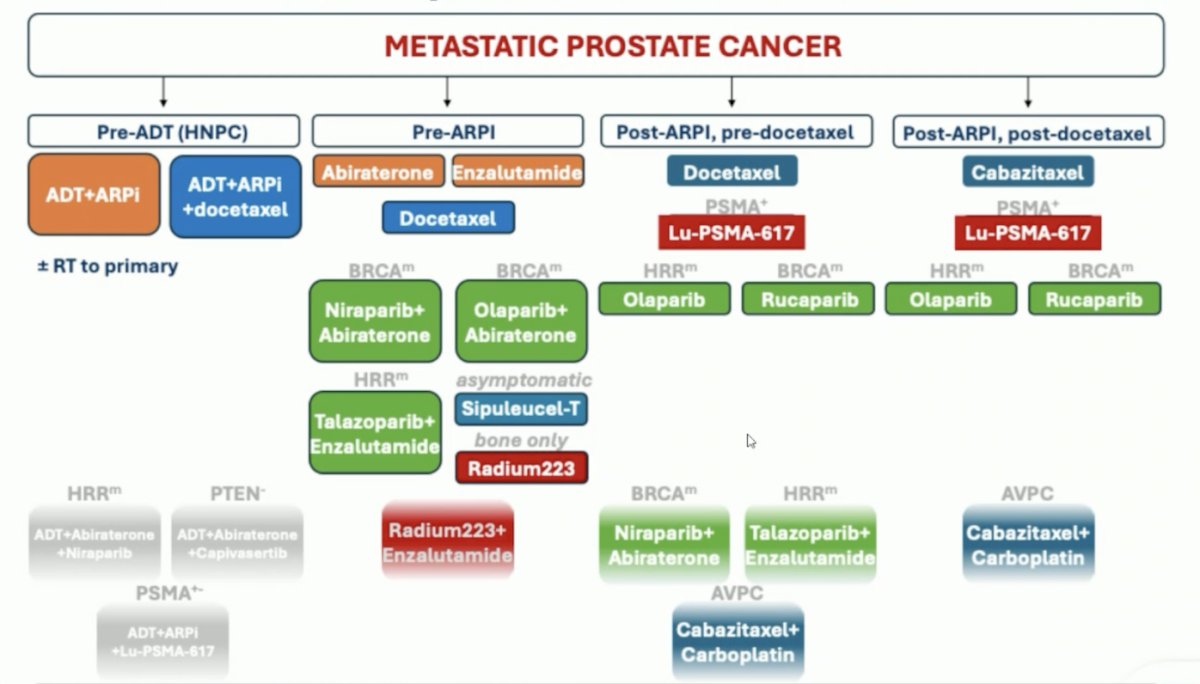
(UroToday.com) The 2025 ESMO annual meeting featured a biomarker-based personalization in metastatic prostate cancer session and a presentation by Dr. Ana Aparicio discussing aggressive variant prostate cancer. Dr. Aparicio started her presentation by highlighting the treatment landscape of metastatic prostate cancer based on approved and what are likely to be approved regimens:
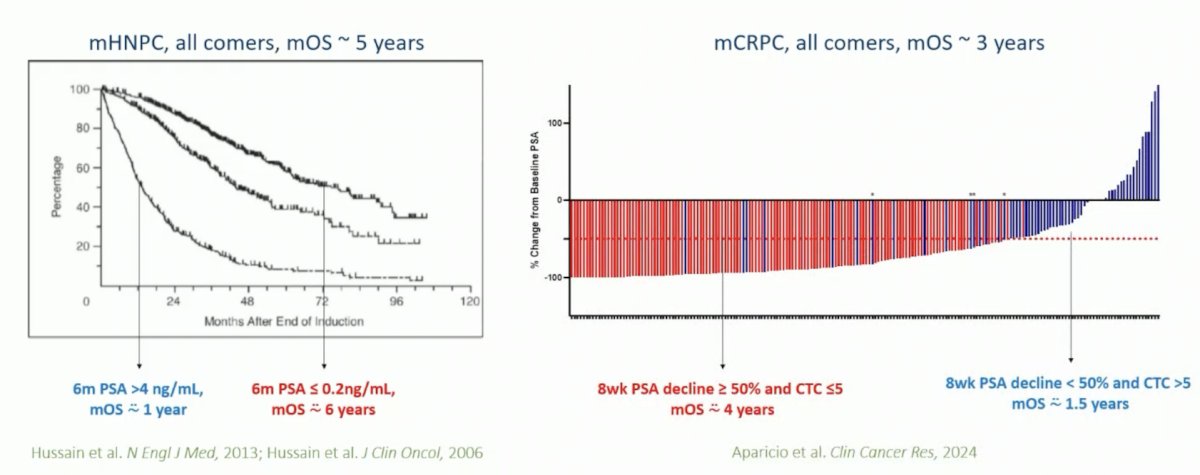
Indeed, androgen responsiveness remains a prostate cancer classifier across disease states, with a median overall survival amongst all comers in metastatic hormone naïve prostate cancer of ~5 years, compared to ~3 years in metastatic castration resistant prostate cancer (mCRPC):
Aggressive variant prostate cancer is a framework to study ‘androgen indifferent’ prostate cancers. Aggressive variant prostate cancer criteria are as follows:
