(UroToday.com) The 2025 ESMO annual meeting featured a metastatic castration-resistant prostate cancer (mCRPC) session and a presentation by Dr. Irene Burger discussing optimized use of radioligand therapy in mCRPC. Dr. Burger started her presentation by emphasizing that there are many ways to improve outcomes in mCRPC with radioligand therapy (both 177Lu-PSMA-617 and radium-223), but the ultimate aim is to improve outcomes and quality of life. For her presentation, Dr. Burger focused on five ways to optimize use of radioligand therapy.
First, improving patient selection for radioligand therapy based on PSMA PET/CT. The phase 3 VISION trial evaluated 177Lu-PSMA-617 in men with PSMA-positive mCRPC who had previously received treatment with a next-generation androgen receptor signaling inhibition (abiraterone, enzalutamide, etc) and one or two prior lines of taxane chemotherapy:
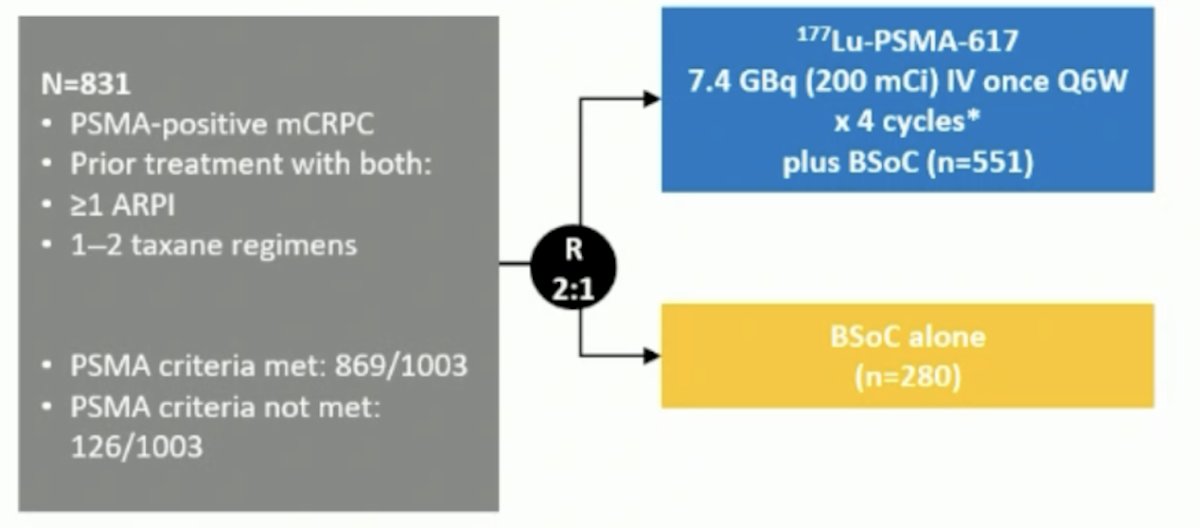
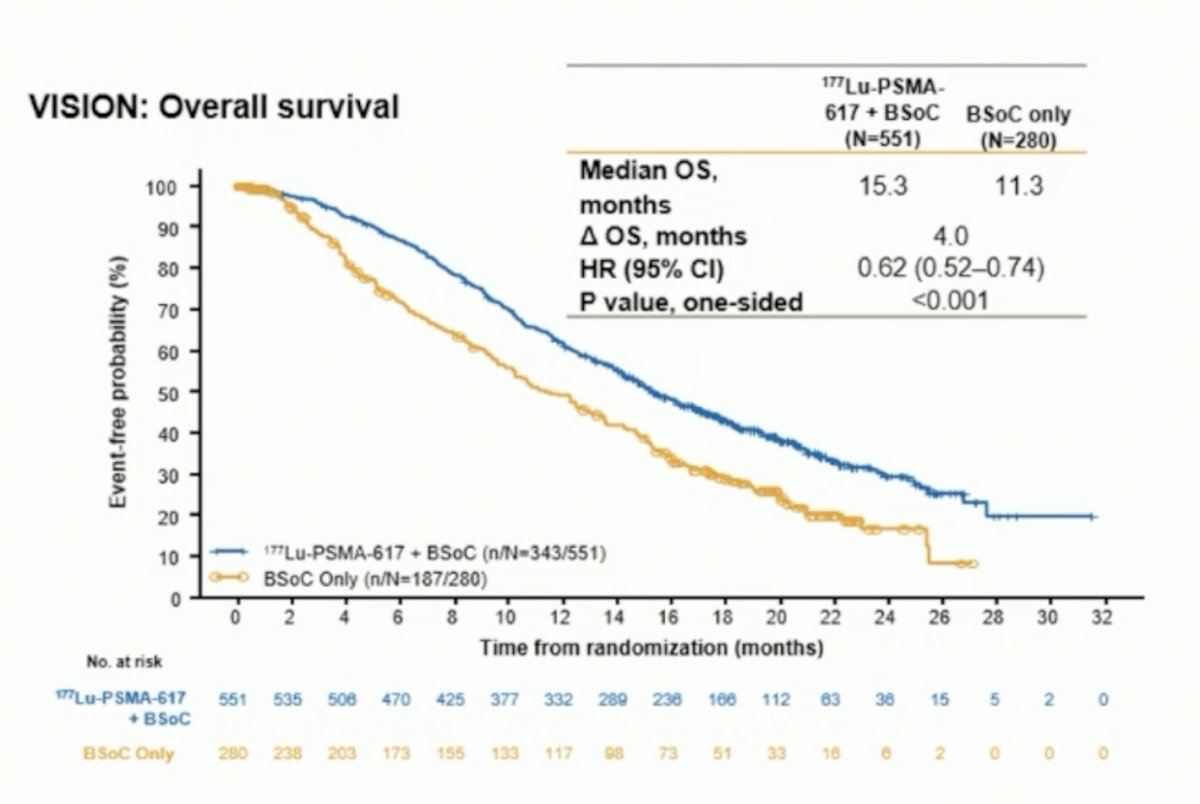
There were two alternate primary endpoints: radiographic progression free survival and overall survival. Treatment with 177Lu-PSMA-617 + standard of care significantly improved radiographic progression free survival, treatment with 177Lu-PSMA-617 + standard of care significantly improved radiographic progression free survival by a median 5.3 months (median radiographic progression free survival, 8.7 versus 3.4 months; HR 0.40, 99.2% CI 0.29 to 0.57; p < 0.001, one-sided). For overall survival 177Lu-PSMA-617 improved overall survival by a median of 4.0 months (median overall survival: 15.3 versus 11.3 months; HR 0.62, 95% CI 0.52 to 0.74; p < 0.001, one-sided), compared to standard of care alone:
