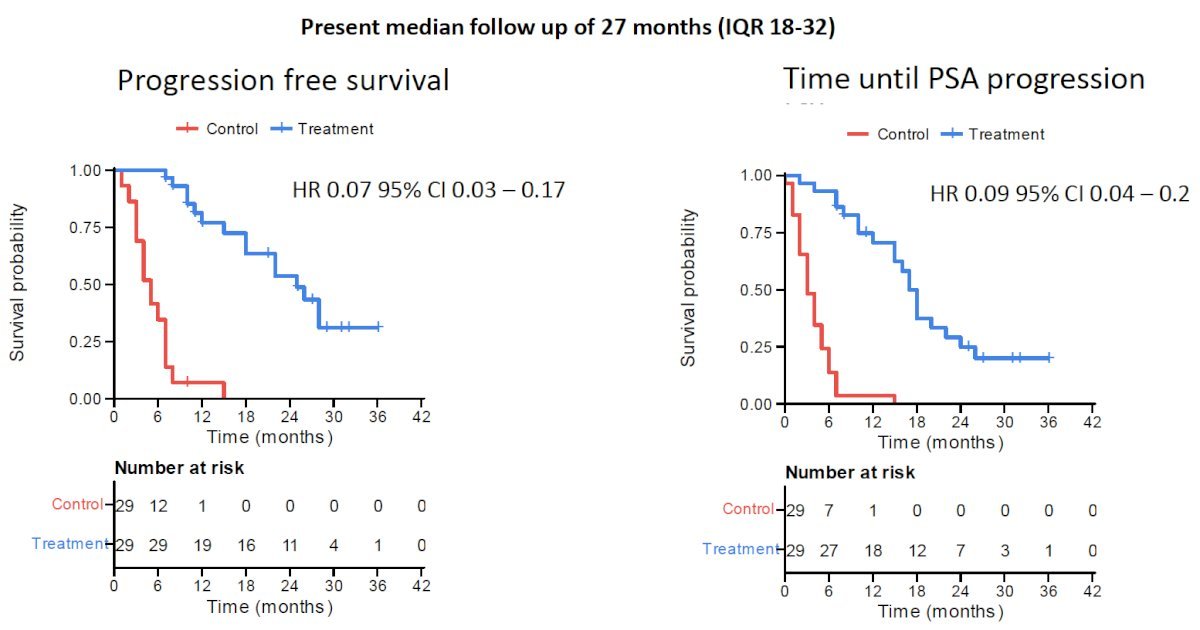
A similar trial in this space is the BULLSEYE trial that was presented at the 2025 ASCO Annual Meeting. This was an international, open-label, randomized trial of 2 (+2) cycles of 7.4 GBq 177Lu-PSMA-617 versus ‘standard of care’ of watchful waiting in patients with oligometastatic (≤5 lesions on PSMA PET) hormone-sensitive prostate cancer with a PSA doubling time ≤6 months. At a median follow-up of 27 months, both PFS (HR: 0.07, 95% CI: 0.03–0.17) and time until PSA progression (HR: 0.09, 95% CI: 0.04–0.2) favored the 177Lu-PSMA-617 arm:
While the LUNAR trial suggests that the addition of neoadjuvant 177Lu-PSMA to SBRT provides a 10-month gain in median PFS and hormone therapy-free survival with limited toxicity, important questions/limitations remain:
- What is the long-term benefit with regard to hard endpoints, such as OS?
- ‘How much’ treatment should oligometastatic HSPC patients receive?
- Can we incorporate genetic biomarkers, clinical parameters, and imaging findings to guide risk-adapted treatment intensification
- What is the long-term toxicity of Lu-PSMA when administered in earlier settings?

Presented by: Karolien Goffin, MD, PhD, Professor, Department of Nuclear Medicine, University Hospitals Leuven, KU Leuven, Leuven, Belgium.
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial. Lancet. 2024;404(10459):1227–1239.
- Sartor AO, Chi KN, Tagawa ST, et al. Efficacy of 177Lu-PNT2002 in PSMA-positive metastatic castration-resistant prostate cancer following progression on an androgen-receptor-pathway inhibitor (SPLASH): a phase 3, randomised, open-label trial. ESMO 2024; LBA65.
- Mutevelic S, Patterson M, Gleason D, et al. ECLIPSE: 177Lu-PSMA-I&T for metastatic castration-resistant prostate cancer—a phase 3, multicentre, open-label, randomised study. J Clin Oncol. 2025;43(4):579-584.
- Kuo PH, Morris MJ, Hesterman J, et al. Quantitative ⁶⁸Ga-PSMA-11 PET and clinical outcomes in metastatic castration-resistant prostate cancer following ¹⁷⁷Lu-PSMA-617 (VISION Trial). Radiology. 2024;312(2):e233460.
- Buteau J, Kratochwil C, Kuo P, et al. ¹⁷⁷Lu-PSMA-617 plus standard care versus standard care alone for metastatic castration-resistant prostate cancer (TheraP): a randomised, open-label, phase 2 trial. Lancet Oncology. 2022; 23(11):1389-1397.
- Privé BM, Noordzij W, Muselaers CHJ, et al. Lutetium-177-PSMA-617 in oligo-metastatic hormone-sensitive prostate cancer (BULLSEYE trial). J Clin Oncol. 2025;43(16_suppl):5009.