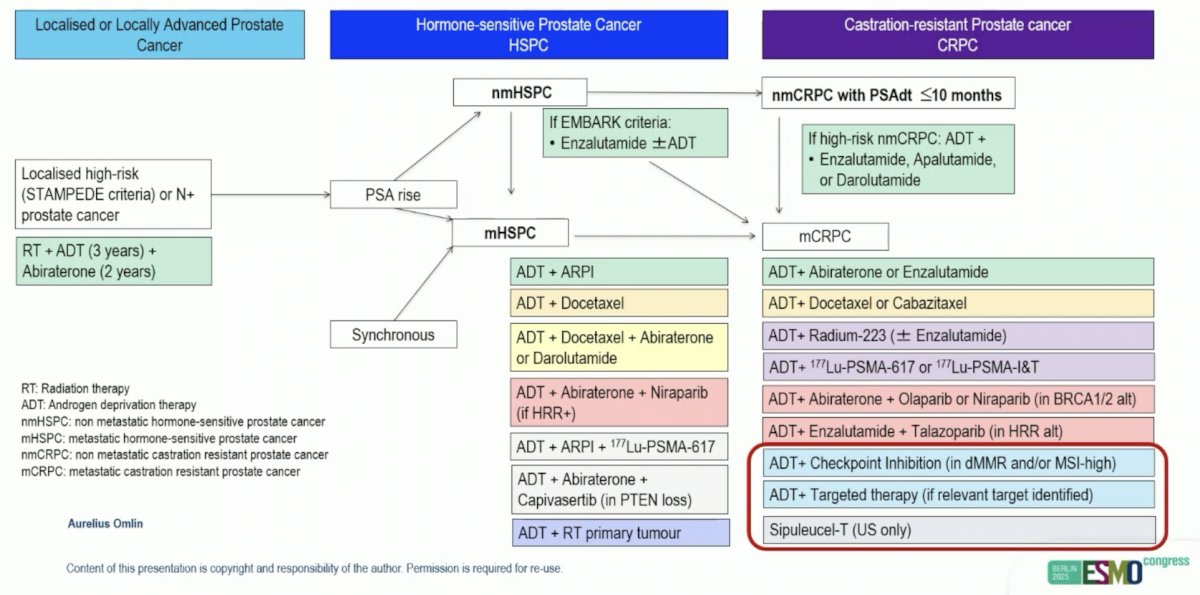
(UroToday.com) The 2025 ESMO annual meeting featured a metastatic castration-resistant prostate cancer (mCRPC) session and a presentation by Dr. Aurelius Omlin discussing optimized use of immunotherapy and targeted therapies in mCRPC. Dr. Omlin notes that the treatment landscape for advanced prostate cancer is vast, however his talk will specifically focus on ADT + checkpoint inhibition, ADT + targeted therapy, and sipuleucel-T:
Immunotherapy has been around in prostate cancer since 2010, when results of the phase III IMPACT trial were published.1 Sipuleucel-T is an autologous vaccine processed following peripheral dendritic cell collection via leukapheresis. This is then incubated with GCS-F and PAP protein, followed by reinfusion into the patient (after a 36-44 hour period) in order to generate a PAP-specific CD4+ and CD8+ T cell response. IMPACT enrolled 512 patients with mCRPC who had asymptomatic disease/minimally symptomatic with no visceral metastases, randomizing men to three infusions of sipuleucel-T (n = 341) or placebo (n = 171). The IMPACT trial noted a 4.1-month improvement in overall survival for those receiving sipuleucel-T compared to placebo, and a 22% reduction in risk of death (HR 0.78, 95% CI 0.61-0.98):
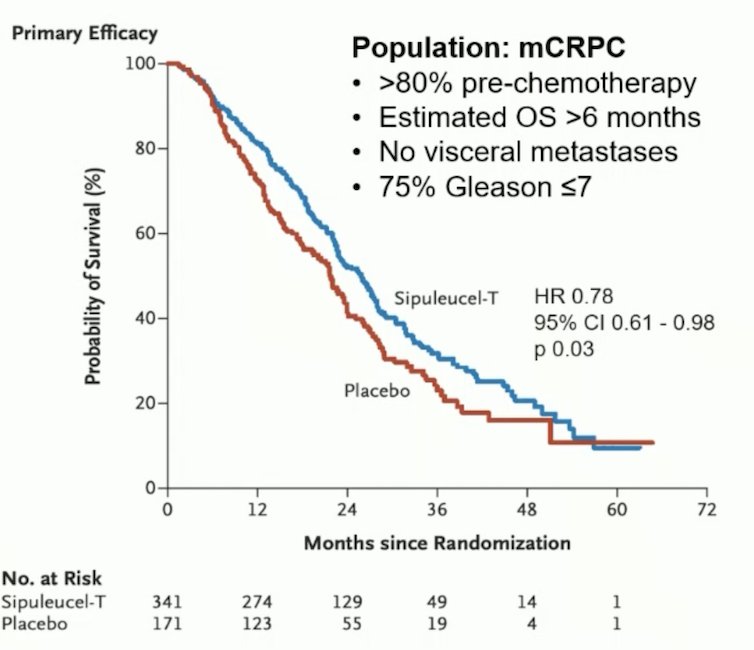
There was no difference between the groups with regards to objective disease progression or PSA response (secondary endpoints). An assessment of safety profile for patients in this study found that the treatment was overall well tolerated with minimal concern for severe adverse events. Dr. Omlin notes that sipuleucel-T was only approved by the FDA (not the EMA) in 2010 for the treatment of asymptomatic or minimally symptomatic mCRPC, with long-term responders having been reported. However, no robust biomarkers for response to sipuleucel-T have been identified.