To explore the association between quantitative baseline 68Ga-PSMA-11 PET/CT parameters and treatment response and outcomes in the VISION trial, Kuo et al. found that whole-body tumor SUVmean was the best predictor of 177Lu-PSMA-617 efficacy, with a HR range of 0.86-1.43 for all outcomes (all p < .001).2 A 1-unit whole-body tumor SUVmean increase was associated with a 12% and 10% decrease in risk of a radiographic progression free survival event and death, respectively. Presented at ESMO 2025 by Herrmann et al., patients in the 177Lu-PSMA-617 arm of PSMAfore with an SUVmean ≥ median had longer radiographic progression free survival than those with SUVmean < median:
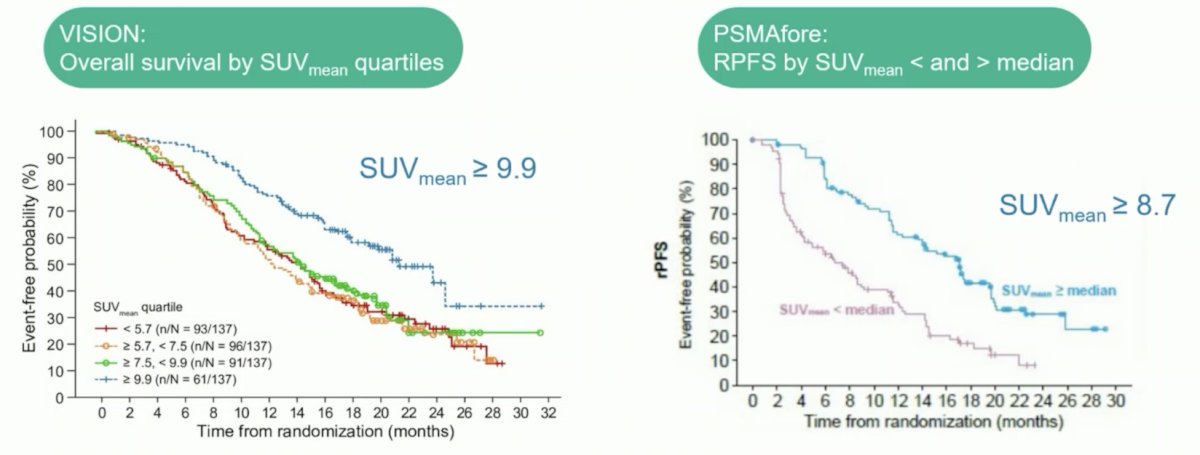
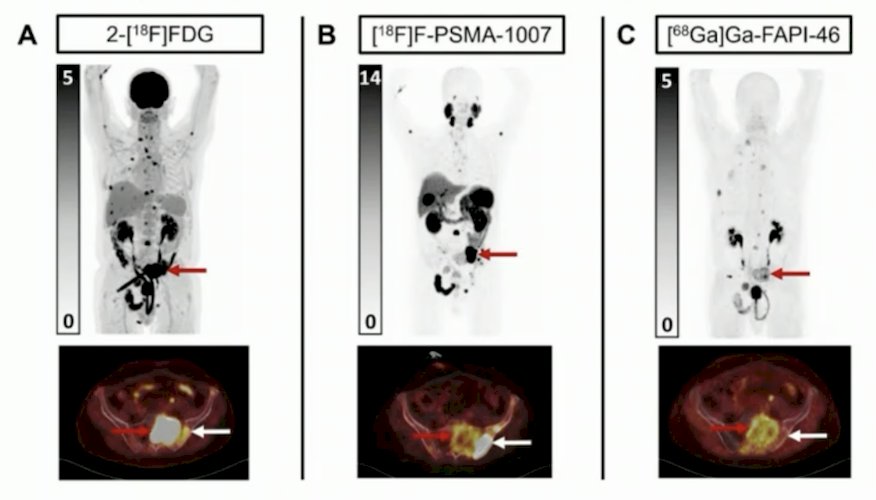
Thus, Dr. Berger emphasized that patients with SUVmean > 9-10 have more benefit from 177Lu-PSMA-617 radioligand therapy. Additionally, patients with PSMA PET and PDG PET mismatch lesions also have improved benefit from 177Lu-PSMA-617 radioligand therapy:
Second, scheduling and the number of radioligand therapy cycles given. In PSMAfore,3 7.4 GBq of 177Lu-PSMA-617 every 6 weeks was given for up to 6 cycles (up 44.4 total GBq), with a median radiographic progression free survival of 12.0 months. On the contrary, in SPLASH (presented at ESMO 2024), 6.8 GBq of 177Lu-PNT2000 every 8 weeks was given for up to 4 cycles (up to 27.2 total GBq), with a median radiographic progression free survival of 9.5 months:
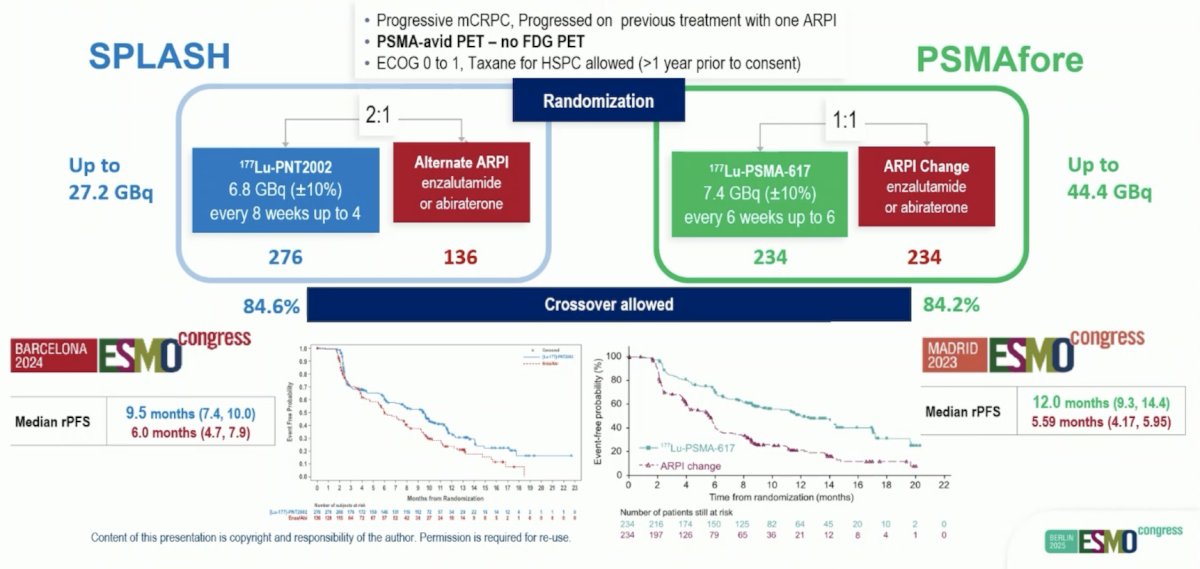
Currently, Dr. Berger endorses 6 x 7.4 GBq every 6 weeks rather than 4 x 6.8 GBq every 8 weeks based on the more impressive radiographic progression free survival in PSMAfore.
Third, therapy monitoring for PSMA radioligand therapy. Prostate cancer changes over the course of the disease process and treatments received. After progression on ADT, there is a decrease in androgen receptor expression and increase in PSMA expression, and after radioligand therapy, partial responders have a decrease in PSA and PSMA tumor volume. However, in progressive disease after radioligand therapy, there may be (i) increased PSA and increased PSMA tumor volume, or (ii) decreased PSA and decreased tumor volume. Thus, it is important to consider not just PSMA PET/CT in follow-up, but also 18F-FDG PET in situations where there may be PSA and clinical discordance, as highlighted in the following patient example:

PSMA PET/SPECT is good for monitoring, as long as it is in line with the clinical picture and laboratory results. Dr. Berger cautions that we must be aware of potential negative selection of PSMA negative tumors after radioligand therapy, and consider alternative imaging if progression is suspected (FDG PET, DWI MRI, etc).
Fourth, assessing the ideal time point for PSMA radioligand therapy. In addition to VISION, SPLASH, and PSMAfore in the mCRPC space, we have seen at ESMO 2025 presentations on LUNAR for 177Lu-PSMA in the oligometastatic mHSPC setting, as well as PSMAddition for 177Lu-PSMA in mHSPC, and previously LuTectomy4 with 