(UroToday.com) The 2025 ESMO annual meeting featured a metastatic castration-resistant prostate cancer (mCRPC) session and a presentation by Dr. Deborah Mukherji discussing optimized use of endocrine therapies and chemotherapies in mCRPC. Are we optimizing therapy for men with metastatic hormone sensitive prostate cancer (mHSPC)? Unfortunately, we are not, according to Dr. Mukherji. In a 2025 study from Rivas et al.1 assessing health records, insurance claims, and cancer registries from eight European and North American databases, 69,680 mHSPC patients were identified, of whom 71% presented with synchronous mHSPC. Patients aged 70–79 years were most often treated with ADT monotherapy or ADT + androgen receptor pathway inhibitors, whereas those aged 60–69 years more frequently received ADT + chemotherapy or ADT + androgen receptor pathway inhibitors + chemotherapy. From 2016 through 2020, the adoption of androgen receptor pathway inhibitors-based combinations rose steadily, use of ADT + chemotherapy declined, and ADT monotherapy remained stable:
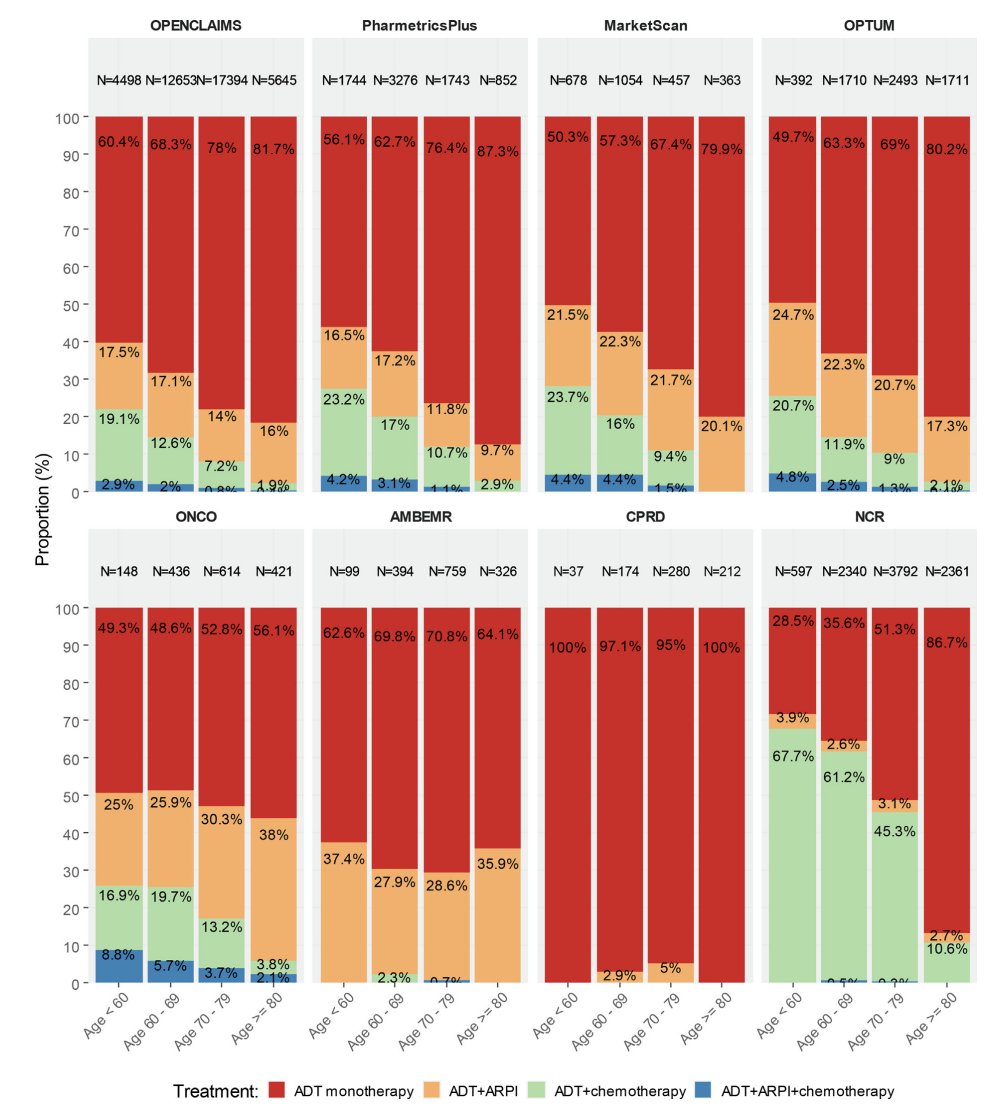
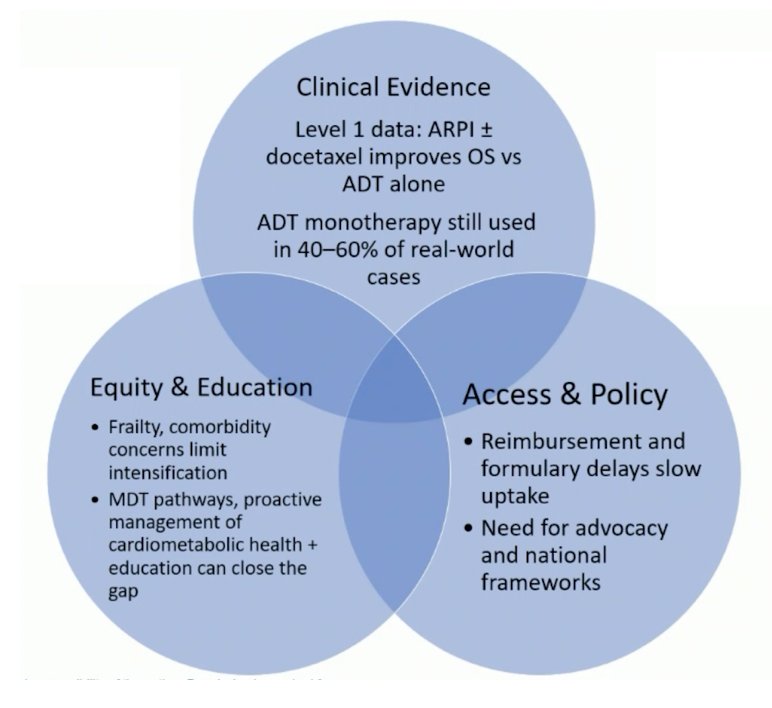
However, Dr. Mukherji emphasized that in 2020, ADT monotherapy use was still >50% in this study. There are multiple options for treatment intensification beyond ADT alone with level 1 evidence. How can we do better for men with mHSPC? We need to integrate evidence, access, and equity for maximal survival benefit and quality of life:
Dr. Mukherji notes that there is a spectrum of mCRPC presentations:
- Sustained responders: slowly rising PSA
- Oligoprogressive disease: is stereotactic body radiotherapy an option for these patients?
- Progression of disease requiring a change in therapy:
- Androgen receptor pathway inhibitor (if ADT alone)
- Docetaxel or cabazitaxel
- PSMA positive metastases: Lu-PSMA
- Symptomatic bone only disease: radium-223 +/- enzalutamide
- BRCA mutation: olaparib, rucaparib, niraparib + abiraterone, talazoparib + enzalutamide
- HRR mutation (non-BRCA): olaparib, talazoparib + enzalutamide
- Pembrolizumab if MSI-H
- Rapid progression: aggressive variant or neuroendocrine transformation
- Chemotherapy: cabazitaxel + carboplatin
- Platinum + etoposide
- Clinical trials
Importantly, there is a difference in the clinical trial population of mCRPC patients and those we are seeing in the real-world setting. Patients in clinical trials are (i) younger (median age of 67-69 years), (ii) ECOG performance status 0-1, (iii) predominantly Western, white cohorts, (iv) have been on limited prior therapies (largely ADT alone), and (v) have fewer cardiovascular/metabolic risks. The current real-world population of men with mCRPC are (i) older (median age 74-77 years), (ii) ethnically diverse, (iii) pre-treated, androgen receptor pathway inhibitor resistant, and (iv) at higher risk of cardio-metabolic toxicity.