With regards to ipilimumab in mCRPC, this immunotherapy was tested in the phase III CA184-043 trial for patients who had progressed on docetaxel chemotherapy, randomizing 799 patients to ipilimumab or placebo after bone-directed radiotherapy.2 The primary endpoint was overall survival, with no difference between the groups (ipilimumab 11.2 months versus placebo 10 months; HR 0.85, p = 0.053); however, there was a small benefit in progression free survival favoring ipilimumab (4.0 versus 3.1 months; HR 0.70, p < 0.0001). Subsequently, Beer et al.3 reported findings of another phase III trial (CA184-095) randomizing 602 patients (2:1) with metastatic chemotherapy-naïve CRPC to ipilimumab versus placebo. Similar to the post-docetaxel patients, there was no difference in overall survival between the groups (HR 1.11, 95% CI 0.88-1.39), however men receiving ipilimumab had improved progression free survival (5.6 months versus 3.8; HR 0.67, 95% CI 0.55-0.81) compared to those receiving placebo:
![With regards to ipilimumab in mCRPC, this immunotherapy was tested in the phase III CA184-043 trial for patients who had progressed on docetaxel chemotherapy, randomizing 799 patients to ipilimumab or placebo after bone-directed radiotherapy [2]. The primary endpoint was overall survival, with no difference between the groups (ipilimumab 11.2 months versus placebo 10 months; HR 0.85, p = 0.053); however, there was a small benefit in progression free survival favoring ipilimumab (4.0 versus 3.1 months; HR 0.70, p < 0.0001). Subsequently, Beer et al. [3] reported findings of another phase III trial (CA184-095) randomizing 602 patients (2:1) with metastatic chemotherapy-naïve CRPC to ipilimumab versus placebo. Similar to the post-docetaxel patients, there was no difference in