- Small cell carcinoma morphology
- Visceral metastases only
- Lytic bone metastases
- Bulky nodes or prostate mass
- Low PSA relative to volume
- Elevated serum CEA or LDH
- Primary castration-resistance
Dr. Aparicio highlighted several lessons learned through correlative rich phase I/II clinical trials in aggressive variant prostate cancer:
- Characterized by combined tumor suppressor defects (TP53, RB1, PTEN)
- Benefitted by platinum-based combinations
- Aggressive variant prostate cancer heterogeneity and potential metabolic dependencies
- Progression free survival and overall survival benefit from the addition of alpha-PD1 to carboplatin-carboplatin-niraparib in a subset
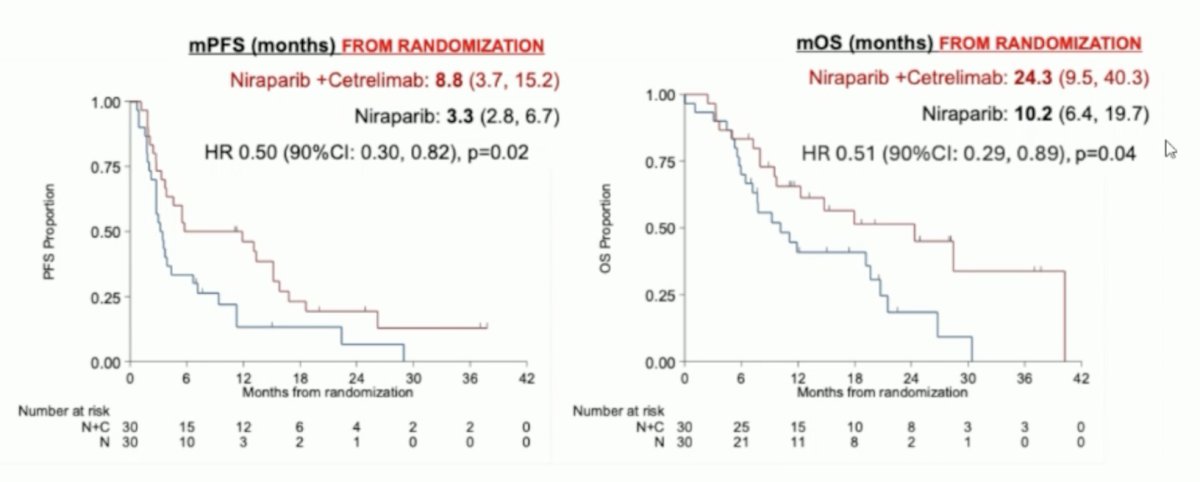
At ASCO 2025, Dr. Aparicio presented data from C3NIRA, a randomized phase II study of carboplatin-cabazitaxel-cetrelimab induction followed by niraparib +/- cetrelimab maintenance in men with