(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st was host to the Poster presentation session. Kim J. Van der Velden presented the poster Treatment intensification in the metastatic castration-sensitive prostate cancer (mCSPC) landscape: real-world evidence from 4,559 patients in the CAPRI-3 registry.
Current guidelines for metastatic castration-sensitive prostate cancer recommend treatment intensification (TI) based on disease volume, typically through the addition of life-prolonging drugs (LPDs) such as ARPIs, docetaxel, or abiraterone, or the use of external-beam radiation therapy (EBRT) in combination with androgen deprivation therapy (ADT). Dr Van der Velden noted the purpose of the study was to evaluate real-world treatment patterns and determine the association between treatment intensification and overall survival (OS) among patients with mCSPC, providing insight into how guideline-recommended strategies are being implemented in clinical practice.
The analysis included patients diagnosed with mCSPC between 2016 and 2021, using data from the Dutch CAPRI-3 registry encompassing 20 participating hospitals. Treatment intensification (TI) was defined as the addition of chemotherapy, androgen receptor pathway inhibitors (ARPIs), or external-beam radiation therapy (EBRT) to androgen deprivation therapy (ADT). Disease volume was categorized according to the CHAARTED criteria.
Key study outcomes included the use of TI and overall survival (OS). Statistical analyses involved multiple imputation to address missing data, binary logistic regression to identify factors associated with TI, and uni- and multivariable Cox proportional hazards models to evaluate the association between TI and OS.
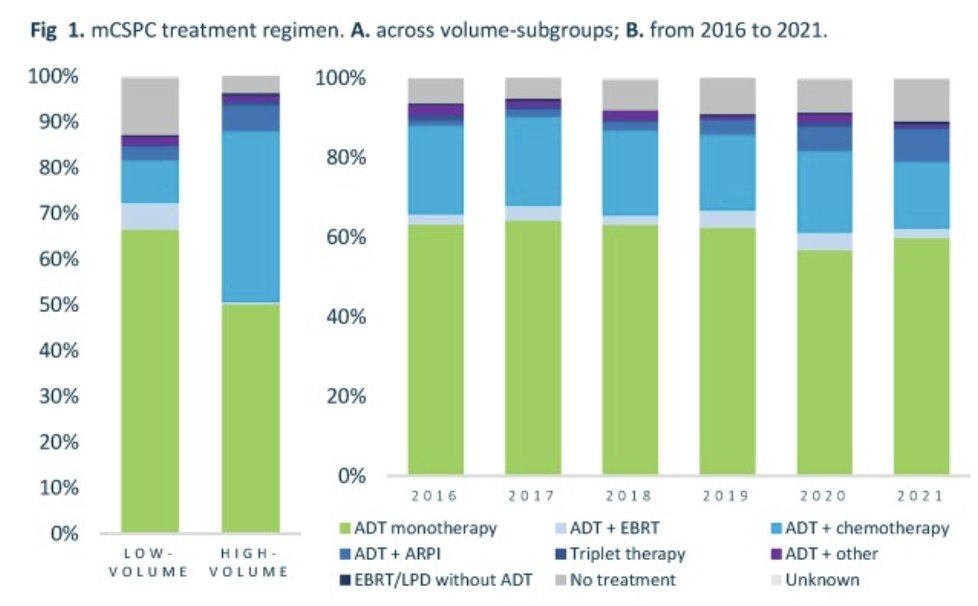
Among 3,799 patients with known disease volume, 56% had low-volume and 44% had high-volume mCSPC. ADT monotherapy remained the most common treatment approach, used in 62% of cases, indicating that a large proportion of patients did not receive treatment intensification (TI). TI was more frequently applied in patients with high-volume disease (45%) compared to those with low-volume disease (20%) as illustrated in the figure below.
Over time, between 2016 and 2021, the use of ADT monotherapy remained relatively stable (57%–65%). While chemotherapy-based TI slightly declined from 22% to 17%, the adoption of ARPI-based intensification gradually increased from 1% to 8%, reflecting a shift in real-world practice toward incorporating novel hormonal therapies.
