(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st, 2025 was host to a radioligand therapeutics proffered paper session. Dr. Kim Chi presented the Canadian Cancer Trials Group (CCTG) Study PR.21, a randomized phase II study of 177Lu-PSMA-617 versus docetaxel in mCRPC patients with PSMA-positive disease.
Dr. Chi noted that 177Lu-PSMA-617 prolongs radiographic progression-free survival (rPFS) in taxane-naïve patients with mCRPC, when compared to an androgen receptor pathway inhibitor (ARPI) switch.1 With 177Lu-PSMA-617, the median rPFS was 11.6 months, and the median overall survival (OS) was 24.5 months.1,2
Docetaxel is also a standard of care option in patients with mCRPC progressing after an ARPI. Outcomes with docetaxel after an ARPI in a recent phase III trial demonstrated a median rPFS of 8.3 months and an OS of 19 months.3
The study investigators sought to compare these two treatment options for chemotherapy-naïve mCRPC patients progressing after ARPI therapy.
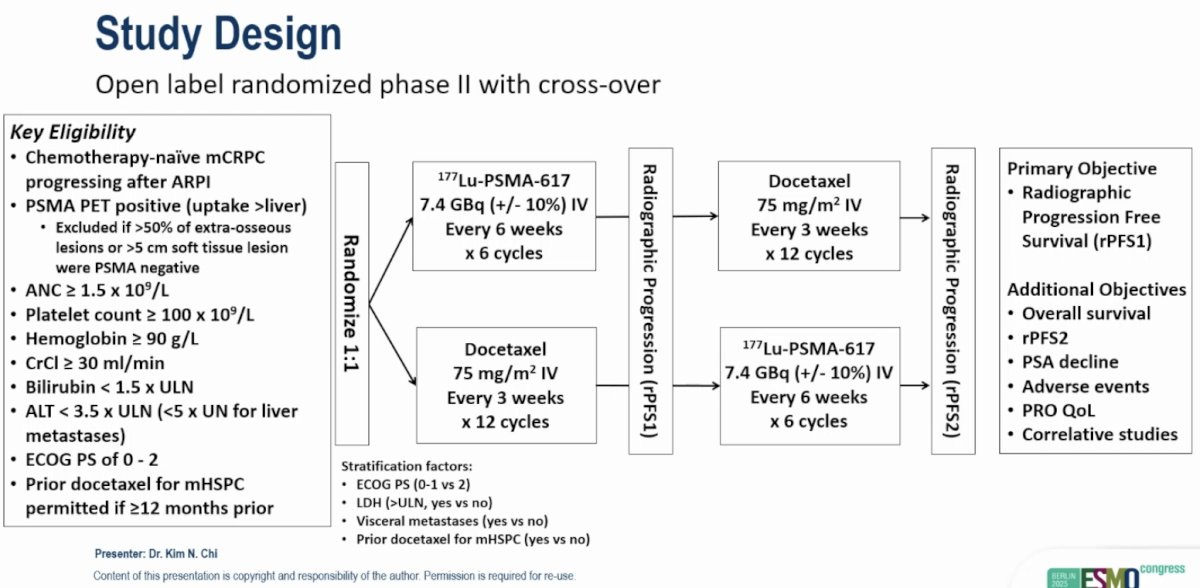
This was an open label, randomized, phase II trial that allowed for crossover between the two study arms. The key eligibility criteria were as follows:
- Chemotherapy-naïve mCRPC progressing after an ARPI
- PSMA PET positive disease (i.e., uptake >liver)
- Excluded if >50% of extra-osseous lesions or >5 cm soft tissue lesion were PSMA negative
- Adequate end organ function
- Prior docetaxel for mHSPC permitted if ≥12 months prior
Eligible patients were randomized 1:1 to:
- 177Lu-PSMA-617 7.4 GBq IV every 6 weeks x 6 cycles
- Docetaxel 75 mg/m2 every 3 weeks x 12 cycles
The primary endpoint was rPFS, with key secondary endpoints including:
- OS
- rPFS2
- PSA decline
- Adverse events
- Patient-reported outcomes/quality-of-life
- Correlative studies
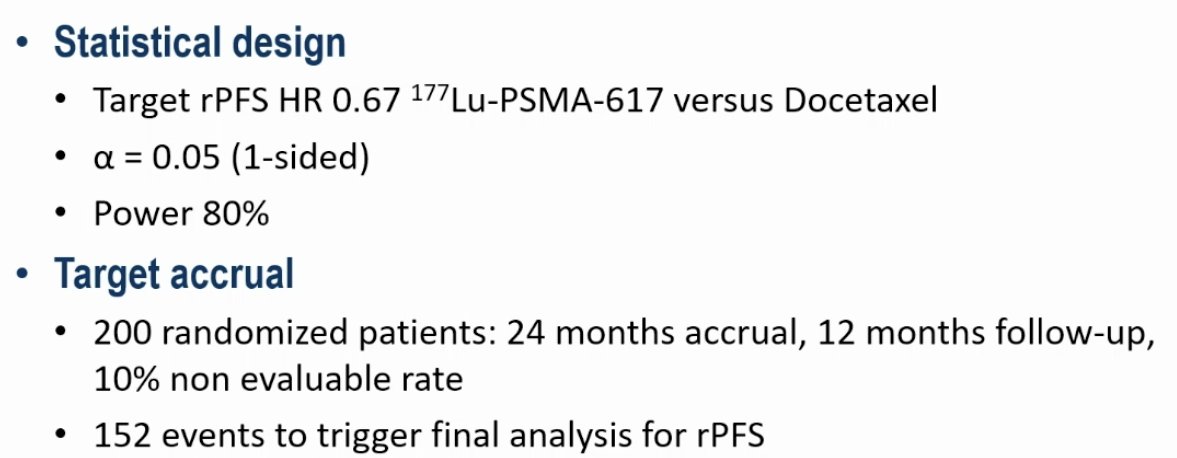
The statistical design and target sample size/accrual were as follows:
The CONSORT diagram is illustrated below. 199 patients were randomized to 177Lu-PSMA-617 (n=100) or docetaxel (n=99). The median numbers of 177Lu-PSMA-617 and docetaxel doses were 5 and 8, respectively. Fifteen patients discontinued docetaxel due to treatment-related adverse events (TRAEs), compared to only one in the 177Lu-PSMA-617 arm. Thirty-eight patients crossed over from 177Lu-PSMA-617 to docetaxel versus 56 from docetaxel to 177Lu-PSMA-617.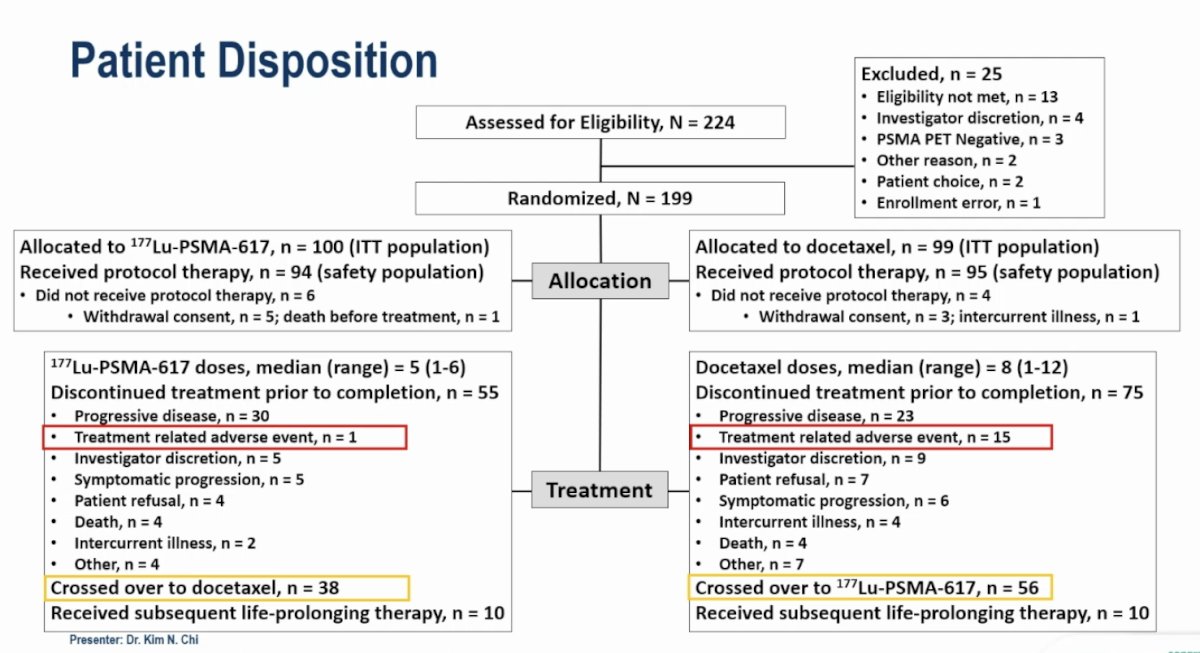
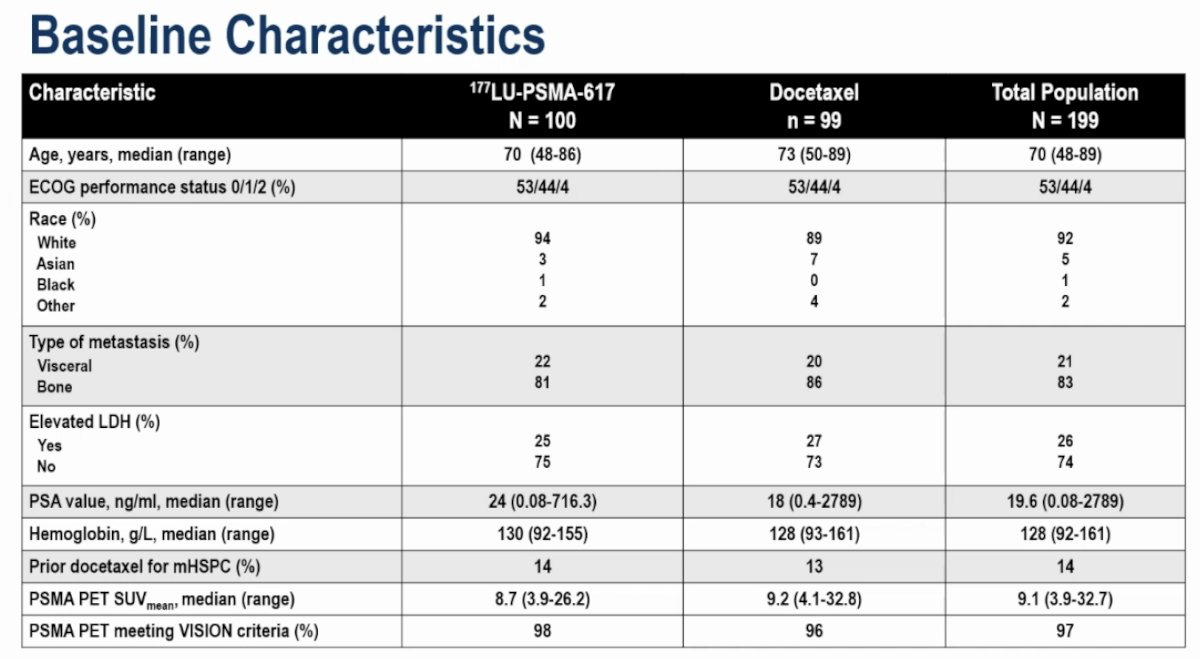