177Lu-PSMA for patients with high risk localized disease. In the mCRPC setting, is the ideal time point before or after a taxane? In addition to the previously published PSMAfore trial in the pre-chemotherapy mCRPC space, data from the Canadian Cancer Trials Group (CCTG) PR21 trial (presented at ESMO 2025) randomized mCRPC patients to docetaxel versus 177Lu-PSMA-617. Patients receiving 177Lu-PSMA-617 had a median radiographic progression free survival of 8.6 months versus 10.7 months for docetaxel (HR 1.01, 90% CI 0.77-1.31):
With regards to overall survival, the median was 14.3 months for 177Lu-PSMA-617 to docetaxel versus 18.2 months for docetaxel to 177Lu-PSMA-617 (HR 1.64, 95% CI 1.14, 2.35), suggesting a benefit for earlier use of docetaxel and later use of 177Lu-PSMA-617:

In LUNAR, also presented at ESMO 2025, patients with 1–5 PSMA PET–positive lesions were randomized 1:1 to receive either stereotactic body radiotherapy alone or two cycles of 177Lu-PNT2002 (6.8 GBq every 8 weeks) followed by stereotactic body radiotherapy. After a median follow-up of 22 months (IQR 19–26), the LUNAR trial met its primary endpoint of progression free survival. The addition of radioligand therapy significantly prolonged median stereotactic body radiotherapy to 17.6 months (95% CI 15 to not reached) compared to 7.4 months (95% CI 6.0–13.5) with stereotactic body radiotherapy alone (HR 0.37, 95% CI 0.22–0.61, p<0.0001):

In PSMAddition (also presented at ESMO 2025), men with untreated or minimally treated mHSPC and ≥1 PSMA-positive metastatic lesion on 68Ga-PSMA-11 PET/CT were randomized to:
- Experimental arm: 177Lu-PSMA 617 (7.4 GBq ±10% 6 cycles every 6 weeks) + ADT + androgen receptor pathway inhibitor
- Control arm: ADT + androgen receptor pathway inhibitor
- Crossover to the 177Lu-PSMA 617 arm was permitted upon radiographic progression
The study met its primary endpoint with radiographic progression free survival significantly prolonged with the addition of 177Lu-PSMA-617 (HR 0.72, 95% CI 0.58-0.90, p = 0.002). Median radiographic progression free survival has not been reached in either arm yet:

However, the adverse event profile was not insignificant for a cumulative dose of 44.4 GBq of 177Lu-PSMA-617 in the mHSPC setting:
- Dry mouth: 46% versus 4%
- Nausea: 34% versus 9%
- Constipation: 18% versus 16%
- Decreased appetite: 14% versus 6.5%
- Vomiting: 14% versus 4%
Fifth, assessing safety and efficacy of different radionuclides such as 225Actinium and 161Terbium. 225Ac-PSMA-617 radioligand therapy has shown preliminary evidence of clinical efficacy in patients with mCRPC5 and may represent a viable treatment option in patients who have received previous lines of therapy:

225Ac-PSMA-617 was assessed in the retrospective multicenter study WARMTH Act, specifically 488 patients at 7 centers. 225Ac-PSMA-617was associated with a median overall survival of 15.5 months and median progression free survival of 7.9 months. Any PSA decline was noted in 73% of patients and PSA50 response was noted in 57% of patients.
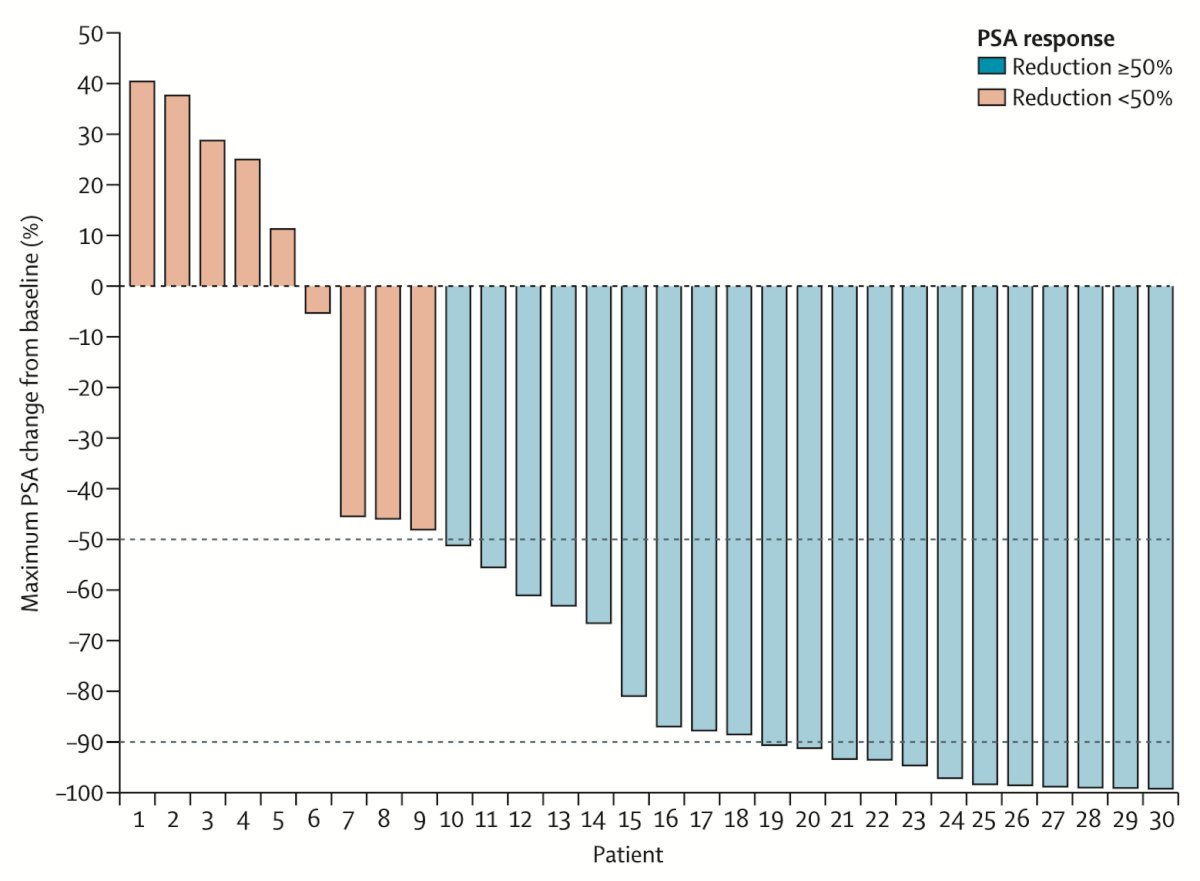
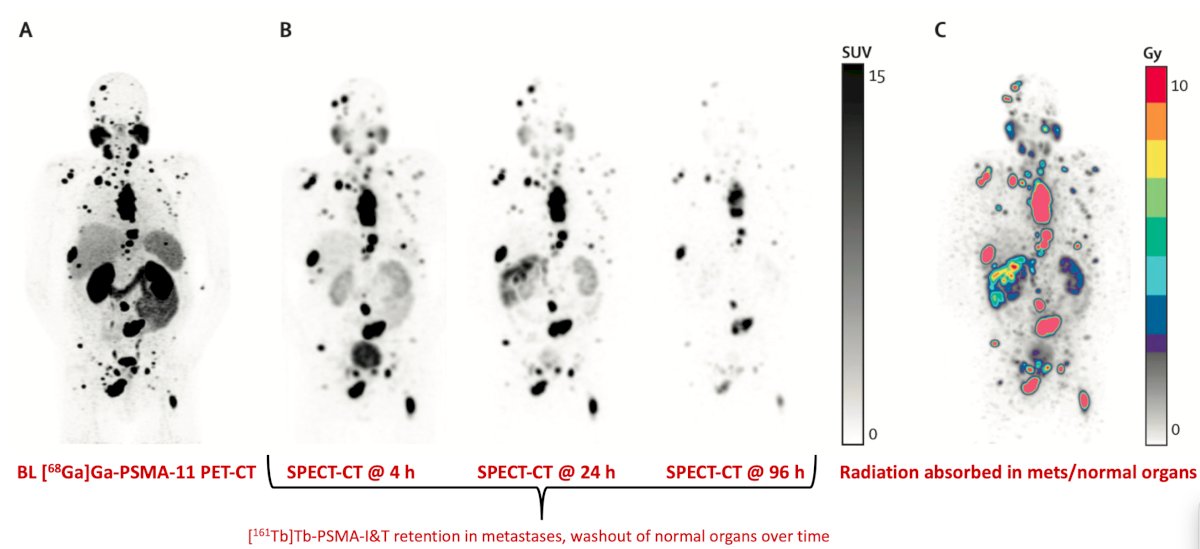
