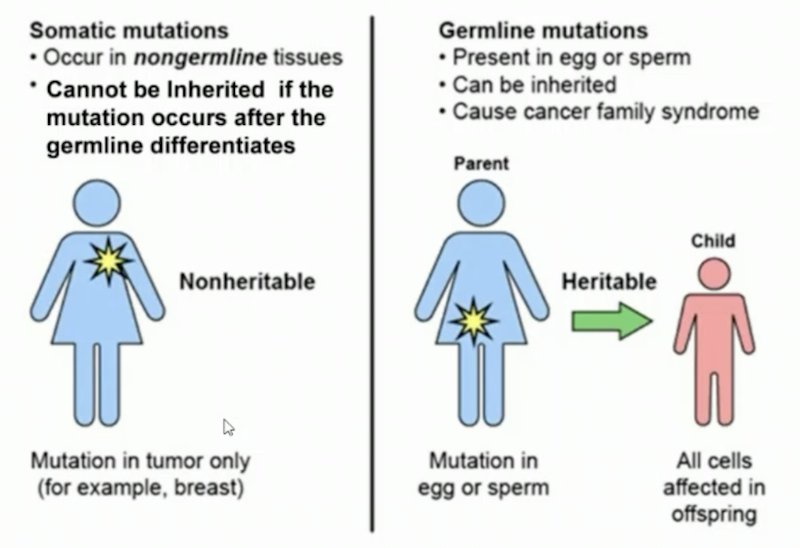
(UroToday.com) The 2025 ESMO annual meeting featured a metastatic castration-resistant prostate cancer (mCRPC) session and a presentation by Dr. Channing Paller discussing germline and somatic genetic testing in advanced prostate cancer. Dr. Paller started her presentation by defining germline versus somatic mutations:
- Germline mutations: present at birth and found in every cell. They are detected from both DNA in any tissue, such as blood (lymphocytes) or saliva (buccal cells + lymphocytes)
- Somatic mutations: acquired in target tissue only. They can evolve over time with disease progression and selection pressures from treatment, and are detected from DNA of target tissue (ie. the tumor)
Based on the classic Pritchard et al.1 study, germline mutations are present in ~12% of metastatic prostate cancer and 6% of localized high risk prostate cancer. Somatic mutations are present in 23% of metastatic castration resistant prostate cancer (mCRPC), and 19% of localized prostate cancer. Dr. Paller notes that there are several practical implications of germline and somatic testing:
- BRCA1 and BRCA2 demonstrate poorer outcomes but are candidates for the following
- PARP inhibitor monotherapy or PARP inhibitor with androgen receptor pathway inhibitor combination therapy
- Platinum-based agents
- Genetic counseling for hereditary cancer syndromes
- MSI-H/dMMR)/tumor mutational burden are candidates for the following:
- PD-1/PDL-1 inhibitor (pembrolizumab)
- Genetic counseling for hereditary cancer syndromes
In the PROfound HRR mutation phase 3 trial,2 among patients with BRCA1/2 or ATM mutations, the median overall survival was 19.1 months versus 14.7 months (HR 0.69, 95% CI 0.50-0.97), which was even further improved in the crossover-adjusted sensitivity analyses (HR 0.42, 95% CI 0.19-0.91):