The baseline characteristics were well-balanced between the treatment arms. 96% of patients had ECOG performance status 0–1. 21% of patients had visceral metastases. The median PSA value was 19.6 ng/ml. 14% of patients had received prior docetaxel for mHSPC. The median PSMA PET SUVmean value was 9.1. 97% of patients had PSMA PET findings that met the more stringent VISION criteria.4
There was no difference in rPFS between the two arms. The median rPFS values were 8.6 and 10.7 months for the 177Lu-PSMA-617 and docetaxel arms, respectively (HR: 1.01, 95% CI: 0.77–1.31, p=0.51).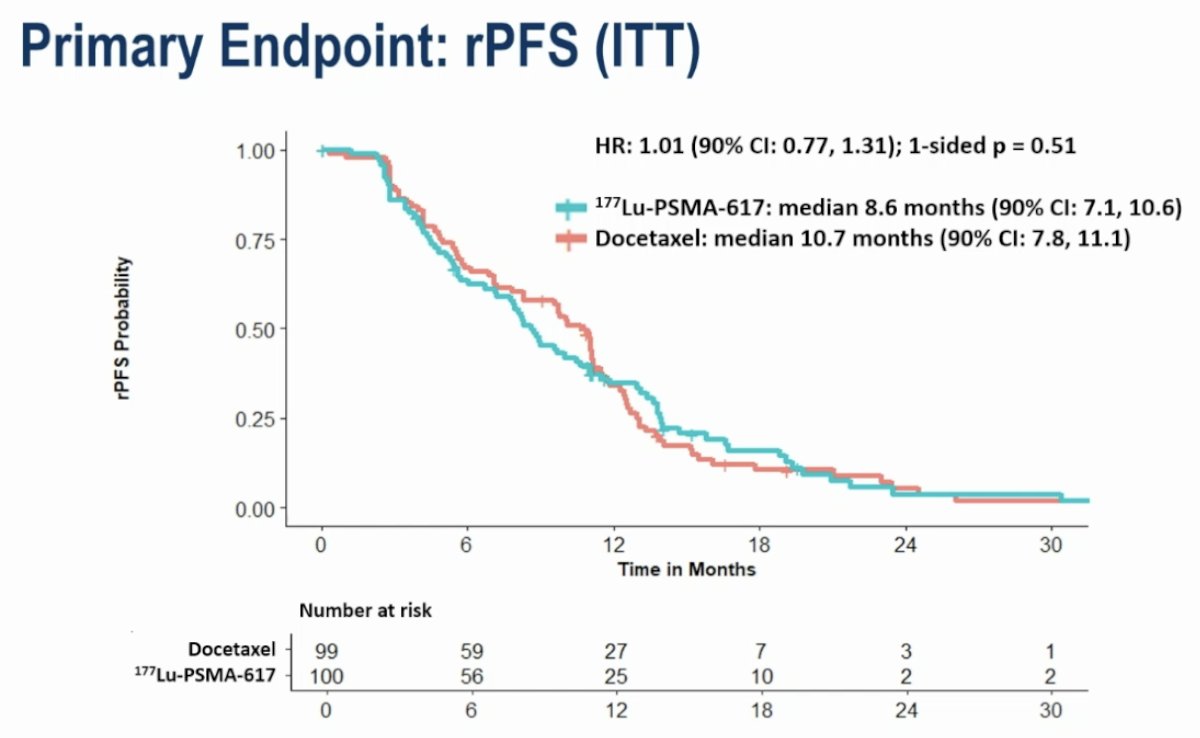
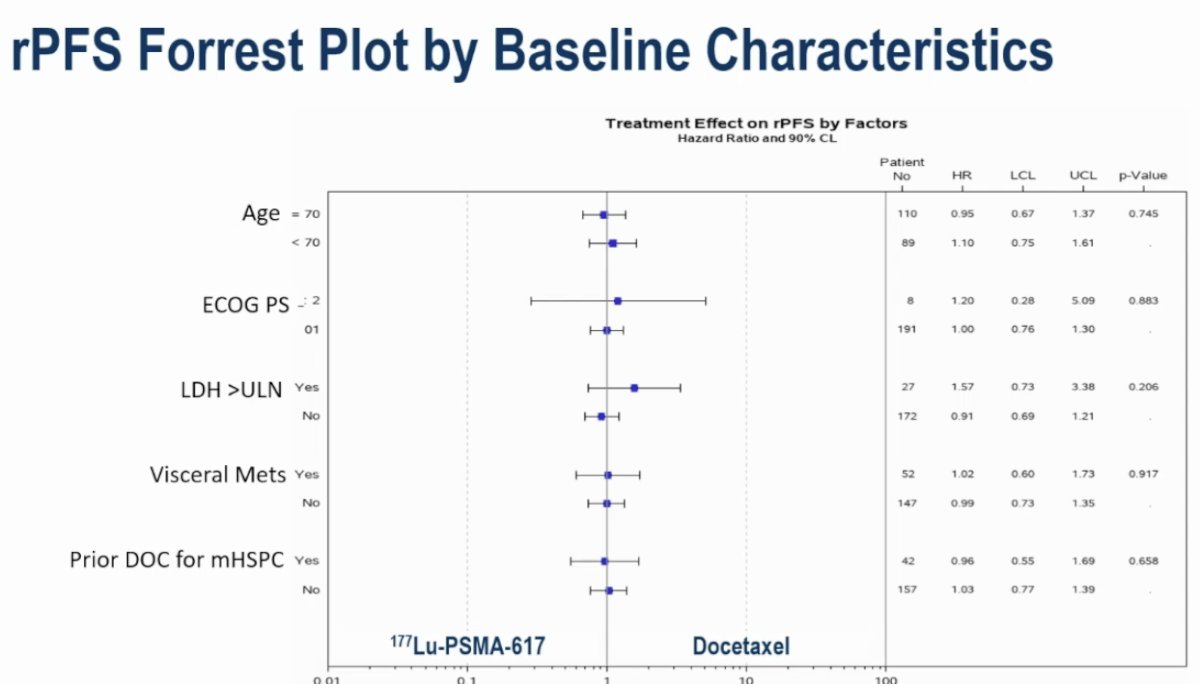
Subgroup analyses did not demonstrate a differential benefit in favor of either arm:
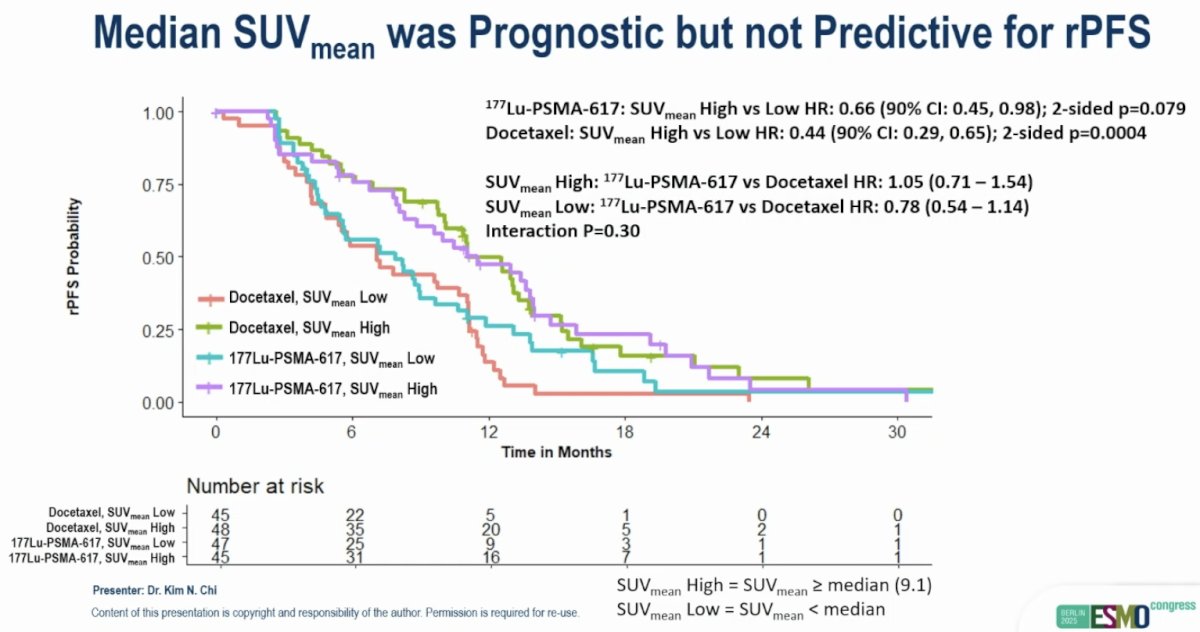
