(UroToday.com) The 2025 ESMO annual meeting featured a prostate cancer session and a presentation by Dr. Scott Tagawa discussing dose-escalation + expansion trial of fractionated and multiple-dose PSMA-targeted alpha radionuclide 225Ac-J591 for metastatic castration-resistant prostate cancer (mCRPC). The first prospective alpha-PSMA trial was single-dose 225Ac-J591 reported in the Journal of Clinical Oncology in 2024.1 Fractionated (dose dense) approaches to treatment with radioligand therapy appear to be attractive and are now being employed in randomized trials. The most common approach is to administer cycles of therapy approximately 6 weeks apart. At ESMO 2025, Dr. Tagawa and colleagues reported mature results of a parallel cohort study of fractionated and multiple-dose regimens.
Eligibility criteria included patients with ECOG performance status 0-2, intact organ function, and progressive mCRPC after androgen receptor pathway inhibitor and chemotherapy (or unfit/refused). PSMA PET/CT scans were performed, but were not used for eligibility. In the fractionated cohort, patients received one dose-dense cycle (45-65 KBq/Kg) on D1 and D15, and in the multiple-dose cohort, 225Ac-J591 (45-65 KBq/Kg) was given every 6 weeks for up to 4 cycles. Follow up imaging with CT/MRI, bone scan, and 68Ga-PSMA-11 PET/CT was done at 12 weeks, then CT/MRI and bone scan were done every 12 weeks until progression or withdrawal. The primary objectives of this trial were an assessment of dose limiting toxicity and identifying the recommended phase 2 dose. Expansion enrollment was undertaken to further define safety and preliminary efficacy outcomes, including PSA, progression free survival, overall survival.
Overall, there were 60 patients treated: 42 in the fractionated cohort (33 in dose-escalation 45-65 KBq/Kg/dose, 9 in the expansion cohort), and 18 in the multiple-dose escalation cohort (45-65 KBq/Kg/dose). The median age was 73 years (IQR 67-80), the median PSA was 69 ng/mL (IQR 10-282), 32 (53%) patients were CALGB (Halabi) high risk, and 23 (38%) were intermediate risk. In terms of metastatic distribution, 88% had bone metastases, 62% nodal metastases, 13% lung metastases, and 13% liver metastases. Prior treatments included 60% of patients receiving ≥2 androgen receptor pathway inhibitors, 70% received ≥1 lines of prior chemotherapy, 13% prior PARP inhibitor, 12% prior radium-223, and 20% prior 177Lu-PSMA-617. The median PSMA PET SUVmax was 42 (IQR 27-85), the median SUVmean was 7.9 (IQR 5-12), and the median total tumor volume was 341 mL (IQR 91-921):

In the fractionated cohort, one dose limiting toxicity occurred at 50 KBq/Kg (grade 4 thrombocytopenia), 2 dose limiting toxicities at 65 KBq (grade 2 thrombocytopenia >2 weeks, grade 4 thrombocytopenia), and one dose limiting toxicity at 60 KBq (grade 4 thrombocytopenia). Based on these results, the recommended phase 2 dose was 60 KBq/Kg x2. Overall survival for < the recommended phase 2 dose was 12.9 months versus 16.0 months with > the recommended phase 2 dose (p = 0.09):

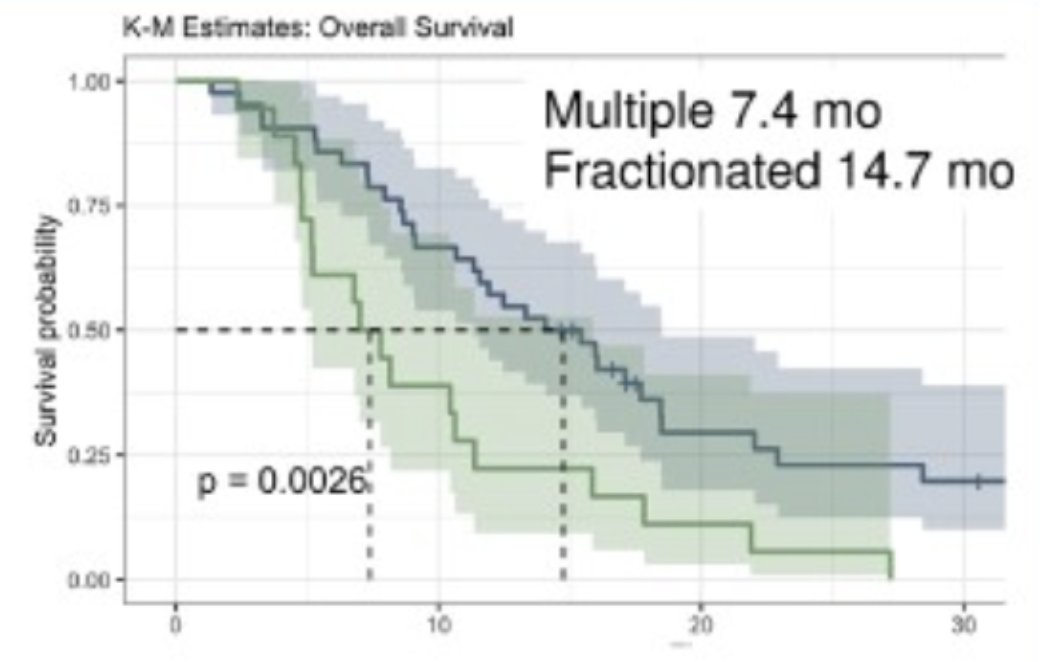
In the multiple-dose cohort, the median number of cycles was 2 (range 1–4), with 2 dose limiting toxicities at 65 KBq/Kg (grade 1 and grade 3 thrombocytopenia), 3 dose limiting toxicities at 55 KBq (1 grade 3 and 2 grade 4 thrombocytopenia), 2 dose limiting toxicities at 45 KBq (grade 1 and grade 2 thrombocytopenia). The median progression free survival was 2.69 (95% CI 1.8-5.6) and median overall survival was 7.4 months (95% CI 5.2-15.9), which was significant worse compared to fractionated dosing (14.7 months; p = 0.0026):
Dr. Tagawa concluded his presentation discussing dose-escalation + expansion trial of fractionated and multiple-dose PSMA-targeted alpha radionuclide 225Ac-J591 for mCRPC with the following take home points:
- 225Ac-J591 in a dose-dense fractionated regimen appears safe with preliminary efficacy despite lack of PSMA pre-selection (and allowing 177Lu-PSMA-617)
- Multiple doses every 6 weeks are not recommended given timing of blood count nadir
- A multicenter study is underway to validate fractionated results with or without prior 177Lu-PSMA-617
Presented by: Scott T. Tagawa, MD, MS, FACP, FASCO, Weill-Cornell Medicine, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References: