(UroToday.com) The 2025 ESMO annual meeting featured a biomarker-based personalization in metastatic prostate cancer session and a presentation by Dr. Alice Bernard-Tessier discussing targeting androgen receptor alterations in prostate cancer.
Dr. Bernard-Tessier started her talk by emphasizing that androgen targeted therapies are the mainstay of prostate cancer, and that resistance to second generation androgen receptor pathway inhibitors is still driven by the androgen receptor. Alterations in androgen receptors are the most common alteration in advanced prostate cancer, and are the most enriched in mCRPC tumors: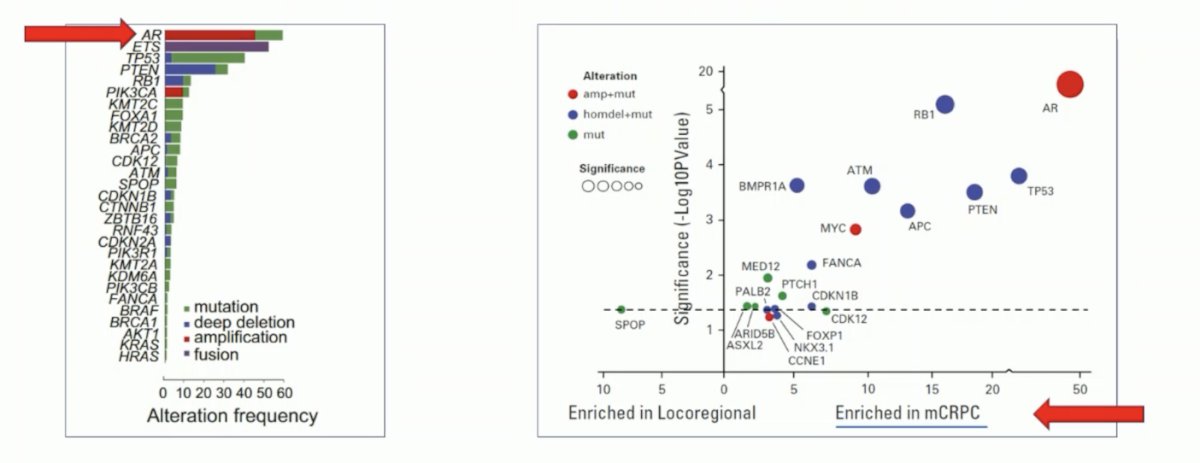
Androgen receptor alterations are prognostic in mCRPC, with androgen receptor amplification occurring in ~40-60% of alterations, and include either an androgen receptor upstream enhancer or copy number gain:

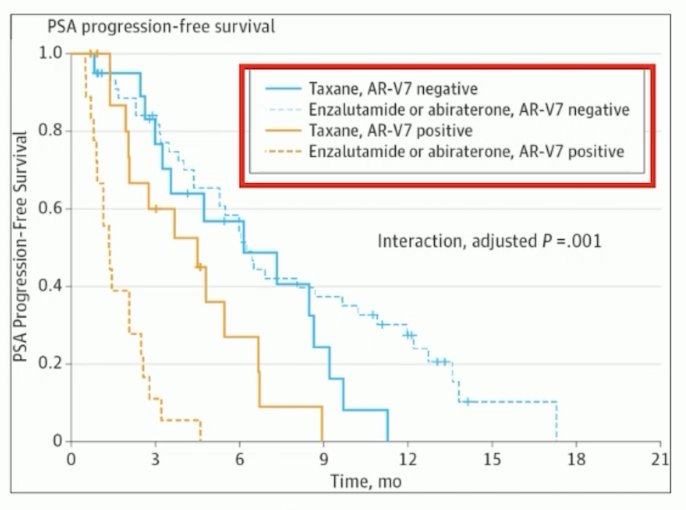
The second most common alteration is androgen receptor splicing variants, which make up ~15-55% of alterations. This includes both alternative splicing and gene structural rearrangements:
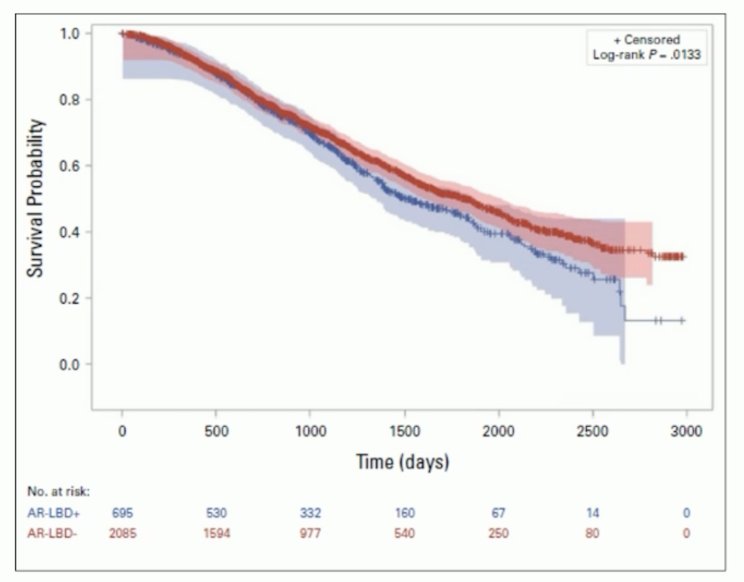
Finally, the androgen receptor mutations make up ~15-25% of alterations, which often occur in the ligand binding domain and are associated with worse prognosis:
Dr. Bernard-Tessier notes that over the last several years, we have elucidated specific androgen receptor targeting opportunities of these alterations. With regards to targeting splice variants, galeterone (an inhibitor of CYP17) was assessed in the ARMOR3-SV phase III trial, randomizing AR-V7 positive patients to enzalutamide versus galeterone:
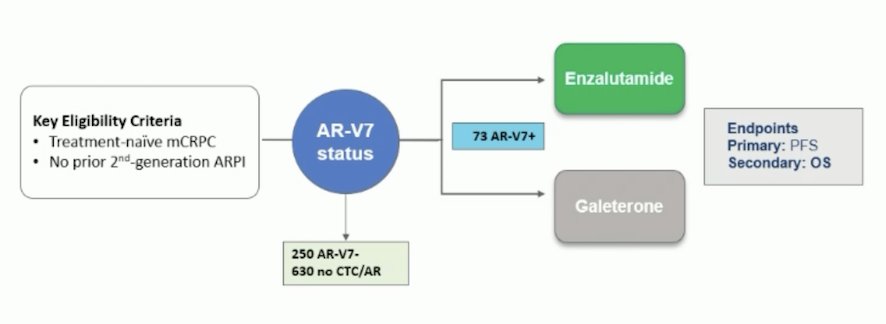
However, this study was closed early as it was deemed unlikely to meet its primary endpoint of improving progression free survival. A second agent, cirtuvivint (a pan CLK/DYRK inhibitor) was also assessed in combination with abiraterone, with modest PSA30 and PSA50 results and a RECIST best response of stable disease in 3/3 patients:

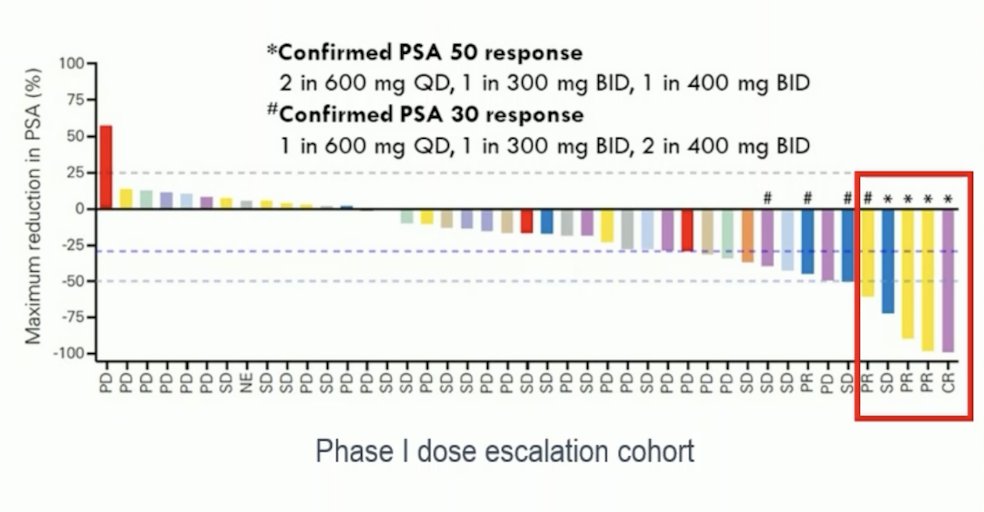
Presented at ASCO 2021 by Dr. de Bono, gumelutamide (TAS3681) is a third generation androgen receptor antagonist targeting the ligand binding domain, but this agent also had minimal activity based on PSA30 and PSA50 responses in a phase I dose escalation cohort:
Because of these results, attention was turned to targeting the N-terminal domain. Masofaniten (EPI-7386) is a small molecule targeting the N-terminal domain that was tested in the ONCT-534 randomized phase II study in combination with enzalutamide versus enzalutamide alone. This trial was ultimately terminated early secondary to a lack of efficacy given that masofaniten + enzalutamide had a PSA90 rate of 64% compared to 74% for enzalutamide alone.