The median SUVmean was prognostic, but not predictive for rPFS. As seen below, patients with SUVmean high disease had worse rPFS outcomes, compared to SUVmean low disease, in both treatment arms. Furthermore, patients with SUVmean high disease did not derive a preferential benefit from 177Lu-PSMA-617 therapy, confirming that SUVmean was not predictive in this setting.
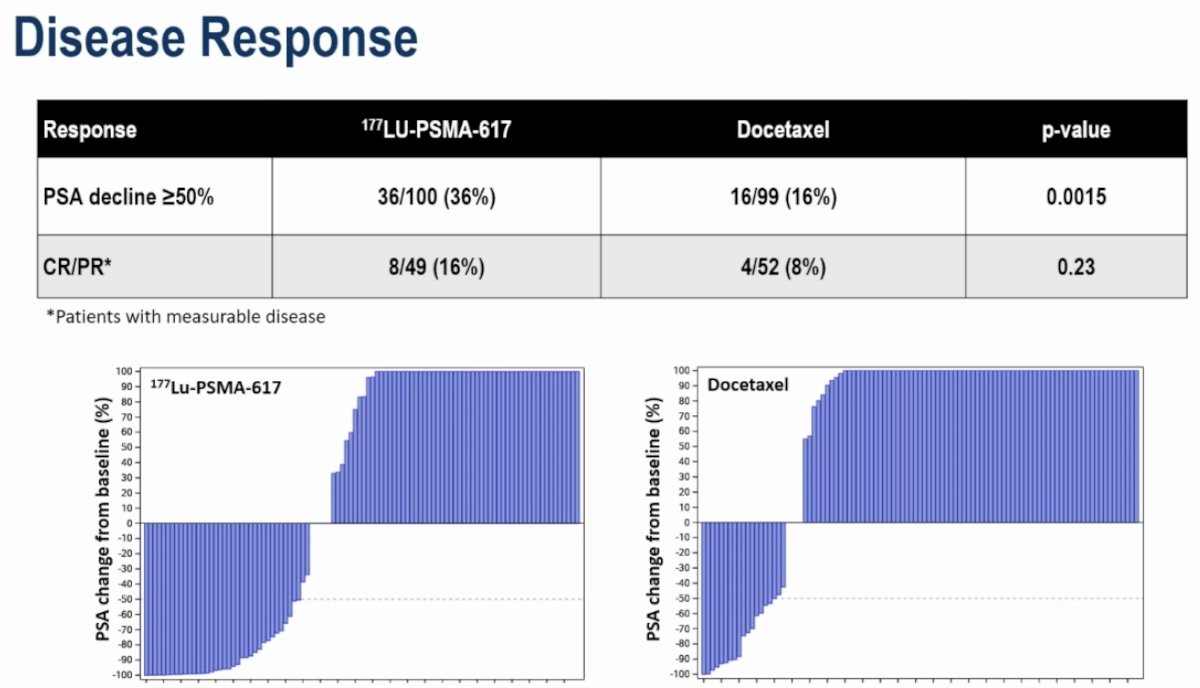
Disease response rates favored 177Lu-PSMA-617:
- PSA50 response: 36% vs 16% (p=0.0015)
- Complete or partial response: 16% vs 8% (p=0.23)
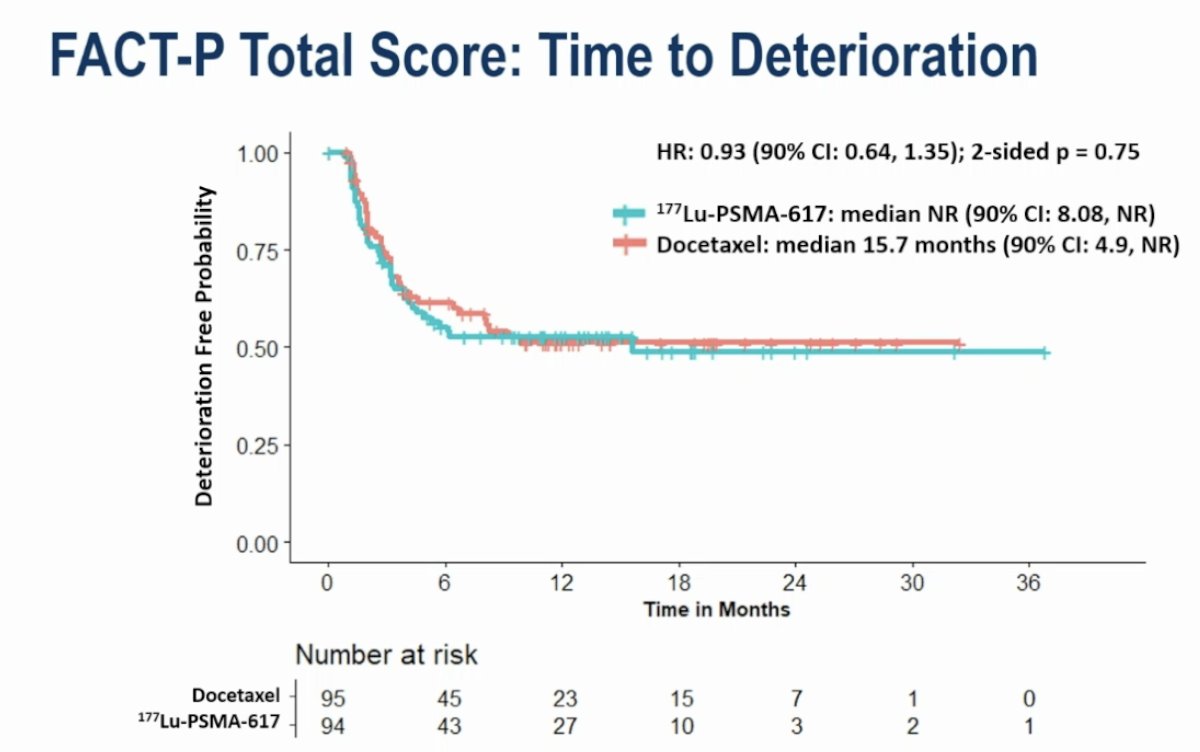
There were no differences in time to deterioration in FACT-P total score (HR: 0.93, p=0.75):
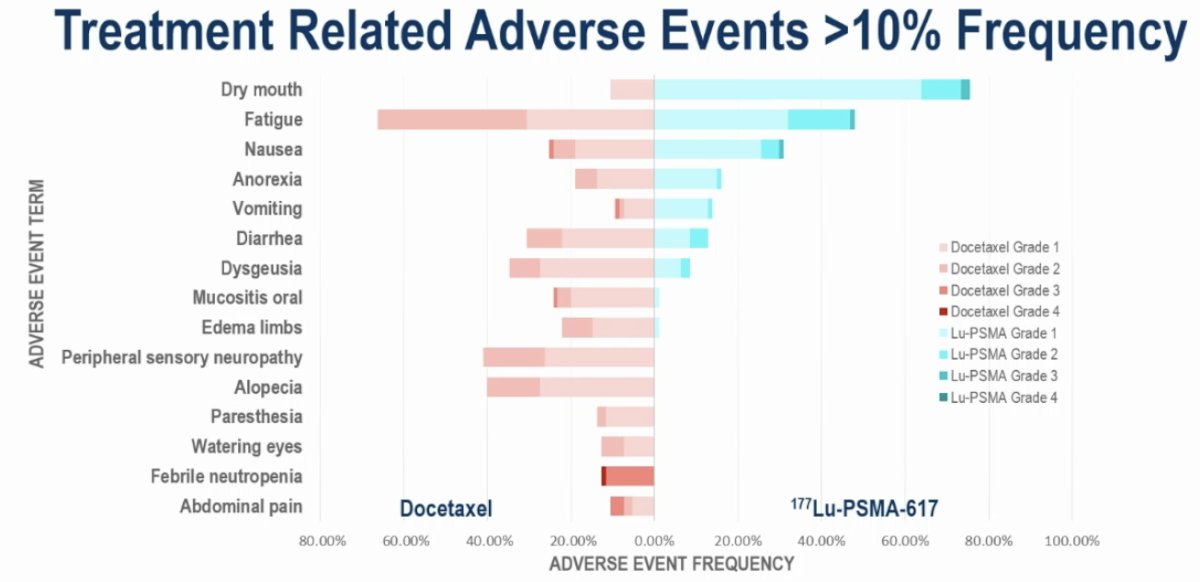
Grade 3-4 TRAEs were more common in the docetaxel arm (34% vs 13%). Two treatment related deaths were observed (sepsis, not otherwise specified), both in the docetaxel arm. The most common adverse events in either arm were as expected for both treatments.