aggressive variant prostate cancers. Despite the small sample size, the addition of cetrelimab (αPD1) to niraparib maintenance following induction significantly improved both progression-free and overall survival in men with aggressive variant prostate cancer. The median progression free survival from randomization was 8.8 months in the niraparib + cetrelimab arm compared to 3.3 months with niraparib alone (HR 0.50, 90% CI 0.30–0.82; p = 0.02), and the median overall survival was also notably longer with combination therapy at 24.3 months versus 10.2 months with niraparib alone (HR 0.51, 90% CI 0.29–0.89; p = 0.04):
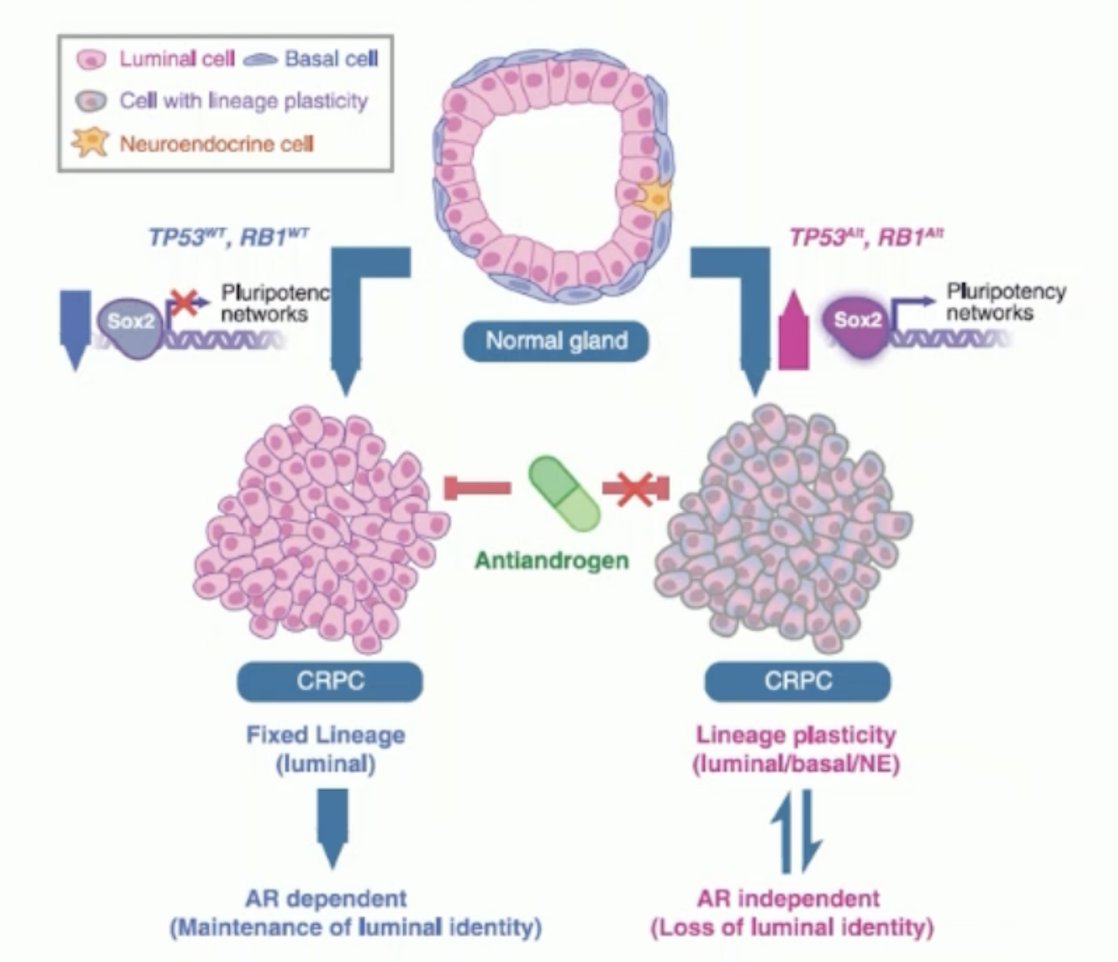
Dr. Aparicio notes that the combined tumor suppressor defects characterize clinically defined aggressive variant prostate cancer, specifically TP53, PTEN, and RB1.1 Indeed, previous studies have shown that the combined defects of Tp53, Pten, and Rb1 reproduce the aggressive variant prostate cancer phenotype:
