(UroToday.com) The 2025 ESMO annual meeting featured a prostate cancer trials in progress session and a presentation by Dr. Guillaume Grisay discussing EORTC GUCG 2238 de-escalate, a pragmatic trial to revisit intermittent ADT in metastatic hormone-naïve prostate cancer in the era of new androgen receptor pathway inhibitors. The development of androgen receptor pathway inhibitors – abiraterone acetate, apalutamide, darolutamide, and enzalutamide – has profoundly reshaped the management of metastatic hormone-naïve prostate cancer (mHNPC). Seven trials have demonstrated that combining these drugs with ADT reduces the risk of death by 20 to 40%, delays the need for further treatment and improves health related quality of life. However, these trials are subject to two critical limitations: treatment duration and patient selection. Treatment typically continues until biochemical, radiological, or clinical progression occurs, sometimes many years after initiation, potentially exposing patients to chronic side effects that impact their quality of life. Furthermore, registration trials often include patient populations that are not representative of the general population. Several sub-analyses of these registration trials have shown that patients achieving a PSA level of ≤0.2 ng/ml have prolonged overall survival. In this study, the hypothesis was that patients reaching a PSA of ≤ 0.2 ng/ml might benefit from treatment interruption without compromising overall survival.
The primary goal of this academic-led, open-label, pragmatic, randomized phase III study is to investigate whether intermittent androgen blockade can be safely administered to mHNPC patients who reached a PSA ≤ 0.2 ng/mL at 6 to 12 months of continuous maximal androgen blockade, as compared to continuing maximal androgen blockade:
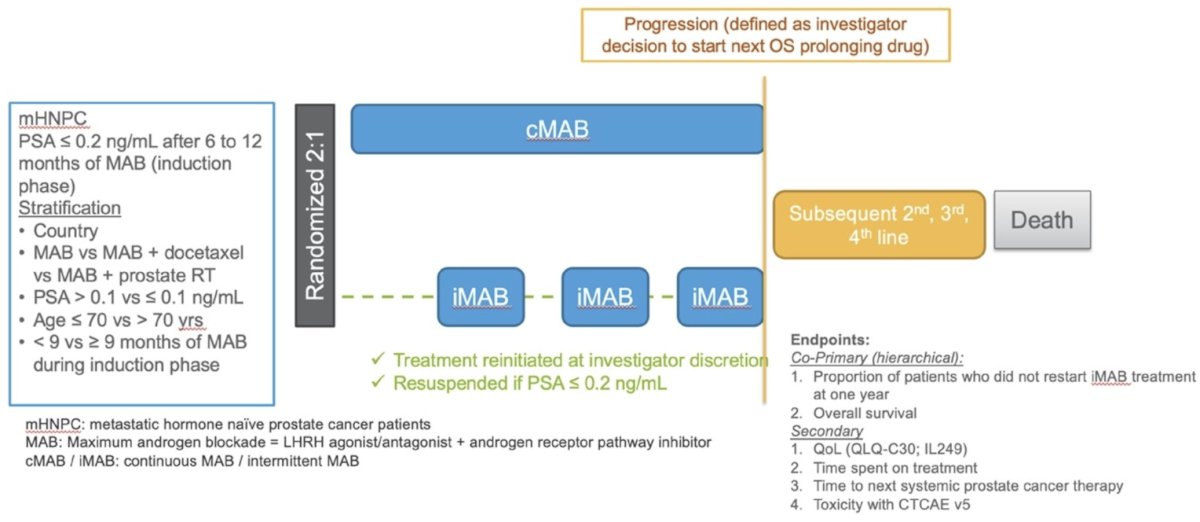
The co-primary endpoints are:
- The proportion of patients who do not need to restart their maximal androgen blockade within one year of interruption is not less than 70%, and
- Overall survival using an intermittent androgen blockade regimen at three years is non-inferior to continuous treatment
Secondary objectives include toxicity comparisons, health related quality of life, and assessing the impact on treatment resources of intermittent androgen blockade. The study will include 1,600 patients treated by continuous maximal androgen blockade for mHNPC for 6 to 12 months presenting with a PSA ≤ 0.2 ng/mL. EORTC GUCG 2238 – De-Escalate is currently open in the first wave of participating countries, including Denmark, France and Spain. So far, 37 patients were included. The second wave of countries is expected to open in the first quarter of 2026.
Clinical trial identification: NCT05974774.
Presented by: Guillaume Grisay, Centres Hospitaliers Universitaires, Woluwe-Saint-Lambert, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025