With regards to sequencing therapies on progression to mCRPC in androgen receptor pathway inhibitor experience patients, the options depend on:
- Treatment received for mHSPC and the response to therapy
- Disease trajectory and symptomatic burden
- Patient co-morbidities, preferences, and patient access
- Biomarkers: genomic, imaging, etc
The aim of optimizing the use of endocrine therapies and chemotherapies in mCRPC is sequencing of active, survival-prolonging therapy, keeping men as well as possible, as long as possible. This includes several key points:
- Imaging + response assessment: we need to be aware of limitations of PSA, conventional imaging, PSMA PET/CT, and whole-body MRI
- Toxicity management: using bone targeted therapy, active management of cardio-metabolic risks, and encouraging exercise
- Genomic biomarkers: HRR mutations, MSI-H/tumor mutational burden, and tumor agnostic biomarkers
- Access: healthcare system specific, engaging in advocacy, and being aware of financial toxicity
At the APCCC consensus conference, the experts were asked the following question: For the majority of patients with mCRPC who have been tested and no DDR alteration was identified, what is your treatment recommendation in the first line setting when they have received ADT + androgen receptor pathway inhibitor for mHSPC? 88% responded with docetaxel, 6% with Lu-PSMA, 4% with an alternative androgen receptor pathway inhibitor, 1% with radium-223, and 1% with adding a PARP inhibitor to the current therapy or changing to an alternate androgen receptor pathway inhibitor + PARP inhibitor. Dr. Mukherji notes that this polling was in April 2024, prior to PSMAfore2 approval, PEACE 33 data, and TALAPRO-2 overall survival data.4
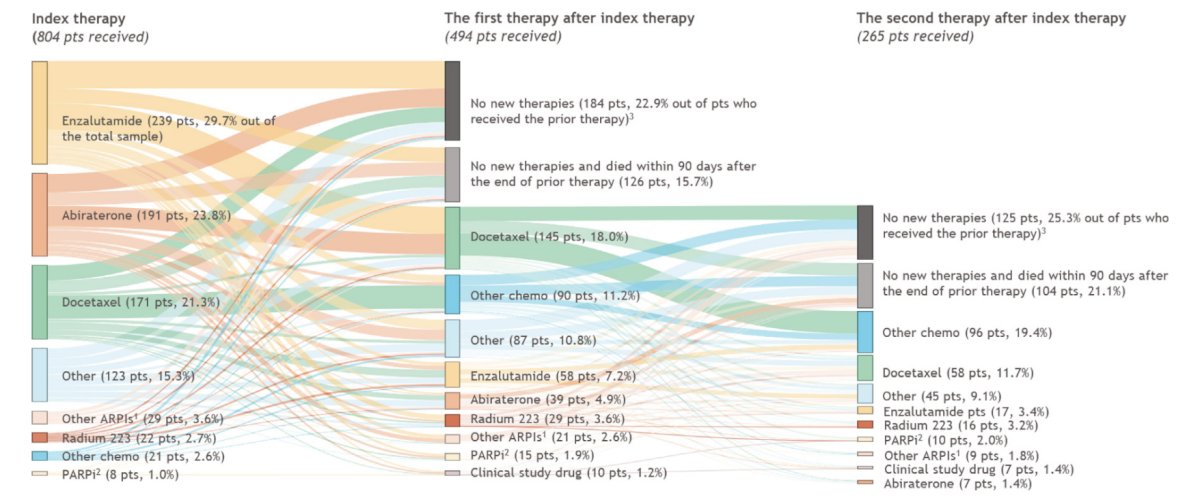
In 2024, Narayan et al.5 performed a retrospective, observational study of androgen receptor pathway inhibitor-experienced patients with mCRPC from the Flatiron database. The study design is highlighted as follows:

Among 804 androgen receptor pathway inhibitor-experienced mCRPC patients, 459 patients (57.1%) received another androgen receptor pathway inhibitor as their index therapy and 192 (23.9%) received chemotherapy as their index therapy, with 22.9% of the patients who received prior therapy receiving no new therapies:
In the overall population, median time on the index therapy and median time from index therapy to next therapy were 4.1 and 6.2 months, respectively. Docetaxel had the lowest time on therapy (median 3.5 months) compared to enzalutamide (median 4.3 months), and abiraterone (median 4.0 months):
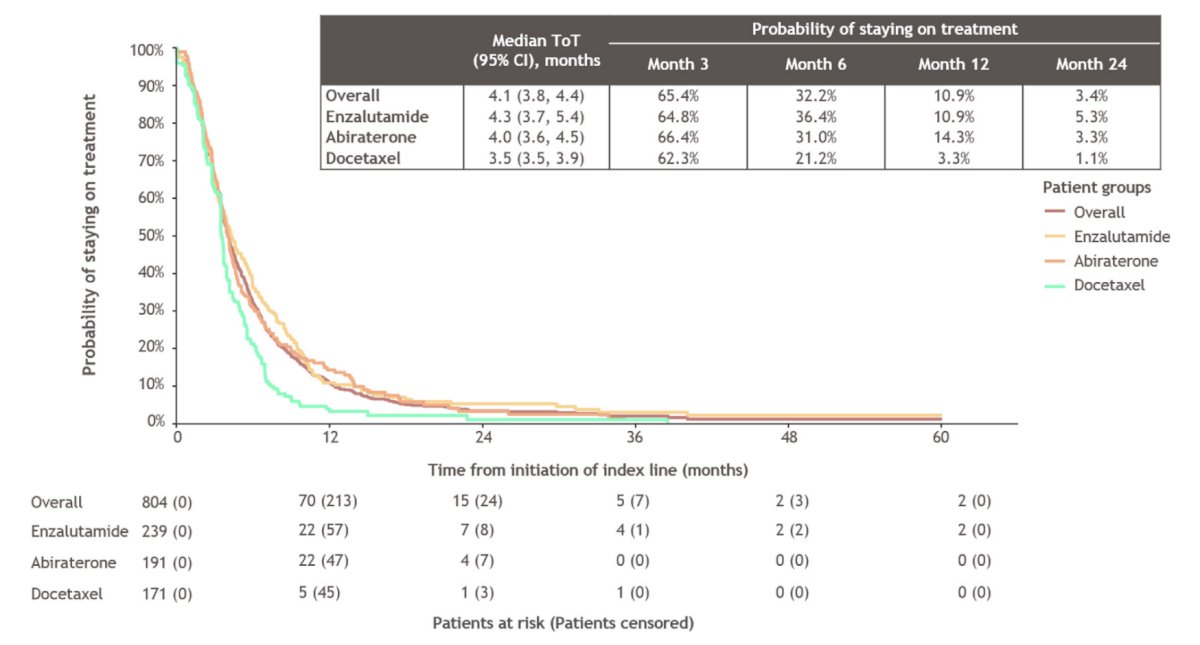
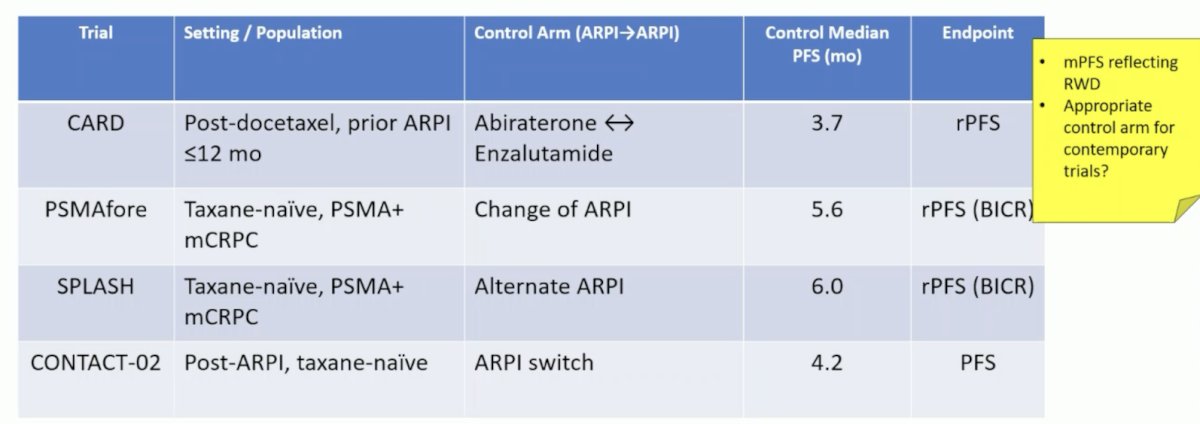
Additionally, Dr. Mukherji emphasized that the median progression free survival with a switch to an alternative androgen receptor pathway inhibitor or docetaxel was less than 4.5 months, and only 1/3 of patients were still on their second line of therapy at 6 months. Is an androgen receptor pathway inhibitor to androgen receptor pathway inhibitor switch an appropriate control arm for contemporary mCRPC trials?
Is there a role for stereotactic body radiotherapy in mCRPC? There are two trials in the oligometastatic mCRPC space in patients starting an androgen receptor pathway inhibitor:
- ARTO trial:6 a phase II randomized trial assessing abiraterone + stereotactic body radiotherapy versus abiraterone alone. The PSA50 was 92% versus 80%, and the progression free survival hazard ratio was 0.35 (95% CI 0.21-0.57) favoring abiraterone + stereotactic body radiotherapy
- GROUQ-PCS 9 trial:7 a phase II randomized trial of enzalutamide + stereotactic body radiotherapy versus enzalutamide alone. The median radiographic progression free survival was 4.6 years versus 2.3 years (HR 0.48, 95% CI 0.27-0.86) enzalutamide + stereotactic body radiotherapy.
There is also one trial for oligoprogressive mCRPC among patients already on an androgen receptor pathway inhibitor. The TRAP trial8 is a phase II prospective trial of stereotactic body radiotherapy to progressing sites on ADT + androgen receptor pathway inhibitor. The median progression free survival was 6.4 months, which delayed time to next line of therapy and was associated with an acceptable safety profile.