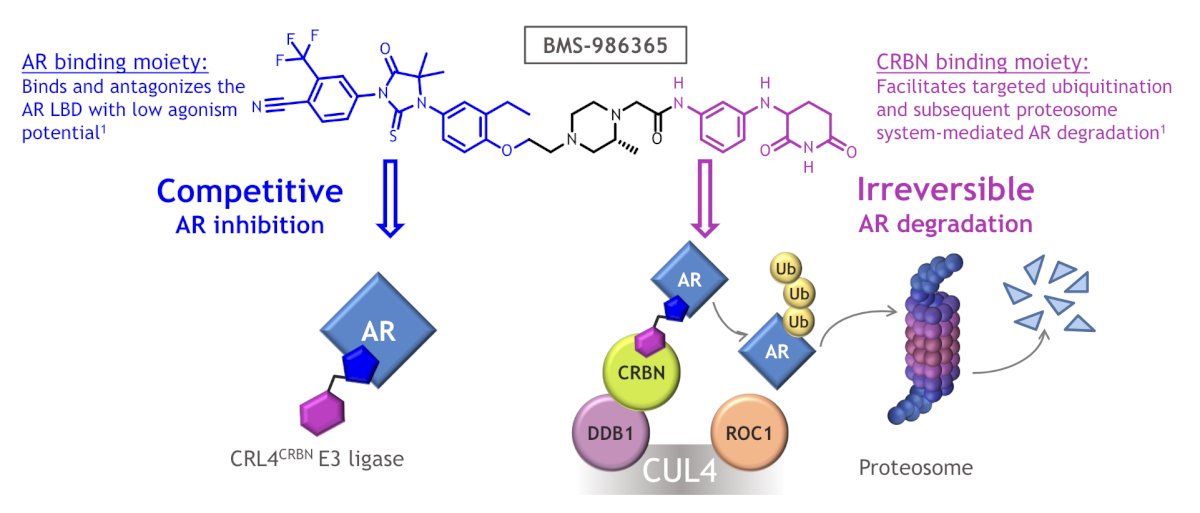
Dr. Bernard-Tessier then discussed BMS-986365, which is an androgen receptor degrader and antagonist. This agent is a heterobifunctional, oral therapy designed to inhibit androgen receptor activity via a first-in-class dual mechanism of androgen receptor degradation and antagonism:
In the CC-94676-PCA-001 trial,1 BMS-986365 was tested in mCRPC patients who progressed on antiandrogen therapy including ≥ 1 androgen receptor pathway inhibitor (ie. enzalutamide, abiraterone). Patients had prior taxane chemotherapy unless ineligible or declined. Part A included dose escalation (n = 27), and data reported are from the Part B dose expansion at 400, 600, or 900 mg BID (n = 20 each). The median follow-up was 14.8 months (range: 9.6-24.3), and the primary objectives were safety and tolerability, as well as the recommended phase 2 dose. Among the 68 patients, prior therapy included chemotherapy (n = 31; 46%), enzalutamide (n = 51; 75%), and abiraterone (n = 44; 65%). Overall, 46% received both enzalutamide and abiraterone:
![In the CC-94676-PCA-001 trial [1], BMS-986365 was tested in mCRPC patients who progressed on antiandrogen therapy including ≥ 1 androgen receptor pathway inhibitor (ie. enzalutamide, abiraterone). Patients had prior taxane chemotherapy unless ineligible or declined. Part A included dose escalation (n = 27), and data reported are from the Part B dose expansion at 400, 600, or 900 mg BID (n = 20 each). The median follow-up was 14.8 months (range: 9.6-24.3), and the primary objectives were safety and tolerability, as well as the recommended phase 2 dose. Among the 68 patients, prior therapy included