(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st, 2025 was host to a presidential symposium. Dr. Arun Azad discussed PSMAddition, a phase III trial of [177Lu]Lu-PSMA-617 combined with androgen deprivation therapy (ADT) plus an androgen receptor pathway inhibitor (ARPI) in patients with PSMA-positive metastatic hormone-sensitive prostate cancer (mHSPC), presented earlier by Dr. Scott Tagawa.
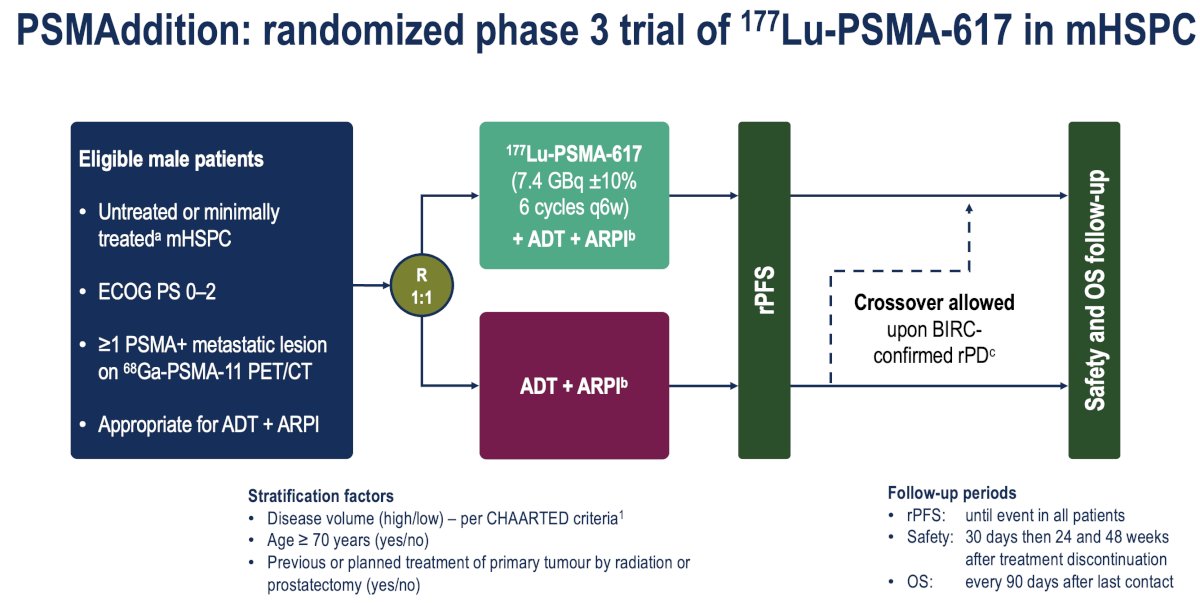
PSMAddition is the first phase III study of targeted radioligand therapy in mHSPC patients. This trial randomized men with untreated or minimally treated mHPSC and ≥1 PSMA-positive metastatic lesion on 68Ga-PSMA-11 PET/CT to:
- Experimental arm: 177Lu-PSMA 617 (7.4 GBq ±10% 6 cycles q6w) + ADT + ARPI
- Control arm: ADT + ARPI
- Crossover to the 177Lu-PSMA 617 arm was permitted upon radiographic progression
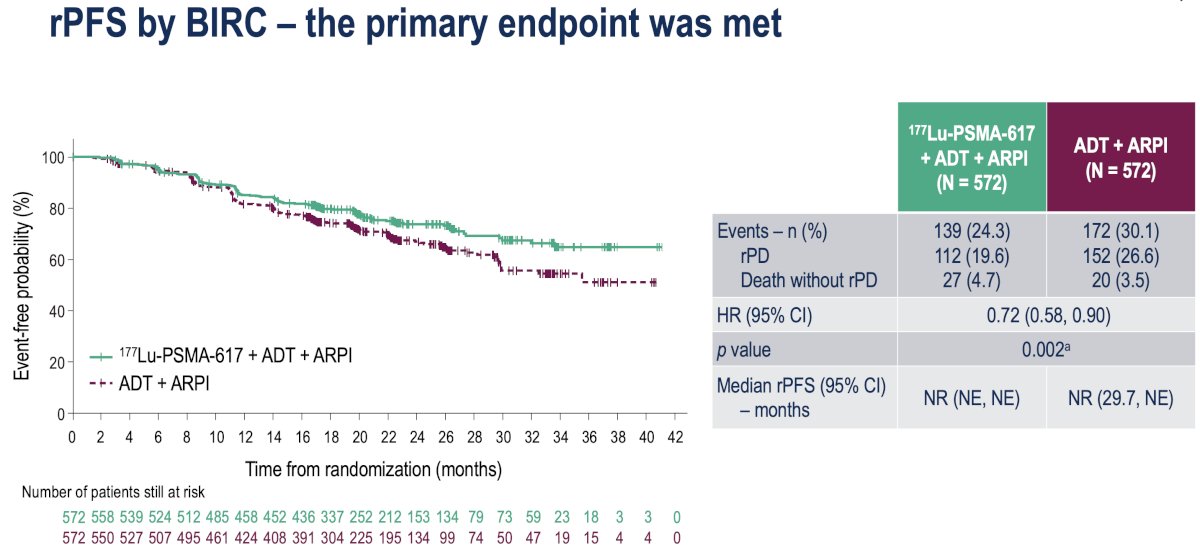
The study met its primary endpoint with radiographic progression-free survival (rPFS) significantly prolonged with the addition of 177Lu-PSMA-617 (HR: 0.72, 95% CI: 0.58-0.90, p=0.002). Median rPFS has not been reached in either arm yet.