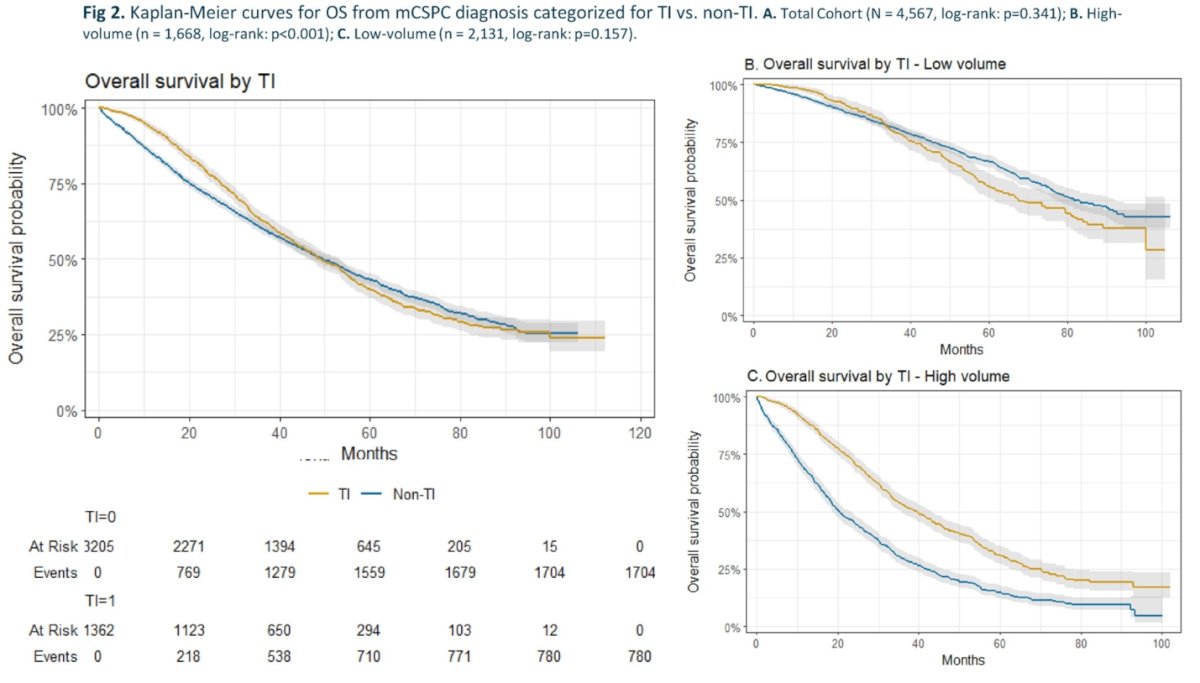
TI did not significantly improve OS in the total mCSPC cohort (HR 0.94, p=0.313). However, when stratified by disease volume, a clear OS benefit emerged among patients with high-volume disease, where median OS was 41.6 months for those receiving TI versus 26.3 months with ADT monotherapy (p<0.001). In contrast, patients with low-volume disease did not experience a significant OS advantage with TI (p=0.157). These findings highlight that the survival benefit of intensification appears primarily driven by high-volume disease, aligning with previous trial data suggesting that disease burden should guide the use of intensified treatment strategies.
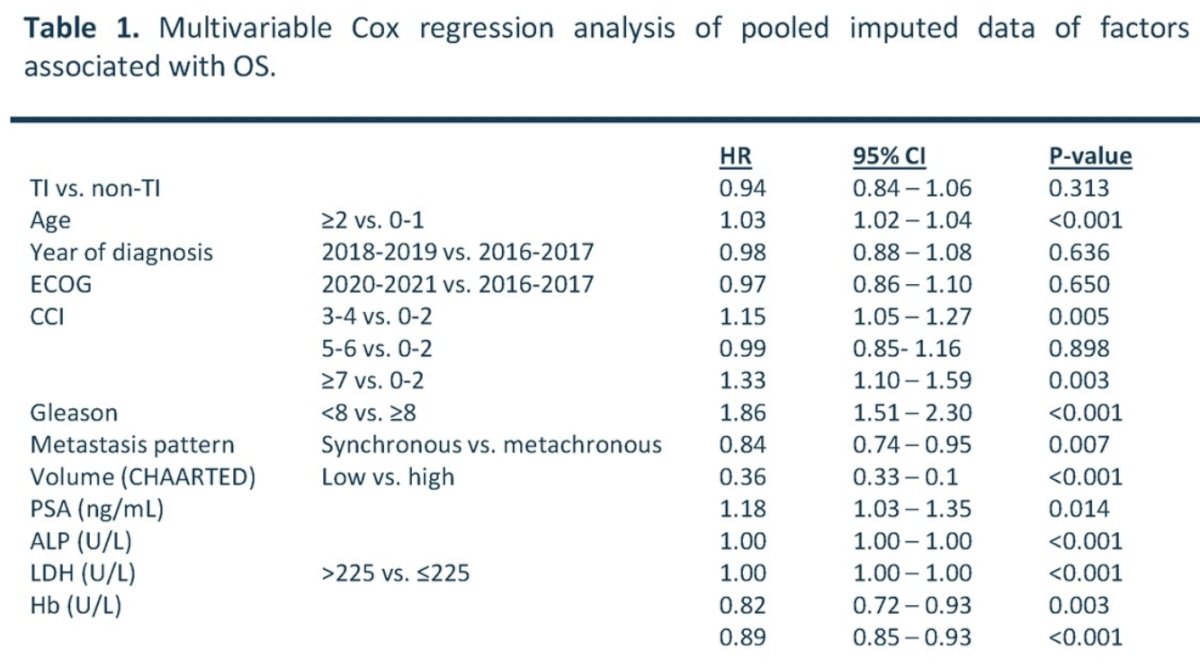
TI was more commonly administered to younger and fitter patients, as well as those with more aggressive disease characteristics, specifically, Gleason ≥8, high-volume or synchronous metastases, and PSA levels ≥20 ng/mL. Despite this, in multivariable Cox regression, TI was not independently associated with improved overall survival (OS) (HR 0.94, p=0.313).
Among all evaluated factors, low-volume disease emerged as the strongest predictor of better OS (HR 0.36, 95% CI 0.33–0.41), underscoring the prognostic importance of disease burden in mCSPC. Other independent predictors of poorer OS included older age, higher comorbidity index, elevated PSA, ALP, and LDH levels, lower hemoglobin, and synchronous metastases as listed in the table below.
Dr. van der Velden concluded their poster presentation with the following key messages:
- There are notable discrepancies between real-world practice, treatment guidelines, and observed survival outcomes in mCSPC.
- Treatment intensification (TI) rates remain low in routine clinical practice, especially among patients with low-volume disease.
- High-volume patients appear to derive the greatest overall survival (OS) benefit from treatment intensification.
- Disease volume emerged as the strongest predictor of survival, underscoring the importance of volume-stratified treatment strategies.
- These results support a tailored approach to therapy based on disease burden and patient fitness rather than a uniform treatment model.
Presented by: Kim J. Van der Velden, BSc, PhDc, PhD Candidate Urology and Master Student, Nijmegen, Netherlands
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.