chemotherapy (n = 31; 46%), enzalutamide (n = 51; 75%), and abiraterone (n = 44; 65%). Overall, 46% received both enzalutamide and abiraterone:](/images/com-doc-importer/232-esmo-2025/esmo-2025-targeting-androgen-receptor-alterations-in-prostate-cancer/image-8.jpg)
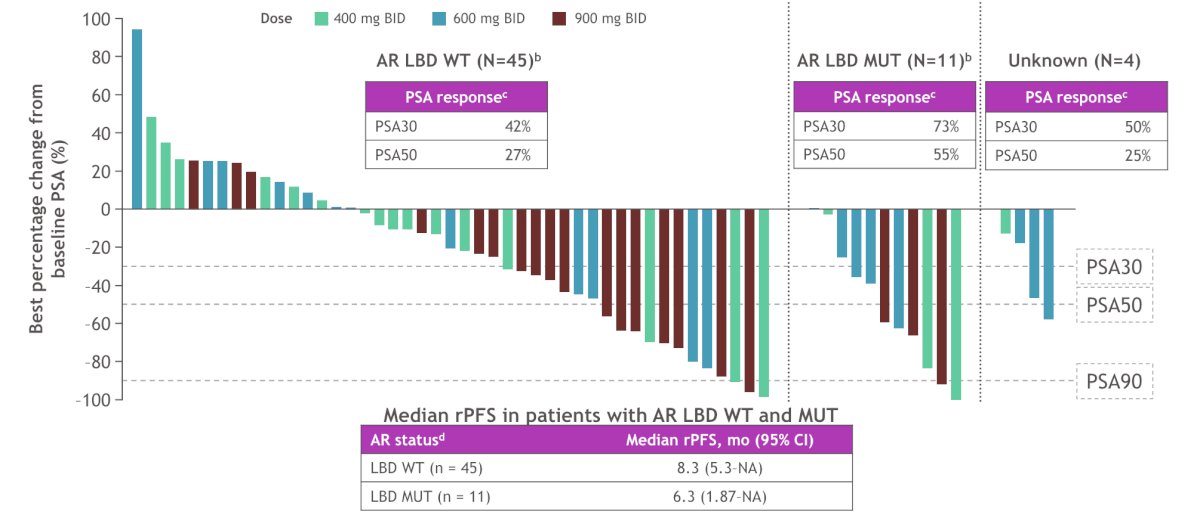
This study found that a clinical benefit of BMS-986365 was observed both in patients with androgen receptor ligand binding domain WT and mutant mCRPC:
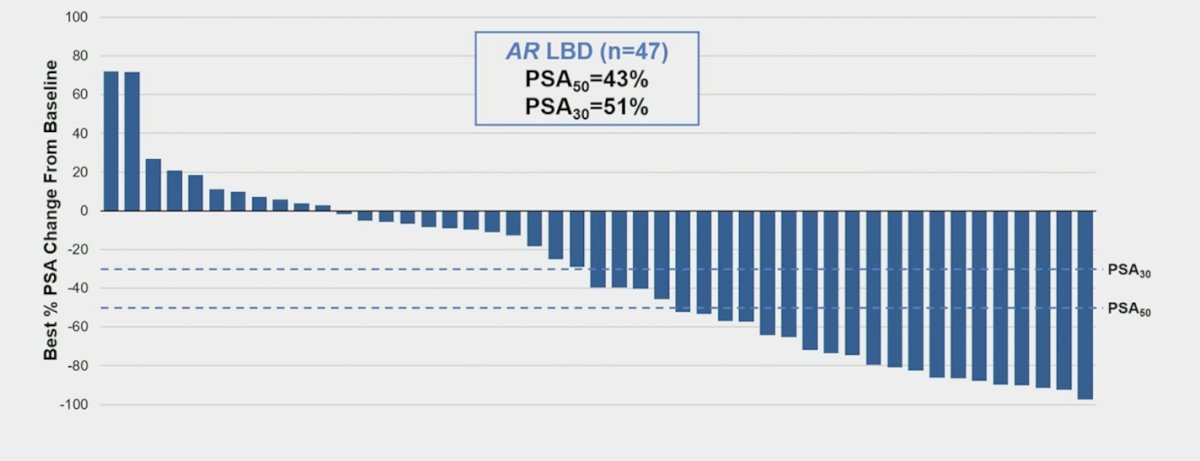
A second androgen receptor degrader has also been assessed, ARV-766/JSB462 (luxdegalutamide), with initial results presented by Dr. Petrylak at ASCO 2024. This agent is a novel, potent, orally administered PROTAC androgen receptor degrader that targets wild-type androgen receptor and clinically relevant androgen receptor ligand-binding domain mutants, including the most prevalent androgen receptor L702H, H875Y, and T878A mutations:
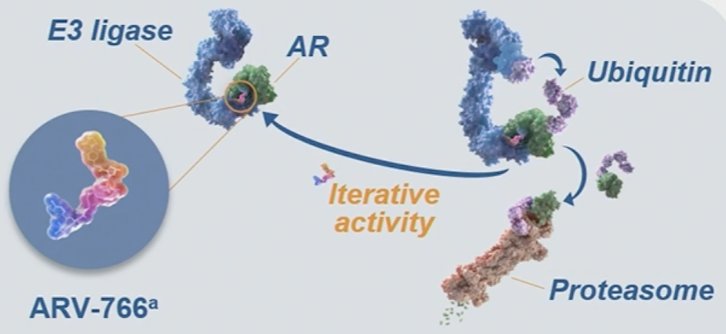
In the initial phase I/II study, eligible patients had progressive mCRPC and ongoing ADT. The phase 1 dose escalation portion evaluated the safety and tolerability of escalating doses of ARV-766 (20–500 mg once daily) in patients who had progressed on ≥2 prior systemic therapies (including ≥1 novel hormonal agents). The phase 2 cohort expansion portion is evaluating the clinical activity and safety of 2 doses of ARV-766 (100 or 300 mg once daily) in patients who had received 1–3 prior novel hormonal agents and ≤2 prior chemotherapy regimens. This study found that among patients with androgen receptor ligand-binding domain mutations, PSA50 was 43% and PSA30 was 51%:
Regarding targeting of androgen receptor activating mutations, Dr. Bernard-Tessier notes that the F877L mutation confers antagonist to agonist switch, and other mutations confer aberrant activation by other steroids including:
- AR L702H: corticosteroids
- AR T878A: progesterone
- AR H875Y: estradiol
Recent work from Dr. Bernard-Tessier’s group found that switching from prednisone to dexamethasone for patients receiving abiraterone led to an improvement in radiographic progression free survival:2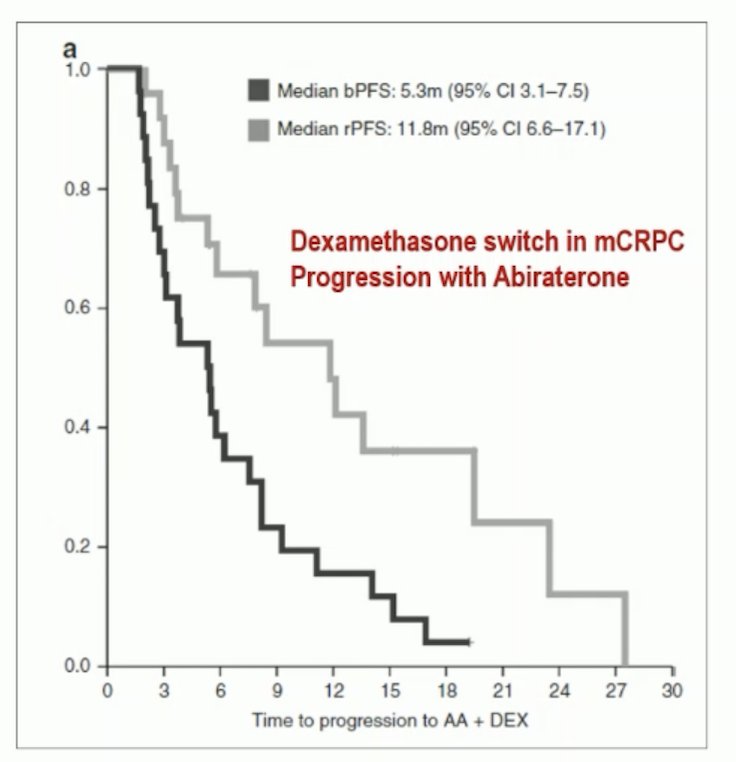
Opevesostat is a non-steroidal selective CYP11A1 inhibitor that was recently assessed in the phase II CYPIDES trial, initially presented at ESMO 2024. This was an open label, non-randomized trial. Patients received opevesostat 5 mg twice daily + supportive adrenal therapy (dexamethasone 1–1.5 mg and fludrocortisone 0.1 mg) along with ADT until disease progression. Eligible participants were mCRPC patients with disease progression following ≥1 novel hormonal agent and ≥1 taxane. A total of 134 patients were enrolled, of whom 66 had androgen receptor ligand binding mutations. Participants were recruited from clinical sites in France, Finland, the USA, and the UK. The median study follow-up was 7.1 months (data cut-off: January 23, 2024). Patients without androgen receptor ligand binding mutations were less likely to have received both abiraterone and enzalutamide and had lower median PSA values at baseline. These differences could reflect patient enrolment during different time periods and conditions favoring the development of androgen receptor ligand binding mutations:
In patients with androgen receptor ligand binding activating mutations, a PSA50 response was observed in 53% of patients:

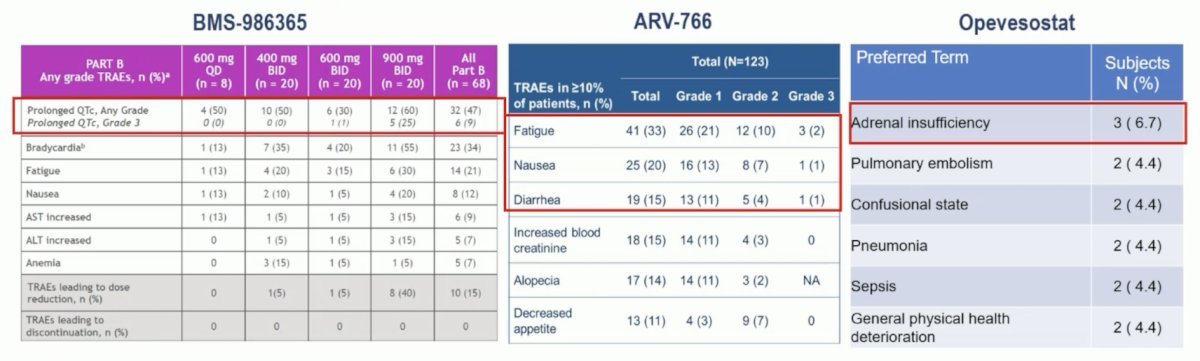
Notably, 37.8% of patients were treated for more than 6 months. Dr. Bernard-Tessier emphasized that safety is certainly a key consideration for these new treatments, raising concern for prolonged QT intervals, fatigue, diarrhea, and adrenal insufficiency:
To date, we do not yet have precision medicine, and many trials are ongoing in this disease space, including:
- OMAHA-3 in post-chemotherapy mCRPC
- OMAHA-4 in pre-chemotherapy mCRPC
- CA071-1000 in rechARge
- NCT07047118
Dr. Bernard-Tessier concluded her presentation discussing targeting androgen receptor alterations in prostate cancer with the following take home points:
- Androgen receptor alterations are still prognostic and not yet predictive
- New drugs targeting the androgen receptor and androgen receptor alterations are coming, including androgen receptor degraders, and CYP11A1 inhibitors
- Questions still remain as to who will benefit the most from 3rd generation androgen receptor pathway inhibitors
Presented by: Alice Bernard-Tessier, MD, Gustave Roussy, Villejuif, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
References:
- Rathkopf DE, Patel MR, Choudhury AD, et al. Safety and clinical activity of BMS-986365 (CC-94676), a dual androgen receptor ligand-directed degraded and antagonist, in heavily pretreated patients with metastatic castration-resistant prostate cancer. Ann Oncol. 2025 Jan;36(1):76-88.
- Bernard-Tessier A, Naoun N, Barraud S, et al. The future of androgen receptor targeting in prostate cancer: third-generation inhibitors and beyond. Ther Adv Med Oncol. 2025 Sep 29;17:17588359251379416.