Overall survival analysis to date demonstrates a non-significant trend towards an OS benefit in the intervention arm (HR: 0.84, 95% CI: 0.64-1.13, p=0.125):
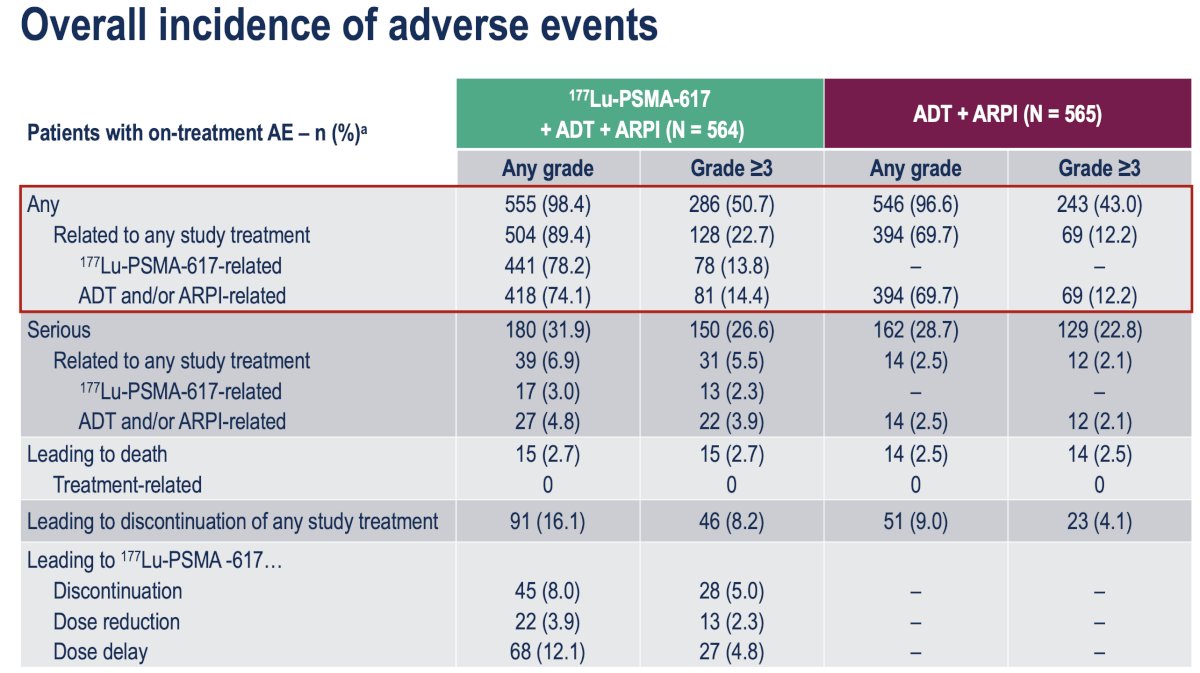
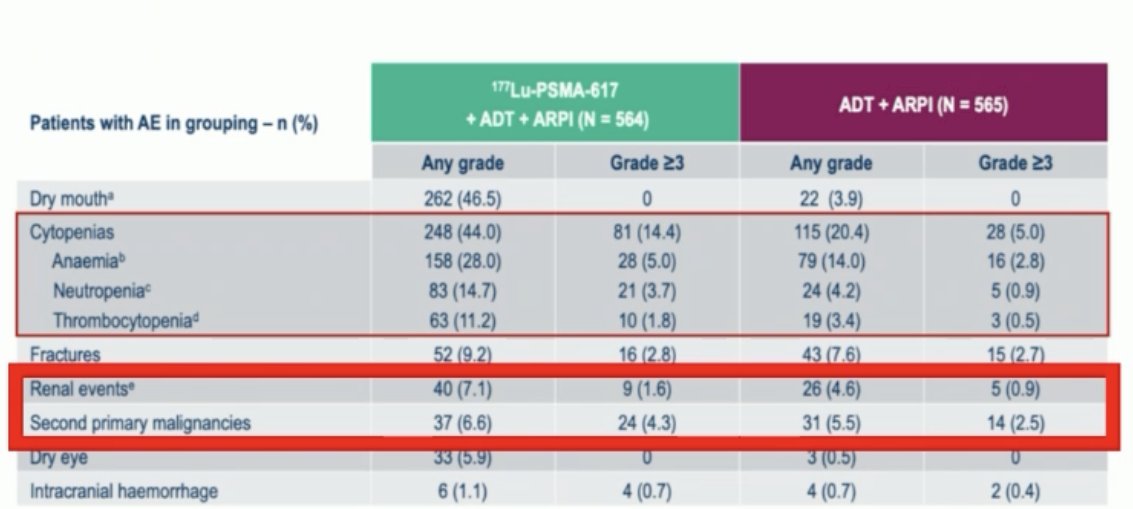
Patients in the Lu-PSMA arm had an increased incidence of adverse events:
- Any grade: 98.4% vs 96.6%
- Grade ≥3: 51% vs 43%
- Any grade dry mouth and GI toxicity
- Secondary primary malignancies and renal events
Key strengths of PSMAddition were as follows:
- Large, randomized phase III trial
- Included an active control arm of ADT + ARPI
- Met its primary endpoint (albeit lower magnitude of effect [i.e., HR] than expected)
- Will early use of Lu-PSMA-617 in mHSPC improve OS?
- Should/can we optimize patient selection for Lu-PSMA-617?
- Do all patients need 6 cycles of Lu-PSMA-617?
- How will toxicity from early use of Lu-PSMA-617 impact patients?
- 60% of the control arm with radiographic progression have already crossed over and this may dilute any OS benefit
- Lu-PSMA retains activity in later lines
Should we optimize patient selection for Lu-PSMA? In the PSMAddition trial, all clinically relevant subgroups derived an rPFS benefit from Lu-PSMA-617. Notably, 87% of screened patients were eligible based on the PSMA PET selection criteria. In effect, this ‘one size fits all’ strategy worked as it led to a positive trial results; however, can we do better?
Dr. Azad argued that biomarkers are key, particularly as we are in an era of personalized medicine for mHSPC, with key trials such as CAPItello-281 and AMPLITUDE2 evaluating capivasertib and niraparib in PTEN-deficient and BRCA/HRR-mutated populations, respectively. Although Lu-PSMA-617 was used in a very broad population in PSMAddition, it is a targeted radiopharmaceutical, and we need to harness PSMA better as a predictive biomarker.
Prior studies have identified PSMA PET biomarkers that are predictive of a greater benefit with Lu-PSMA-617 therapy, including PSMA SUVmean (TheraP, VISION)3,4 and PSMA total tumor volume (Enza-P)5. Increased PSMA uptake in tumors is associated with improved radiation absorption and increased tumor cell death.