161Tb-PSMA-I&T was assessed in the VIOLET single center, single arm phase 1/2 study.6 Among 30 eligible patients, 20 (67%) of 30 patients had received previous docetaxel. There were no dose-limiting toxicities and the maximum administered dose and recommended phase 2 dose was 7.4 GBq. Grade 3 treatment related adverse events were limited to pain (1, 3%; the only serious treatment related adverse events) and lymphopenia (1, 3%). No grade 4 treatment related adverse events or treatment-related deaths occurred. The PSA50 response rate for 161Tb-PSMA-I&T was 70% (95% CI 51-85) and the PSA90 response rate was 40% (95% CI 23-59):
An example of 3-time point quantitative SPECT @ cycle 1 is highlighted in the following figure:
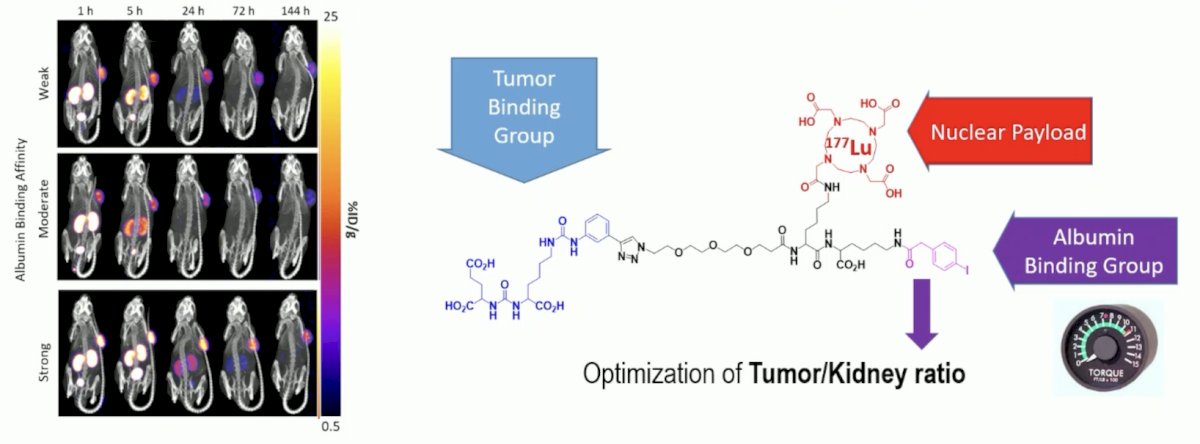
Dr. Burger also noted that improved biodistribution is necessary, specifically tuning the strength of the albumin binding group altering tumor uptake and the therapeutic index:
Dr. Burger concluded this presentation discussing optimized use of radioligand therapy in mCRPC with the following take home points:
- Patient selection based on PSMA PET:
- Patients with SUVmean > 9–10 benefit more from radioligand therapy
- Patients without mismatch lesions also derive greater benefit
- Numbers of cycles and scheduling:
- 6×7.4 GBq every 6 weeks is > 4×6.8 GBq every 8 weeks
- More than 6 cycles seems safe and effective
- Shorter intervals for aggressive disease might be better
- Therapy monitoring:
- Cave: for PSMA negative tumors after radioligand therapy
- Consider ceCT / FDG / DWI if progression is suspected