overall survival between the groups (HR 1.11, 95% CI 0.88-1.39), however men receiving ipilimumab had improved progression free survival (5.6 months versus 3.8; HR 0.67, 95% CI 0.55-0.81) compared to those receiving placebo:](/images/com-doc-importer/232-esmo-2025/esmo-2025-optimized-use-of-immunotherapy-and-targeted-therapies-in-mcrpc/image-2.jpg)
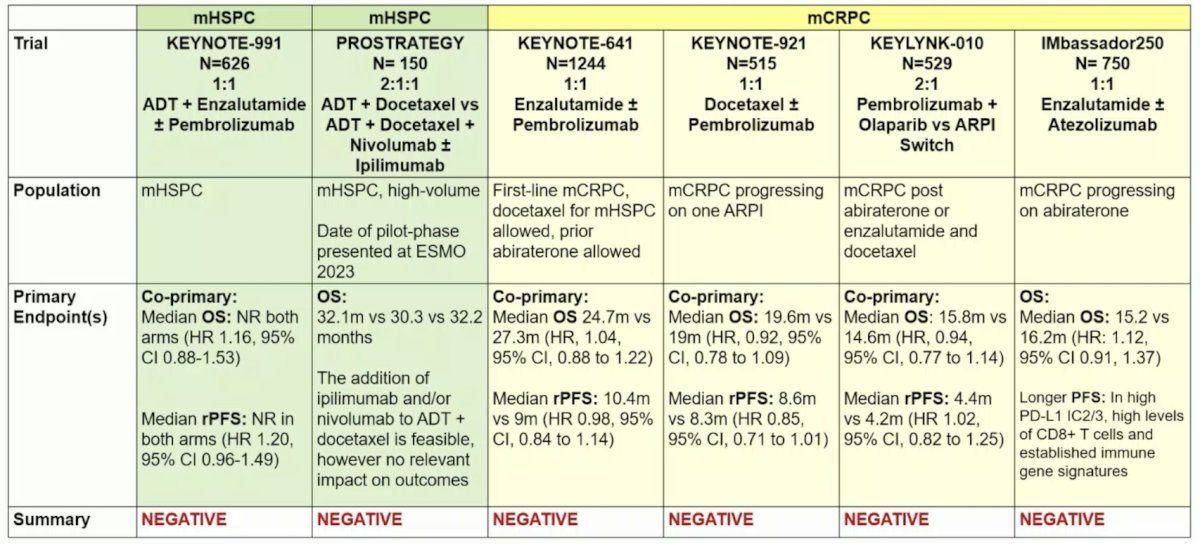
The following table highlights all 6 PD1/PD-L1 inhibitor trials in unselected patients (phase III trials), all of which are negative trials:
Because cabozantinib has been shown to induce favorable changes in the tumor microenvironment and regression of prostate tumors in vivo, it was subsequently combined with atezolizumab in the phase 3 CONTACT-02 trial. In this trial, patients were randomized 1:1 to cabozantinib + atezolizumab (cabozantinib [40 mg PO daily] + atezolizumab [1200 mg IV every 3 weeks]) or control (abiraterone [1000 mg PO daily] + prednisone [5 mg PO twice daily] or enzalutamide [160 mg PO daily]) and were stratified by liver metastasis (yes/no), prior docetaxel for mHSPC (yes/no), and prior novel hormonal therapy for mHSPC, M0CRPC, or mCRPC. The trial design for CONTACT-02 is as follows:
![Because cabozantinib has been shown to induce favorable changes in the tumor microenvironment and regression of prostate tumors in vivo, it was subsequently combined with atezolizumab in the phase 3 CONTACT-02 trial. In this trial, patients were randomized 1:1 to cabozantinib + atezolizumab (cabozantinib [40 mg PO daily] + atezolizumab [1200 mg IV every 3 weeks]) or control (abiraterone [1000 mg PO daily] + prednisone [5 mg PO twice daily] or enzalutamide [160 mg PO daily]) and were stratified by liver metastasis (yes/no), prior docetaxel for mHSPC (yes/no), and prior novel hormonal therapy for mHSPC, M0CRPC, or mCRPC. The trial design for CONTACT-02 is as follows:](/images/com-doc-importer/232-esmo-2025/esmo-2025-optimized-use-of-immunotherapy-and-targeted-therapies-in-mcrpc/image-4.jpg)