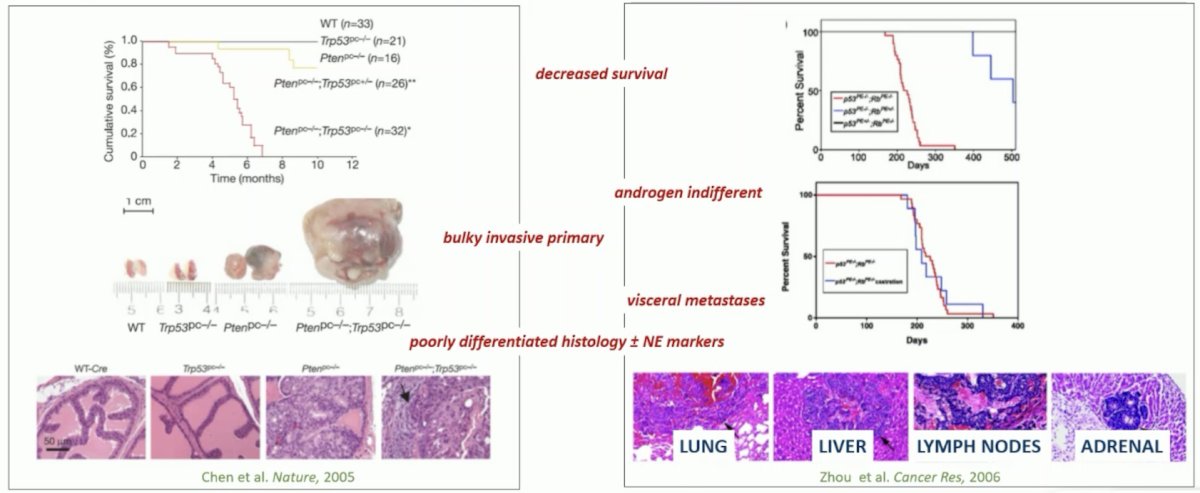
Furthermore, these combined defects also promote lineage plasticity and androgen indifference:
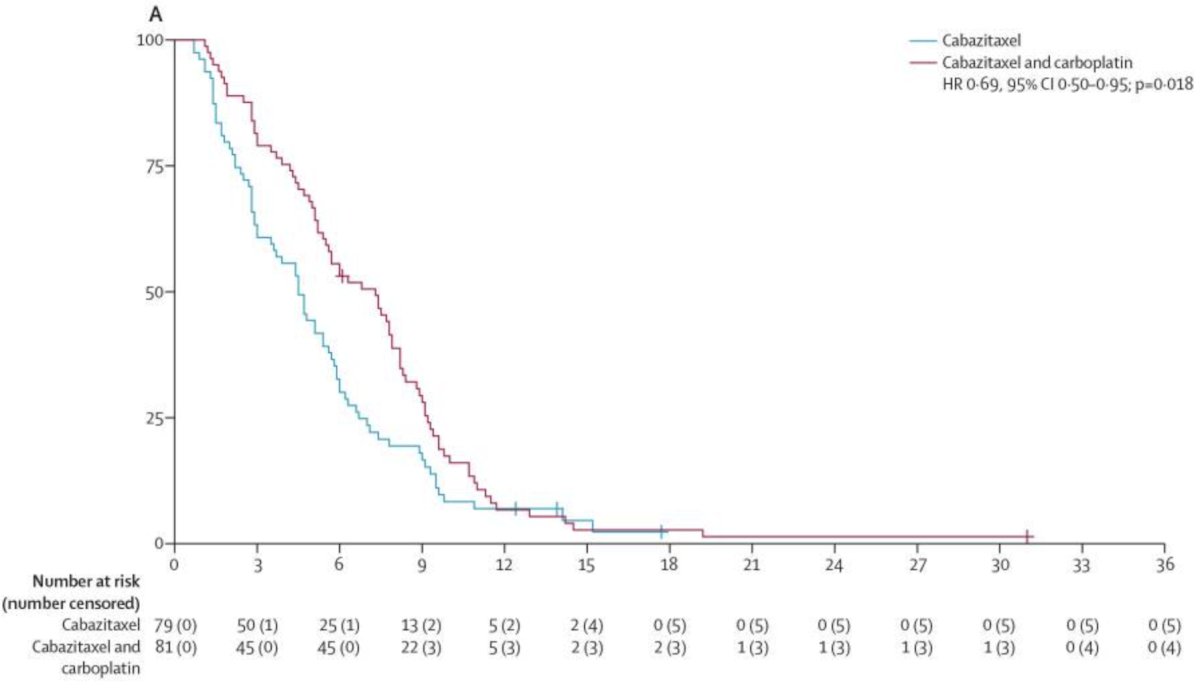
Dr. Aparicio highlighted that aggressive variant prostate cancer mutations do benefit from the addition of carboplatin to cabazitaxel based on data from a randomized, open-label, phase 1-2 trial,2 with a 2.8 month improvement in progression free survival (HR 0.69, 95% CI 0.50-95):
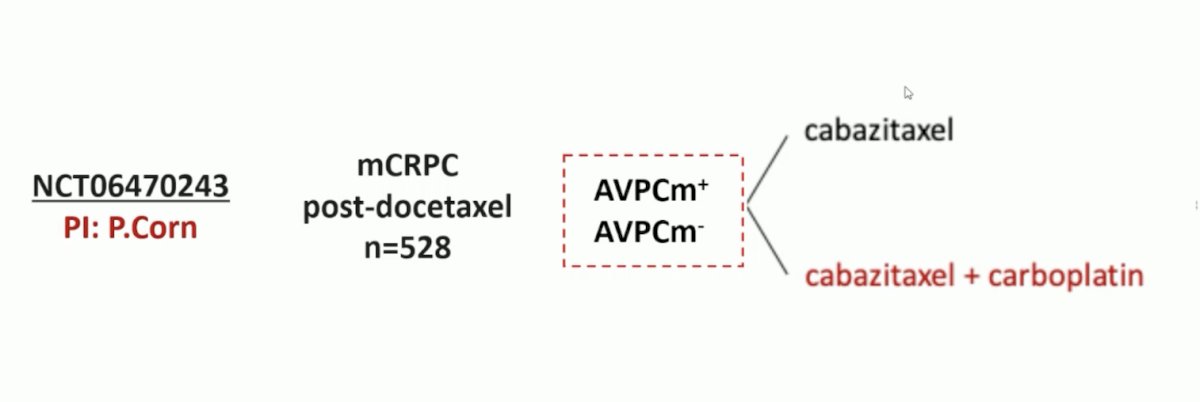
As such, SWOG 2312 is a randomized phase III trial that will assess cabazitaxel +/- carboplatin in men with mCRPC, stratified by aggressive variant prostate cancer mutations:
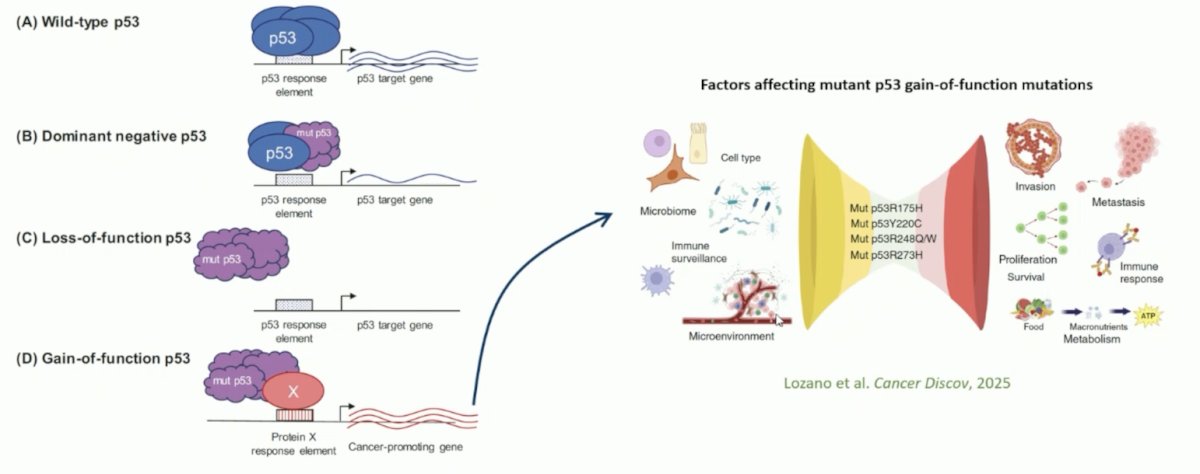
Specific to p53 mutations, diverse mechanisms account for the oncogenic activity of mutant p53 proteins:
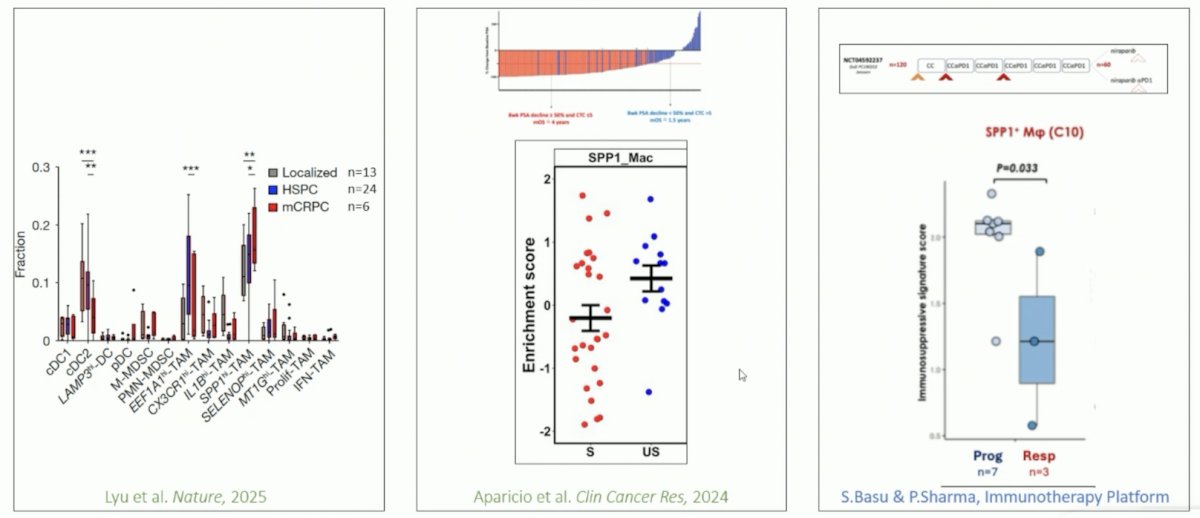