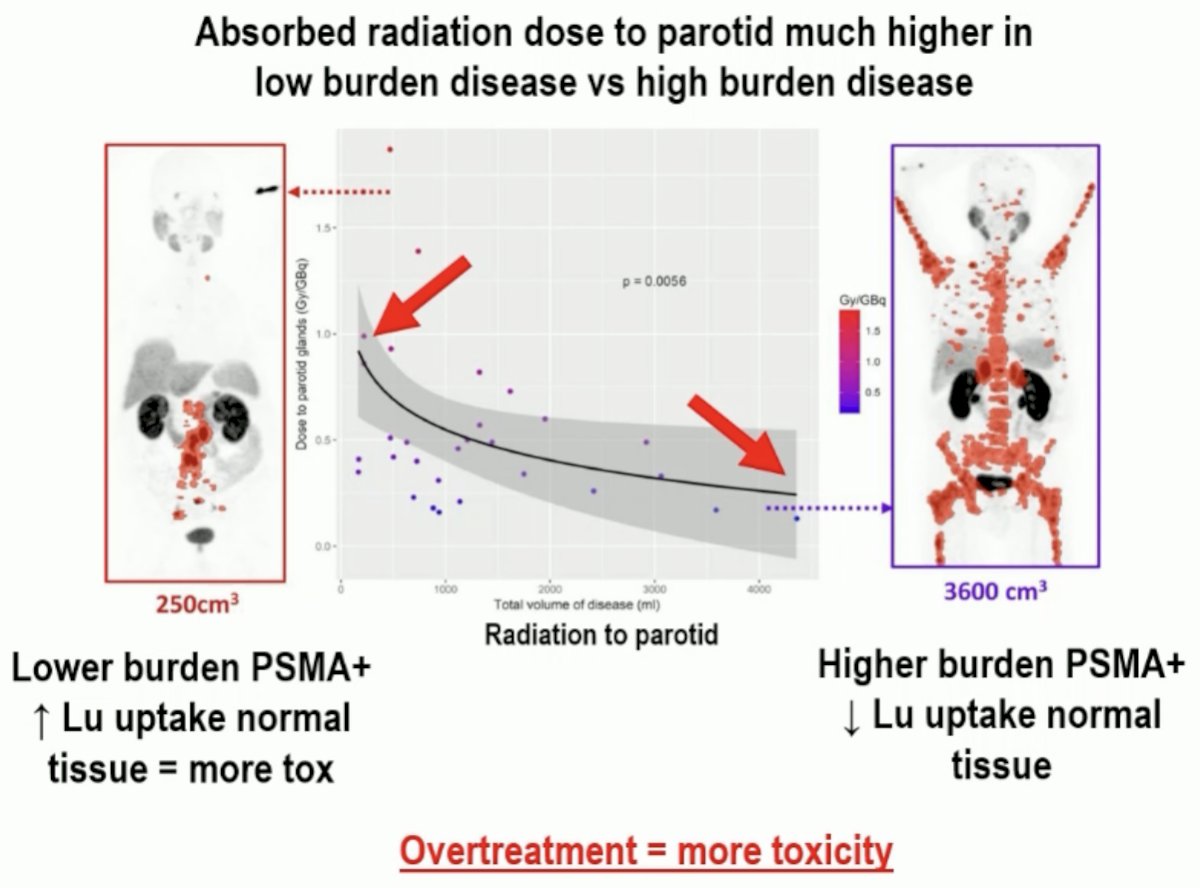
Do all patients need the full 6 cycles of Lu-PSMA-617? A key principle of theranostics is: ‘We see what we treat, and we treat what we see’. In other words, if there is no visible disease, then there is nothing to treat. In the UpFrontPSMA trial of patients with de novo, high volume disease, impressive responses were seen with only two cycles of Lu-PSMA-617.6 In the PSMAddition study population of patients that included those with lower volume disease, it is even more likely that 6 cycles of Lu-PSMA-617 represented overtreatment for a significant proportion.