![In the PROfound HRR mutation phase 3 trial [2], among patients with BRCA1/2 or ATM mutations, the median overall survival was 19.1 months versus 14.7 months (HR 0.69, 95% CI 0.50-0.97), which was even further improved in the crossover-adjusted sensitivity analyses (HR 0.42, 95% CI 0.19-0.91):](/images/com-doc-importer/232-esmo-2025/esmo-2025-germline-and-somatic-genetic-testing-in-advanced-prostate-cancer-practical-considerations-and-challenges/image-1.jpg)
Unfortunately, we still have room for improvement with regards to uptake in germline and somatic testing frequency. A 2022 study from Leith et al. [3] assessing HRR mutation testing in mCRPC patients in the US, Europe, and Japan found that 3/4 of physicians (oncologists, urologists, specialist surgeons) reported access to genetic/genomic testing and just over half were HRR mutation testers. Surveyed physicians reported HRR mutation testing and positivity rates for 1,913 patients, which were 18.1% and 33.7%, respectively. Of patients tested (n = 347), the most common HRR genes tested were BRCA (91.6%) and ATM (47.3%):
![Unfortunately, we still have room for improvement with regards to uptake in germline and somatic testing frequency. A 2022 study from Leith et al. [3] assessing HRR mutation testing in mCRPC patients in the US, Europe, and Japan found that 3/4 of physicians (oncologists, urologists, specialist surgeons) reported access to genetic/genomic testing and just over half were HRR mutation testers. Surveyed physicians reported HRR mutation testing and positivity rates for 1,913 patients, which were 18.1% and 33.7%, respectively. Of patients tested (n = 347), the most common HRR genes tested were BRCA (91.6%) and ATM (47.3%):](/images/com-doc-importer/232-esmo-2025/esmo-2025-germline-and-somatic-genetic-testing-in-advanced-prostate-cancer-practical-considerations-and-challenges/image-2.jpg)
The ASCO Guideline Clinical Insights provides recommendations for somatic and germline testing for metastatic prostate cancer:4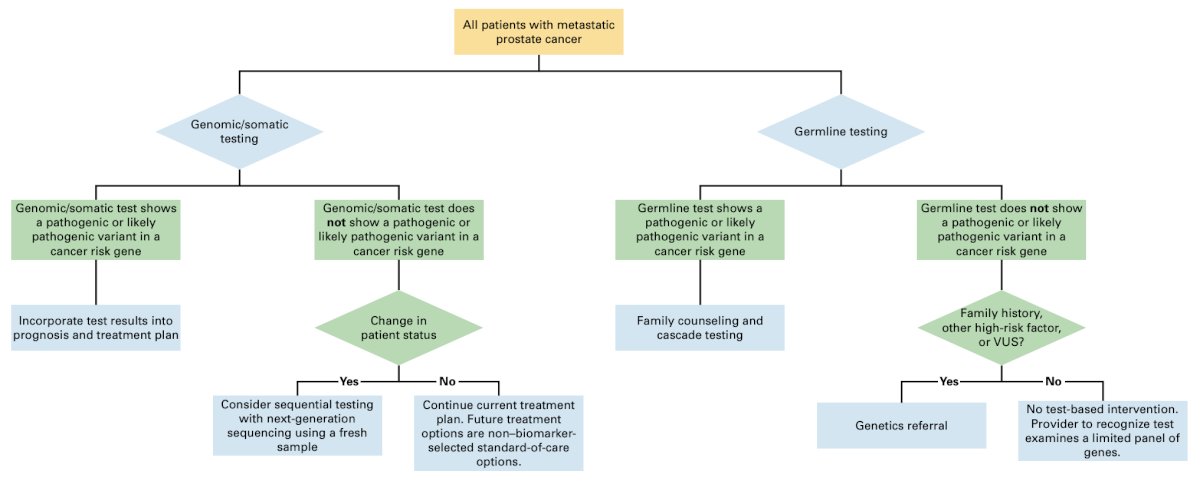
Specific to somatic tumor testing recommendations, NCCN and ASCO also provide the following guidance: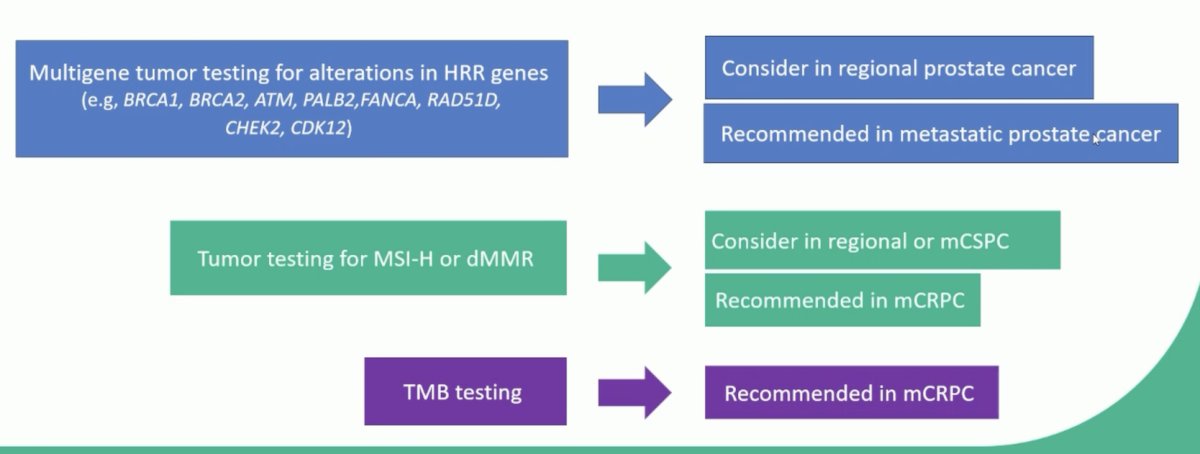
Which test is best clinically? Dr. Paller notes that for initial testing, archival tissue or metastatic biopsy tissue is favored. If there is no accessible metastatic site, ctDNA and/or germline testing should be performed, and if there is minimal residual disease burden (associated with low ctDNA fraction), a metastatic biopsy should be done. The following table highlights the common types and the costs associated with somatic testing: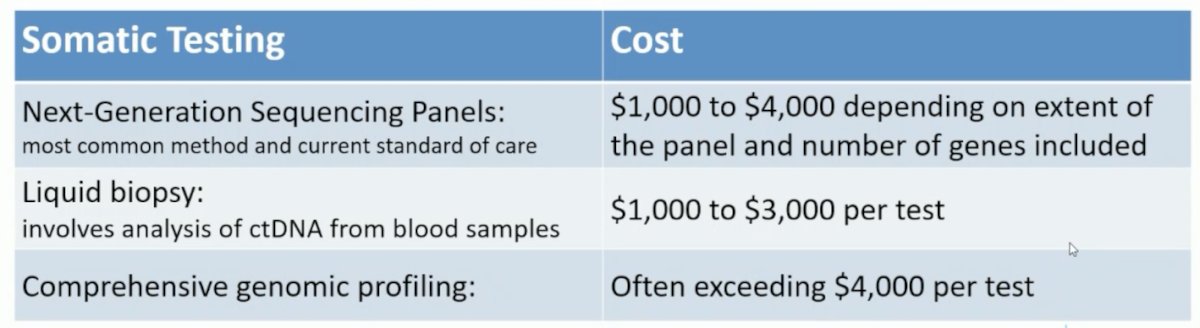
There are several limitations of somatic testing, as highlighted by Dr. Paller:
- Variability in findings based on sample type (formalin-fixed paraffin-embedded tissue or plasma cell-free DNA)
- Technical limitations of tumor sequencing (especially small copy number deletions, and large or complex insertions or deletions)
- Variability in tumor fraction
- Clonal hematopoiesis and false positive results
- Lack of standardization of somatic test reporting which can impact identification of actionable variants and ability to compare results
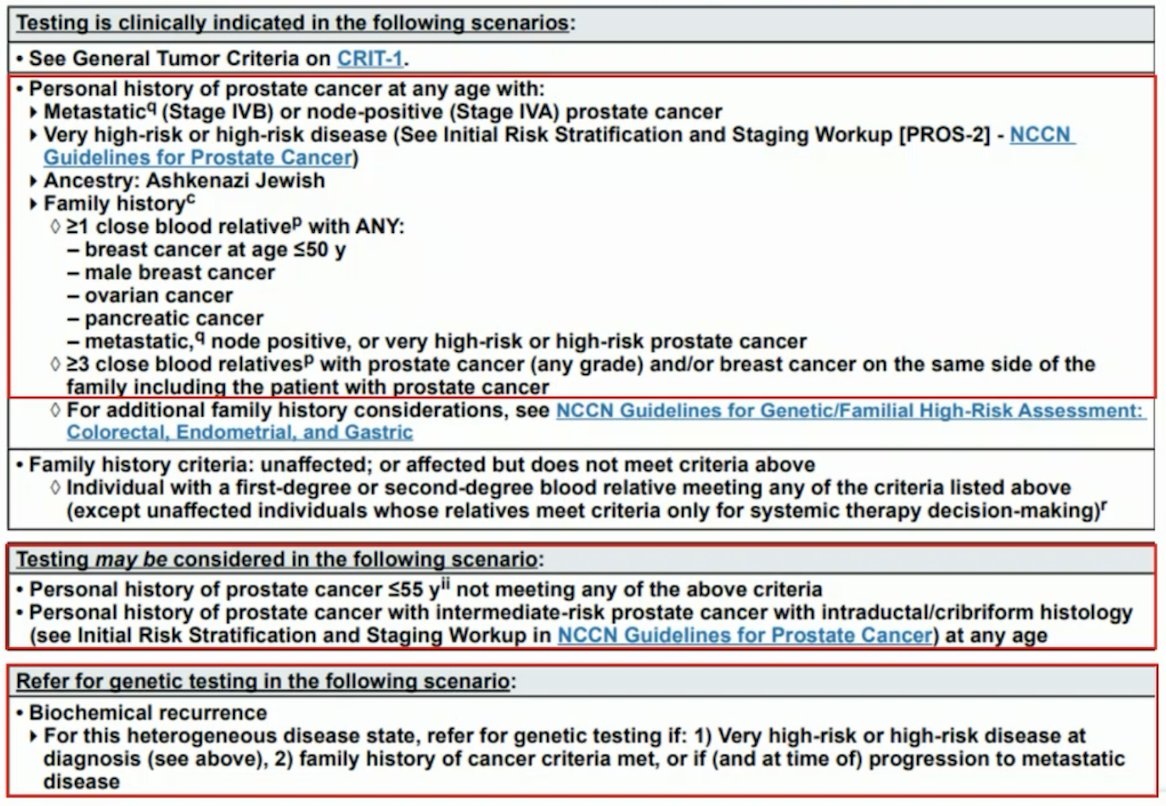
For germline genetic testing, the NCCN guidelines provide comprehensive recommendation for who to refer to a genetic counsellor:
The main professional societies also provide guidance on germline testing based on prostate cancer characteristics: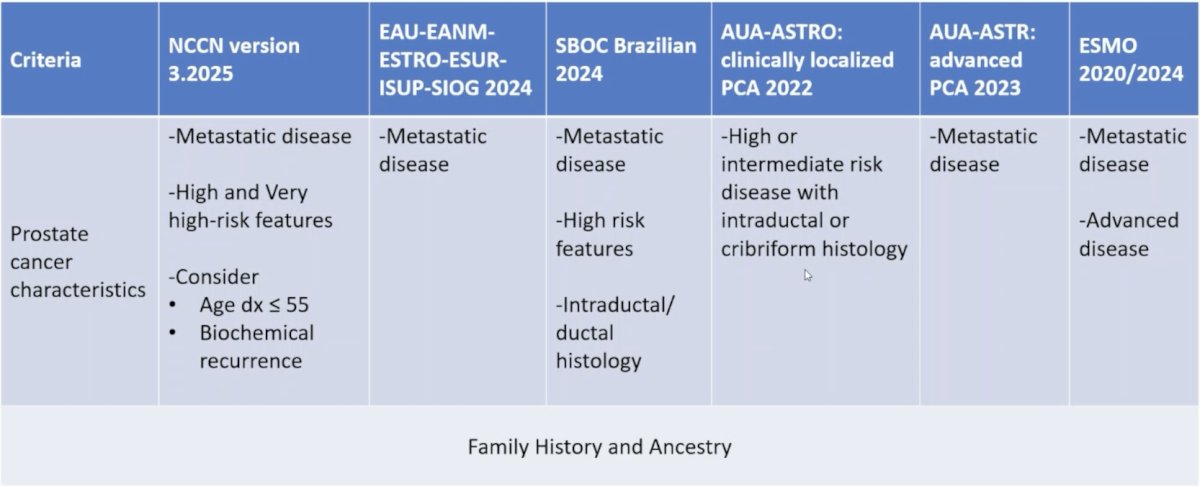
The role of genetic counseling is very important, summarized by Dr. Paller in the following points:
- Pretest counseling must cover purpose of germline testing, hereditary implications, potential to identify additional cancer risks for patient/family, panel testing options, potential results (pathogenic/likely pathogenic, VUS, negative, or inconclusive), legal protections, and the importance of cascade testing
- If pathogenic variant identified: it is strongly recommended that patients be referred to a genetics professional to discuss cancer risks and cascade testing in families
- A multidisciplinary care team: medical oncology, urology, radiation oncology, primary care, and cancer genetics, should collaborate to establish clear pre- and post-test genetic counseling pathways to maximize benefits and minimize harms