- Ideal time point of radioligand therapy:
- Still an open question and depends on the radionuclide
- Different radionuclides / improved biodistribution:
- 161Tb and 225Ac – have the potential to bring more efficacy, however the side-effect profile needs consideration
- Tailoring albumin binding might improve the side effect profile and efficacy
- Combinations with radioligand therapy
- Different targets
Presented by: Irene A. Burger, UniversitatsSpital Zurich, Zurich, Switzerland
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Kuo PH, Morris MJ, Hesterman J, et al. Quantitative 68Ga-PSMA-11 PET and Clinical Outcomes in Metastatic Castration-resistant prostate cancer following 177Lu-PSMA-617 (VISION Trial). Radiology. 2024 Aug;312(2):e233460.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Eapen RS, Buteau JP, Jackson P, et al. Administering [177Lu]Lu-PSMA-617 Prior to Radical Prostatectomy in Men with High-risk Localized Prostate Cancer (LuTectomy): A Single-centre, single-arm, phase 1/2 study. Eur Urol. 2023 Oct 25:S0302-2838(23)03087-7.
- Sathekge MM, Lawal IO, Bal C, et al. Actinium-225-PSMA radioligand therapy of metastatic castration-resistant prostate cancer (WARMTH Act): A multicentre, retrospective study. Lancet Oncol. 2024 Feb;25(2):175-183.
- Buteau JP, Kostos L, Jackson PA, et al. First-in-human results of terbium-161 [161Tb]Tb-PSMA-I&T dual beta-Auger radioligand therapy in patients with metastatic castration-resistant prostate cancer (VIOLET): A single-centre, single-arm, phase 1/2 study. Lancet Oncol. 2025 Aug;26(8):1009-1017.