Regarding toxicity management, Dr. Mukherji highlighted bone health and avoiding treatment related fractures. There are many potential threats to bone health, including ADT, steroids, androgen receptor pathway inhibitors, age, and chemotherapy. These mCRPC patients should be considered for zoledronic acid or denosumab, a dental review prior to initiating therapy, and provided with calcium and vitamin D supplementation.
Patients are also at risk of cardiovascular toxicity with androgen receptor pathway inhibitor therapy in mCRPC. In a systematic review and meta-analysis of cardiovascular events and androgen receptor pathway inhibitors in prostate cancer, El-Taji and colleagues9 found that androgen receptor pathway inhibitors significantly increased the risk of hypertension and cardiac dysrhythmias:

Cardio-oncology aspects and goals for our patients are the following:
- High intensity statin when indicated
- Blood pressure <130/80 mmHg (ACE inhibitor/ARB)
- Optimizing glycemic control (HbA1c <7%)
- Addressing atrial fibrillation and coronary artery disease early
- Regular EKG + QTc monitoring while on androgen receptor pathway inhibitors
- Lifestyle modifications: exercise, smoking cessation
- Cardio-oncology referral for 1+ major cardiovascular risk
Borrowing work from Dr. Chris Sweeney, Dr. Mukherji emphasize the optimized use of endocrine therapies and chemotherapies in mCRPC, by sequencing of active, survival-prolonging therapy, and taking into account patient preferences, co-morbidities, and therapy access:
- Oligo-progression (bone): consider external beam radiotherapy
- Germline BRCA or somatic BRCA, CHEK2, PALB2 mutations: PARP inhibitor +/- androgen receptor pathway inhibitor
- PSMA PET positive disease with no discordance: Lu-PSMA
- “Anaplastic” PTEN loss, p53 mutant, RB1 mutant: carboplatin + taxane
- None of the above: Docetaxel (or cabazitaxel if prior docetaxel), or radium-223 for bone-only disease
Dr. Mukherji concluded her presentation discussing optimized use of endocrine therapies and chemotherapies in mCRPC with the following take home points:
- Translating evidence from clinical trials into practice has been a challenge – as a community we need to advocate for our patients to receive all the evidence-based therapies available to them
- Treatment-selection biomarkers are becoming increasingly important to inform our sequencing choices – we also need to be aware of the limitations
- Pro-active management of cardio-metabolic risks and bone health is essential for all patients with advanced prostate cancer
Presented by: Deborah Mukherji, MBBS, FRCP, Clemenceau Medical Center Dubai, Dubai, United Arab Emirates
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Rivas JG, Kraft P, Evans-Axelsson S, et al. Real-world evidence on baseline characteristics and treatment in metastatic hormone-sensitive prostate cancer: Findings from the PIONEER 2.0 Big Data Investigation Group. 2025 Nov;81:82-91.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Tombal B, Choudhury A, Saad F, et al. Enzalutamide plus radium-223 in metastatic castration-resistant prostate cancer: results of the EORTC 1333/PEACE-3 trial. Ann Oncol. 2025 Sep;36(9):1058-1067.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with metastatic-castration-resistant prostate cancer: final overall survival results from the randomized, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet. 2025 Aug 2;406(10502):447-460.
- Narayan V, Patel MY, Teitsson S, et al. Treatment patterns and survival outcomes among androgen receptor pathway inhibitor-experienced patients with metastatic castration-resistant prostate cancer. Clin Genitourin Cancer. 2024 Dec;22(6):102188.
- Fancolini G, Allegra AG, Detti B, et al. Stereotactic body radiation therapy and abiraterone acetate for patients affected by oligometastatic castrate-resistant prostate cancer: A randomized phase II trial (ARTO). J Clin Oncol. 2023 Sep 21;JCO2300985.
- Niazi T, Saad F, Tisseverasinghe S, et al. Metastasis-directed therapy in addition to standard systemic therapy in oligometastatic castration-resistant prostate cancer in Canada (GROUQ-PCS 9): A multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2025 Sep;26(9):1158-1167.
- Patel P, Dreibe S, Attard G, et al. Stereotactic body radiation therapy for oligoprogressive disease in androgen-suppressed prostate cancer: Primary endpoint analysis of the TRAP trial. Int J Radiat Oncol Biol Phys. 2025 Mar 9 [Epub ahead of print].
- El-Taji O, Taktak S, Jones C, et al. Cardiovascular events and androgen receptor signaling inhibitors in advanced prostate cancer: A systematic review and meta-analysis. JAMA Oncol. 2024 Jul 1;10(7):874-884.