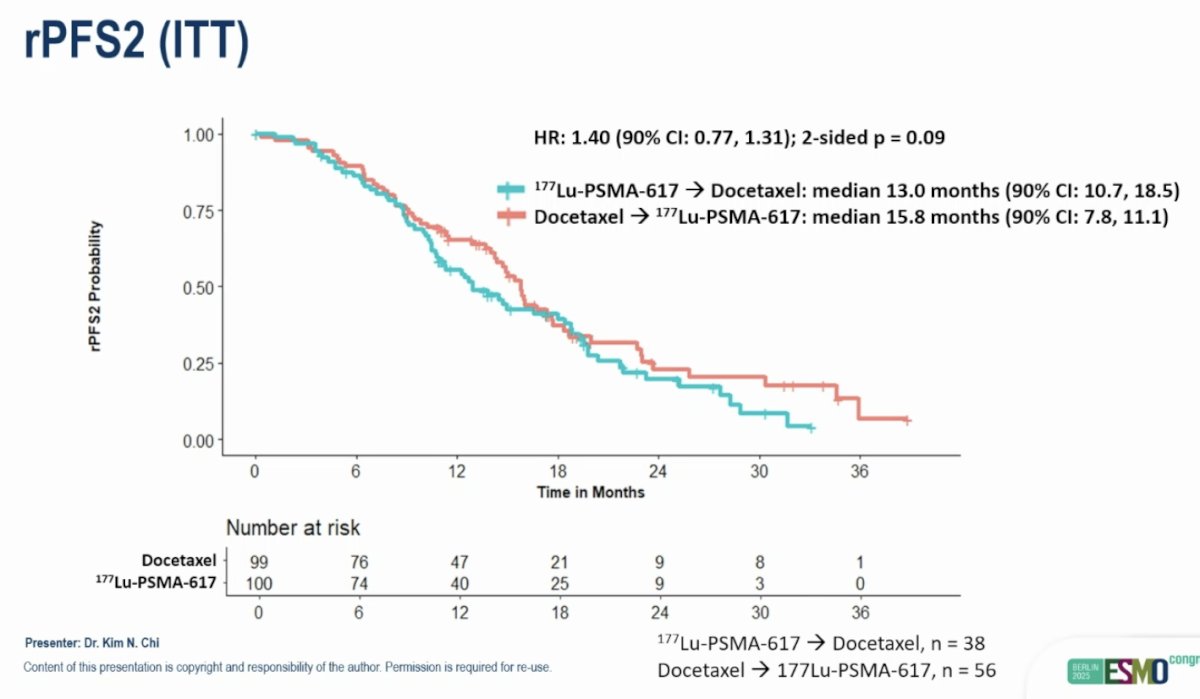
rPFS2 favored patients initially randomized to the docetaxel arm (HR: 1.40, 90% CI: 0.77–1.31, p=0.09):
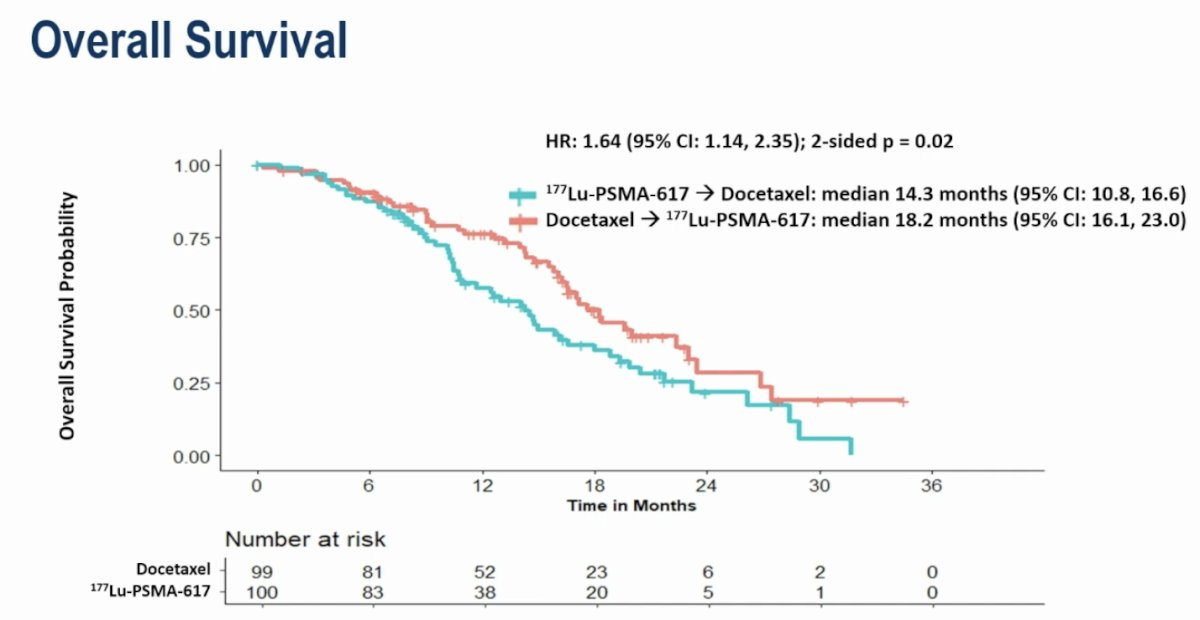
OS also favored patients initially randomized to the docetaxel arm (HR: 1.64, 95% CI: 1.14–2.35, p=0.02). The median OS were 14.3 and 18.2 months, respectively, in favor of initial randomization to docetaxel (i.e., docetaxel 177Lu-PSMA-617):
Dr. Chi concluded his presentation of the CCTG Study PR.21 as follows:
- There was no difference in the primary endpoint of rPFS between 177Lu-PSMA-617 and docetaxel in patients with chemotherapy-naïve mCRPC progressing after an ARPI
- Ther was no difference in time to FACT-P total score deterioration
- Other endpoints favored 177 Lu-PSMA-617