The following table highlights the common types and the costs associated with germline testing: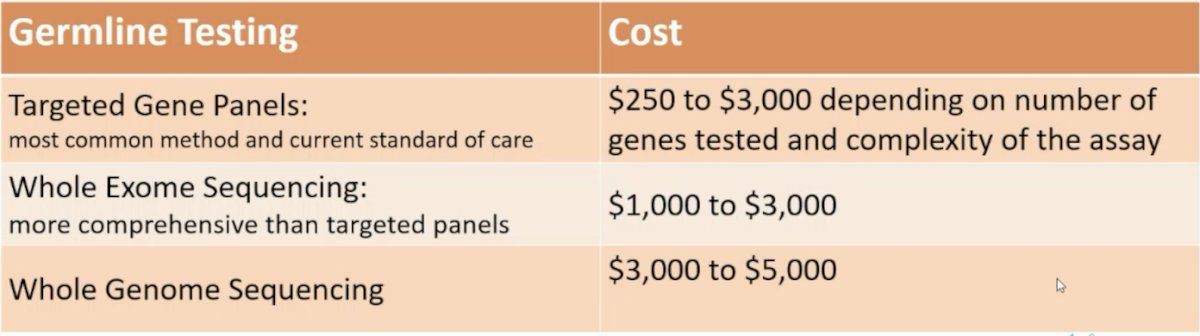
Dr. Paller also noted the following benefits of genetic testing:
- Peace of mind (informative/true negative): confirms a known familial variant is not inherited
- Enables targeted risk-reduction and screening when a pathogenic variant is found
- Guides therapy selection for patients with cancer (e.g., targeted drugs, trial eligibility)
- Informs family (cascade testing): at-risk relatives can test and act
- Clarifies personal cancer history: may contribute to a more accurate prognosis
- Informs risk of additional cancer: can guide surveillance and prevention
However, there are several risks and limitations of genetic testing:
- Psychological stress: burden of knowing one’s own and relatives’ elevated risk
- Resource constraints: Limited clinic time/space, reimbursement, workflow/process hurdles, insufficient educational materials, and limited access to genetic counselors
- Uninformative result (e.g., VUS): uncertainty may cause anxiety or inappropriate actions
- Cost and coverage barriers: for testing and downstream care
- Follow-up burden: ongoing prevention/surveillance can be time-consuming and costly
- Privacy/discrimination concerns: unauthorized sharing of results (insurance/employment)
- Variability in genes: variability in the genes included on multigene panels and variant classification criteria across different clinical genetic laboratories
- Guideline gaps and complexity: may miss at-risk patients
Dr. Paller emphasized, that if resources allow, we should do somatic and germline testing on appropriate patients. This is important given that germline-only testing will miss almost half of BRCA1/2 alterations and will miss most cases of microsatellite instability. Moreover, tumor testing alone may miss pathogenic germline variants. However, there are limitations, such as commercial assays having variable quality and analytic coverage (sensitivity, specificity, ability to evaluate tumor content, variant-allele fractions, and include and/or exclude germline findings).