The median follow-up was 12.0 months for all randomized patients and 14.3 months for the first 400 patients. The median radiographic progression free survival was significantly longer with cabozantinib + atezolizumab versus control (6.3 versus 4.2 months; HR 0.65, 95% CI 0.50-0.84):
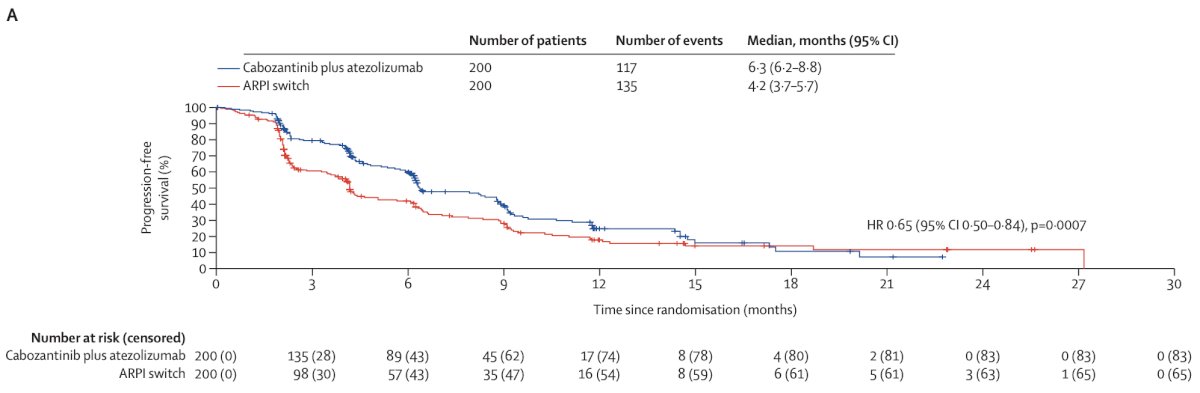
After a median follow-up of 23.1 months (IQR 17.4-30.5), overall survival was not significantly different between the cabozantinib + atezolizumab and androgen receptor pathway inhibitor switch groups (median 14.8 months versus 15.0 months; HR 0.89, 95% CI 0.72-1.10, p = 0.30):
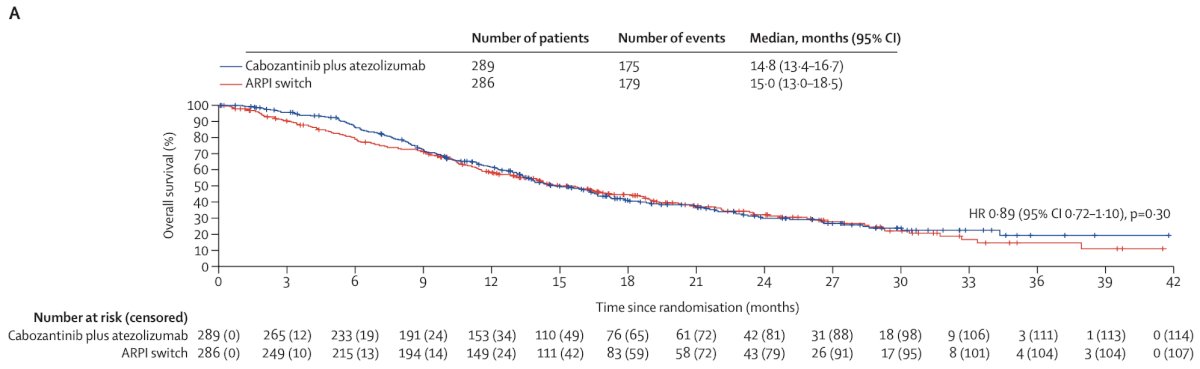
Dr. Omlin notes that the control group of androgen receptor pathway inhibitor switch in this patient population (48% visceral metastases, 23% liver metastases) was not adequate. However, there was a possible signal in patients with mCRPC and liver metastases (n = 99), noting a progression free survival of 6.2 versus 2.1 months (HR 0.43, 95% CI 0.27-0.68), and a median overall survival of 12.1 versus 7.1 months (HR 0.68, 95% CI 0.47-1.0). Of note, the trial was not powered to formally conduct hypothesis testing around biomarker-defined subgroups.
Checkpoint inhibition has also been tested in aggressive variant prostate cancer, notably the KEYNOTE-365 cohort I that assessed carboplatin + etoposide + pembrolizumab in treatment emergent or de novo neuroendocrine prostate cancer. This trial showed an objective response rate of 25%, with no complete responses, and 25% partial responses. Dr. Omlin notes that KEYNOTE-365 continues enrolment, but due to the small sample size, these results should be interpreted as preliminary.