- There was a higher proportion of patients with a PSA decline and measurable disease response
- Fewer grade ≥3 adverse events and treatment discontinuations due to adverse events were seen with initial 177Lu-PSMA-617 randomization
- PSMA PET median SUVmean was prognostic, but not predictive, of rPFS for 177Lu-PSMA-617 and docetaxel
- Overall survival was longer in patients initially randomized to docetaxel
- This is possibly due to a higher treatment cross-over rate from docetaxel to 177Lu-PSMA-617
- Additional analyses with longer follow-up, patient reported outcomes, PSMA PET parameters and serial ctDNA samples are planned
Presented by: Kim N. Chi, MD, Vice President & Chief Medical Officer, British Columbia Cancer Agency, Vancouver Cancer Centre, Vancouver, Canada
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: The PLUDO Study: Comparing First-Line Lutetium vs Docetaxel in Chemo-Naive Metastatic Prostate Cancer - Kim Chi
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial. Lancet. 2024;404(10459):1227–1239.
- Fizazi K, Chi KN, Shore ND, et al. Final overall survival and safety analyses of the phase III PSMAfore trial of [¹⁷⁷Lu]Lu-PSMA-617 versus change of androgen receptor pathway inhibitor in taxane-naive patients with metastatic castration-resistant prostate cancer. Ann Oncol. 2025 Jul 17:S0923-7534(25)00852-X.
- Petrylak DP, Ratta R, Matsubara N, et al. Pembrolizumab plus docetaxel versus docetaxel for previously treated metastatic castration-resistant prostate cancer: the randomized, double-blind, phase III KEYNOTE-921 trial. J Clin Oncol. 2025;43(14):1638–1649.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021; 385(12):1091-1103.