Dr. Paller concluded her presentation discussing germline and somatic genetic testing in advanced prostate cancer with the following take home points:
- Indications for germline testing:
- Metastatic disease diagnosis, very high-risk disease features and Ashkenazi Jewish descent
- Family history of hereditary cancer syndromes, including hereditary breast and ovarian cancer syndrome, Lynch syndrome, or classical hereditary prostate cancer
- Cascade testing for positive pathogenic variant
- Indications for somatic testing:
- Metastatic disease and being considered for targeted therapy
- All males with advanced metastatic prostate cancer should undergo molecular testing of their tumor and germline DNA to identify potential molecular targets for therapy, particularly for PARP inhibitors, platinum chemotherapy, and immunotherapies
- Archival tissue samples are widely used
- Liquid biopsies, particularly ctDNA assays, are increasingly used in clinical practice; however, the risk for false positives from CHIP remains a significant limitation
- Consider repeat metastatic biopsies – there may be new actionable somatic mutations
Presented by: Channing Paller, MD, Johns Hopkins University, Baltimore, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
References:
- Pritchard CC, Mateo J, Walsh MF, et al. Inherited DNA-Repair gene mutations in men with metastatic prostate cancer. N Engl J Med. 2016;375(5):443-453.
- de Bono J, Mateo J, Fizazi K, et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2020 May 28;382(22):2091-2102.
- Leith A, Ribbands A, Kim J, et al. Real-world homologous recombination repair mutation testing in metastatic castration-resistant prostate cancer in the USA, Europe, and Japan. Future Oncol. 2022 Mar;18(8)937-951.
- Giri VN, Rumble RB, Yu EY, et al. Germline and somatic genomic testing for metastatic prostate cancer: ASCO Guideline Clinical Insights. JCO Oncol Pract. 2025 Apr 16:OP2500186.