(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to the Poster presentation session. Dr. Fernando S. Monteiro presented the poster Opportunities to Optimize the Systemic Treatment for Metastatic Castration Resistant Prostate Cancer (mCRPC) in Low-Income Countries: A Seven-Years Analysis of the Brazilian Public Health System (BPHS).
Dr. Monteiro began his poster presentation by emphasizing that prostate cancer remains the most common malignancy among men worldwide. As novel therapies are developed and incorporated into international guidelines, treatment-related costs have escalated, creating disparities in access particularly for patients in Low- and Middle-Income Countries (LMICs). Within the Brazilian Public Health System (BPHS), docetaxel is broadly accessible, whereas abiraterone remains limited in availability for metastatic castration-resistant prostate cancer (mCRPC). In this setting, several treatment strategies without proven survival benefit continue to be used in routine clinical practice.
This was an observational retrospective study. The study included patients aged ≥18 years with histologically confirmed prostate adenocarcinoma and metastatic castration-resistant prostate cancer (mCRPC; any T, any N, M1) treated within the Brazilian Public Health System between January 1, 2017, and December 31, 2023. Data were obtained from the Department of Health Informatics of the Ministry of Health of Brazil.
A total of 38,851 patients with mCRPC were included in the analysis. The median duration of treatment (DoT) was 20.5 months, and the cumulative expenditure associated with castration-resistant therapy was US$333.2 million. Of these, 31,430 patients (81%) received Treatment Protocols with Survival Benefit (TPSB), while 7,421 patients (19%) were treated with Interventions Lacking Substantial Empirical Evidence (ILSEE) for survival benefit.
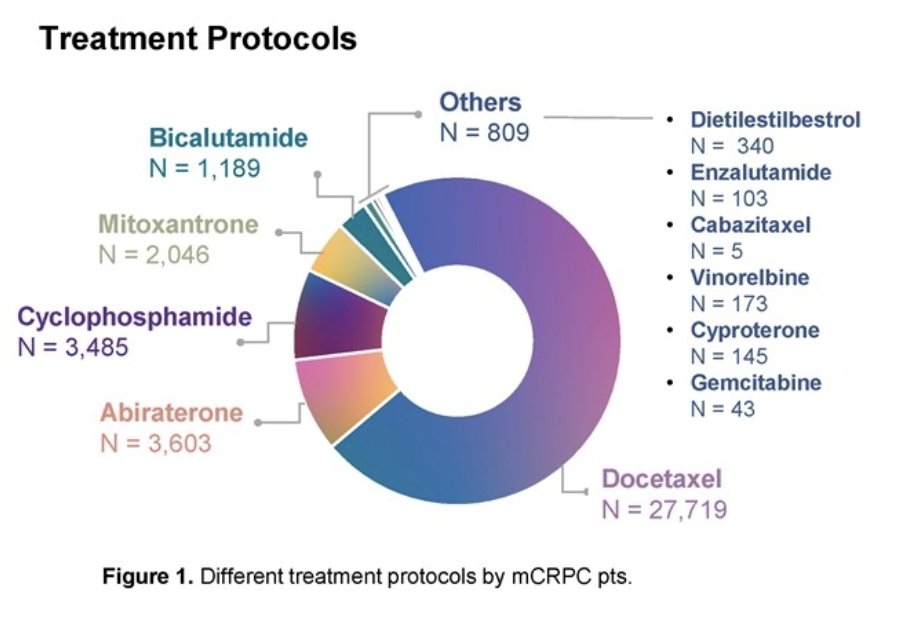
Docetaxel was the most frequently administered treatment (n=27,719), followed by abiraterone (n=3,603), cyclophosphamide (n=3,485), mitoxantrone (n=2,046), and bicalutamide (n=1,189). Less commonly used agents included diethylstilbestrol, vinorelbine, cyproterone, gemcitabine, cabazitaxel, and enzalutamide.
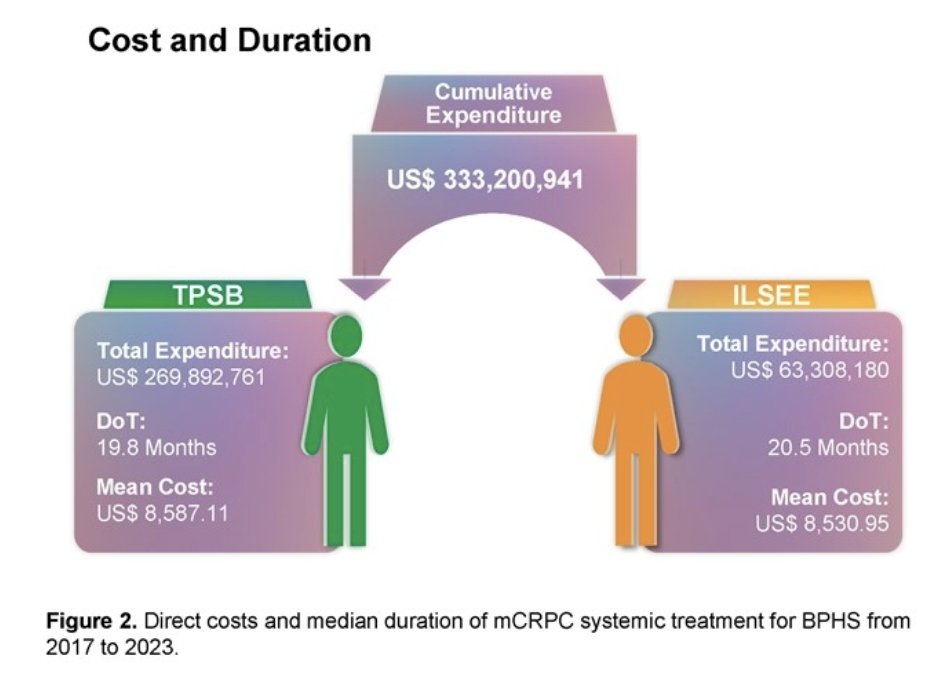
Interventions recognized for their survival benefits (TPSB) had a median duration of treatment (DoT) of 19.8 months, with a total expenditure of US$269,892,761 and an average cost per patient of US$8,587.11. In contrast, treatments lacking demonstrated survival benefit (ILSEE) were administered for a median DoT of 20.5 months, resulting in a total cost of US$63,308,180 and an average expense per patient of US$8,530.95. Despite similar treatment durations and per-patient costs, ILSEE therapies contributed substantially to total spending without proven efficacy in improving survival.
An exploratory financial analysis suggested that reallocating funds currently used for interventions without proven survival benefit could significantly improve access to evidence-based therapies. Specifically, the resources expended on a single patient receiving an ILSEE regimen could be redirected to provide generic cabazitaxel (20 mg/m² every 21 days) for up to two patients across six treatment cycles.
This model underscores how strategic redistribution of existing budgets could optimize patient outcomes in the Brazilian Public Health System, improving equity in access to life-prolonging treatments such as cabazitaxel while minimizing the use of low-value therapies.

Dr. Monteiro concluded their poster presentation with the following key points:
- This comprehensive analysis highlights real-world treatment patterns, duration, and financial burden associated with mCRPC management in Brazil’s public health system.
- A significant proportion of patients continue to receive treatments without proven survival benefit, underscoring inefficiencies in resource allocation.
- Findings call for research and policy reforms aimed at optimizing evidence-based therapy access and improving cost-effectiveness in mCRPC care within low- and middle-income countries.
Presented by: Fernando S. Monteiro, MD, at Hospital Sírio-Libanês: Brasília, Distrito Federal, Brasilia, Brazil
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025