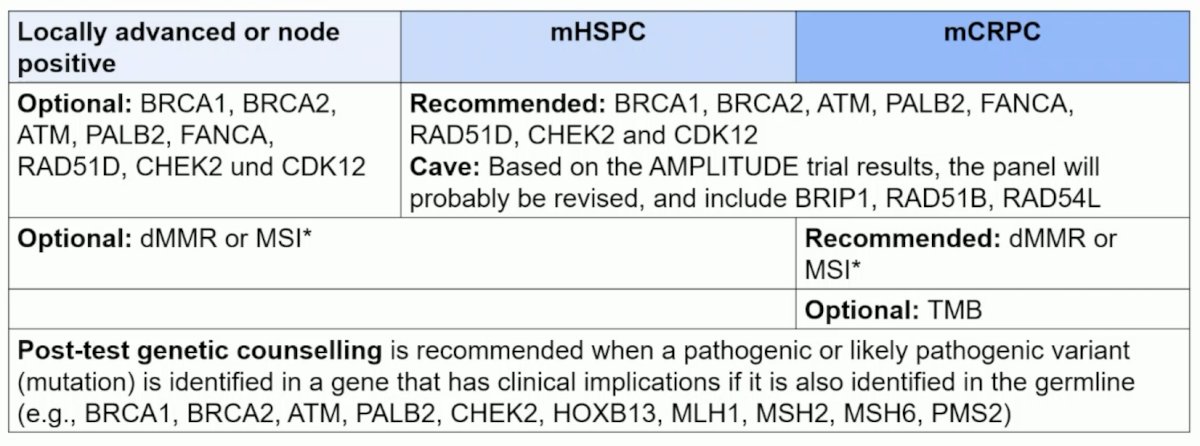
Tumor genomic profiling is the basis of targeted therapies, with the following table highlighting the options and targets in mHSPC and mCRPC:
Efficacy of PD1/PD-L1 inhibitors has been shown in selected patients with the following features:
- Loss of MMR protein expression on IHC
- Somatic or germline pathogenic or likely pathogenic alteration in one of the MMR genes
- Microsatellite instability according to polymerase chain reaction analysis or next generation sequencing (MSI-H)
- Nonsynonymous tumor mutational burden > 20 mutations/M
Dr. Omlin notes that a combination of IHC/molecular features may be the best for selecting patients at the highest likelihood of response to immune checkpoint inhibitors.
CDK12 aberrations are noted in ~5% of mCRPC patients and are associated with higher grade group, concomitant HRR alterations, ATM loss by IHC, poor prognosis, and by tumor infiltration of CD4+FOXP3- T-lymphocytes:

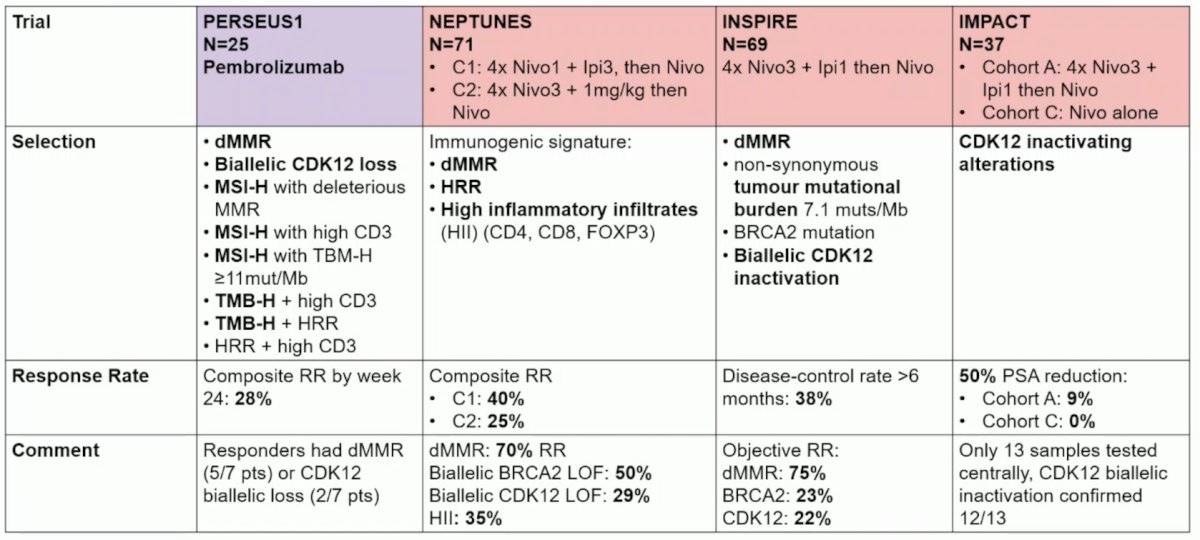
PERSEUS1, NEPTUNES, INSPIRE, and IMPACT are all prospective immunotherapy trials in selected mCRPC patients, with selection criteria and response rate noted:
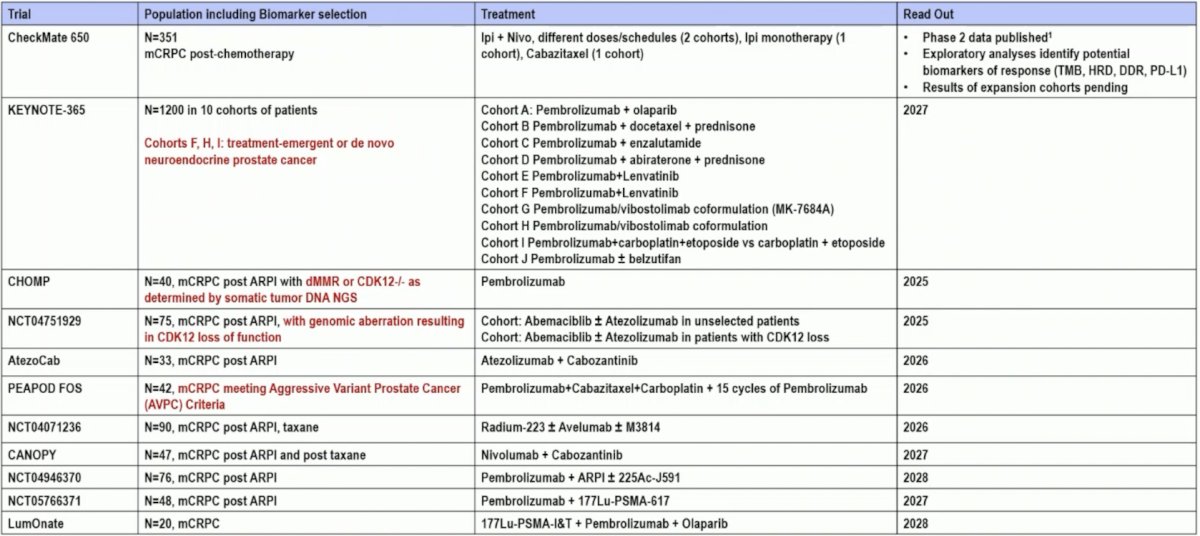
At the 2022 APCCC conference, the expert consensus panel was asked the following question: In the majority of patients with dMMR/MSH-H, do you recommend treatment with immune checkpoint inhibitor in the course of disease? 96% of respondents answered yes, and 4% answered no. At the 2024 APCCC conference, the expert consensus panel was asked the following question: In patients with mCRPC progressing on or after an androgen receptor pathway inhibitor and with an inactivating CDK12 alteration, do you recommend treatment with a checkpoint inhibitor in preference to a standard mCRPC option? 41% answered no, 25% answered yes, and 34% said yes, but only if the patient also has a high tumor mutational burden. The following table highlights pending checkpoint inhibitor trials in mCRPC:
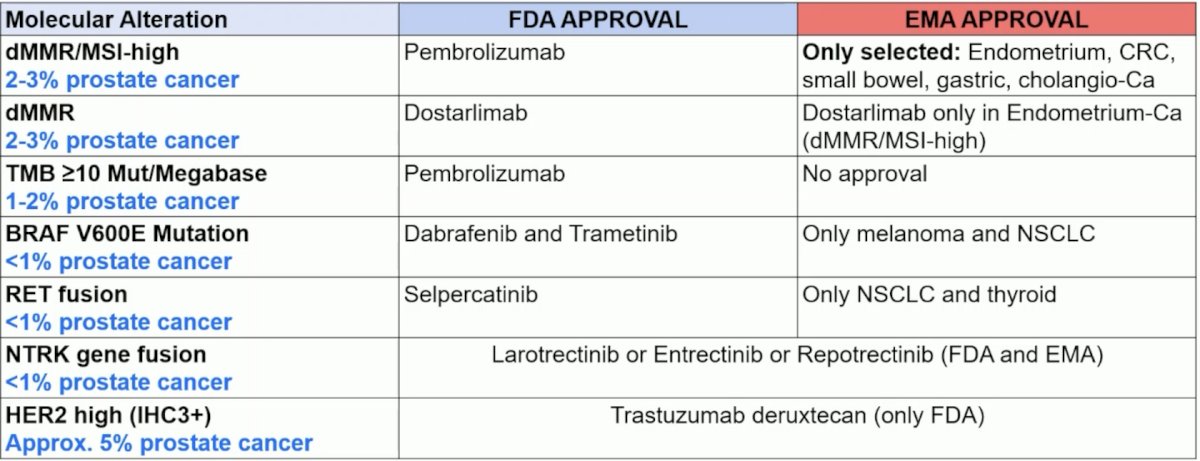
Finally, the table below highlights tumor agnostic approval of therapies in October 2025. Dr. Omlin states that generally, these targeted therapies (with the exception of checkpoint inhibitors in dMMR/MSI) should only be considered in patients progressing on/after ADT, androgen receptor pathway inhibitor, at least one taxane (if fit) and/or radioligand therapy with 177Lu-PSMA-617 (if PSMA positive disease):
Dr. Omlin concluded his presentation discussing optimized use of immunotherapy and targeted therapies in mCRPC with the following take home points for testing:
- Tumor genomic profiling (somatic testing) is recommended in patients presenting with mHSPC and the latest in mCRPC
- Treatment relevant targets:
○ BRCA1/2 alterations (approximately 10–12%)
○ Other HRR alterations (approximately 10–20%)
○ dMMR, MSI-high, (tumor mutational burden-high) (approximately 2–5%)
○ PTEN-loss by IHC ≥90% in mHSPC (depending on CAPItello approximately 25%)
○ Rare alterations and treatment based on tumor agnostic approval - If relevant changes in somatic testing are detected, we need to follow-up with post-test genetic counselling to confirm or rule out a germline alterations