Other targets include SPP1hi tumor associated macrophages, that are enriched in resistant tumors:
Ultimately, Dr. Aparicio emphasized that it is time to work towards a biologically based, therapeutically relevant prostate cancer classification, as highlighted in the following figure:

Dr. Aparicio concluded her presentation discussing aggressive variant prostate cancer with the following take home points:
- The aggressive variant prostate cancer criteria serve to select patients for prospective clinical trials interrogating biology relevant to androgen indifferent prostate cancer
- The aggressive variant prostate cancer mutation is associated with a distinct androgen indifferent/plasticity phenotype in preclinical models and worse outcomes in men with advanced prostate cancers. However, its utility as a disease classifier remains to be validated prospectively
- A detailed understanding of the relevant alterations of the aggressive variant prostate cancer mutation components (TP53, RB1, PTEN) – and how to optimally assess them – is needed
- The addition of tumor microenvironment biomarkers may be required to arrive at biologically-based, therapeutically-relevant classifying signatures
Presented by: Ana Aparicio, MD, The University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: Clinical and Molecular Criteria for Aggressive Variant Prostate Cancer - Ana Aparicio
References:
- Aparicio AM, Shen L, Tapia ELN, et al. Combined tumor suppressor defects characterize clinically defined aggressive variant prostate cancer. Clin Cancer Res. 2016 Mar 15;22(6):1520-1530.
- Corn PG, Heath EI, Zurita A, et al. Cabazitaxel plus carboplatin for the treatment of men with metastatic castration-resistant prostate cancers: a randomized, open-label, phase 1-2 trial. Lancet Oncol. 2019 Oct;20(10):1432-1443.