Dr. Omlin also provided the following take home points with regards to treatment:
- The use of checkpoint inhibitors in unselected patients with mCRPC is not recommended
- A meaningful response with checkpoint inhibition is most likely in patients with:
dMMR (IHC or NGS) and/or MSI-high ± tumor mutational burden-high - A checkpoint inhibitor may be considered in patients with mCRPC after failure of ADT + androgen receptor pathway inhibitors
- Some patients with bi-allelic CDK12 alterations may benefit from checkpoint inhibition but no tumor agnostic approval supports the use currently
- Targeted therapies for rare alterations in individual patients should be supported by a molecular tumor board and clinical trial inclusion if possible is recommended
Presented by: Aurelius Omlin, MD, Onkozentrum Zürich, Switzerland
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med 2010;363(5):411-422.
- Kwon ED, Drake CG, Scher HI, et al. Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): a multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2014;15(7):700-712.
- Beer TM, Kwon ED, Drake CG, et al. Randomized, Double-Blind, Phase III Trial of Ipilimumab Versus Placebo in Asymptomatic or Minimally Symptomatic Patients With Metastatic Chemotherapy-Naive Castration-Resistant Prostate Cancer. J Clin Oncol. 2017;35(1):40-47.
- Agarwal N, Azad AA, Carles J, et al. Cabozantinib plus atezolizumab in metastatic prostate cancer (CONTACT-02): Final analyses from a phase 3, open-label, randomized trial. Lancet Oncol. 2025 Jul;26(7):860-876.