One issue to keep in mind is the ‘sink effect’, whereby giving Lu-PSMA-617 to a patient with minimal or no residual PSMA-positive disease is potentially harmful, as normal tissues will be exposed to a higher dose of radiation. One potential solution to this issue is to perform a PSMA PET scan after 2-4 cycles to identify complete metabolic responders who will not benefit from further Lu-PSMA-617, imaged with either SPECT or PET.
How will toxicity from the early use of Lu-PSMA-617 impact patients? Patients receiving Lu-PSMA-617 in the PSMAddition trial had higher:
- Any grade and grade ≥3 hematologic toxicities
- Any grade dry mouth and GI toxicity

Dr. Azad noted that we must be mindful of two important late toxicities with Lu-PSMA-617:
- Secondary myeloid neoplasms, particularly acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS) – occur in 1.3% of mCRPC patients receiving Lu-PSMA7
- Renal impairment (Lu is renally excreted)
Dr. Azad concluded the discussant session of the PSMAddition trial with his own take home messages:
- PSMAddition is the 1st randomized, phase III trial demonstrating the efficacy of Lu-PSMA-617 in mHSPC
- rPFS benefit probably will lead to regulatory approval; however, to date, there is no improvement in OS and lower QoL with Lu-PSMA-617
- The goal of any anti-cancer treatment is to make patients live longer and live better
- This goal has not been achieved in PSMAddition
- He would not recommend widespread use of Lu-PSMA-617 in mHSPC at this stage
- He would consider using it if there is evidence of "bad" disease (e.g. de novo, high volume) or "bad" scans (e.g. very high PSMA SUVmean and/or total tumour volume)
- He expressed concerns regarding patient selection, overtreatment and impact of toxicity
- Lu-PSMA-617 remains an active and approved agent for mCRPC
- But to deliver the best outcomes in mHSPC, it will take a patient-centered approach focused on identifying predictive biomarkers, avoiding overtreatment, and minimizing (late) toxicities
Presented by: Arun Azad, PhD, MBBS, FRACP, Professor, Department of Medicine, Peter MacCallum Cancer Centre, Melbourne, Victoria, Australia
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: Interim PSMAddition Analysis Shows Lutetium PSMA-617 Improves rPFS in mHSPC - Scott Tagawa
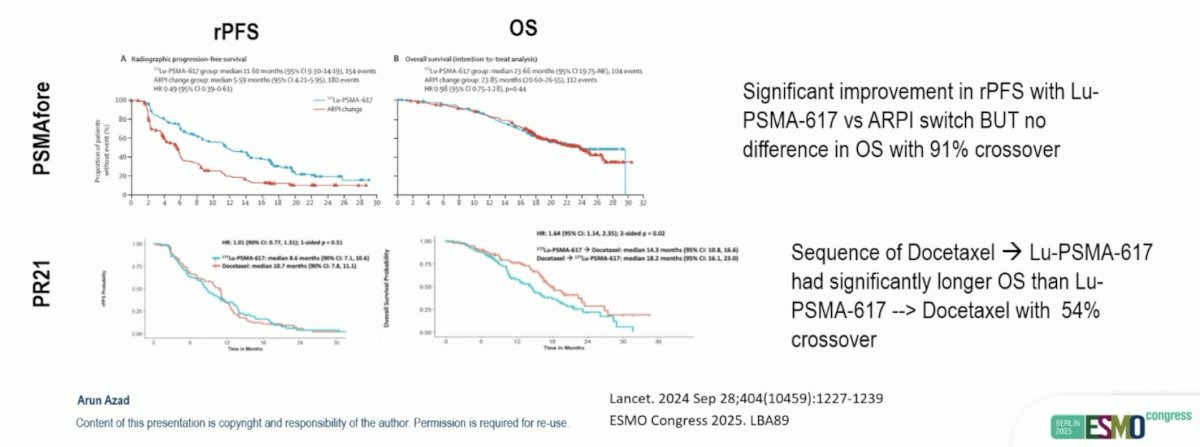
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial. Lancet. 2024;404(10358):1–11.
- Attard G, Agarwal N, Graff JN, et al. Phase 3 AMPLITUDE trial: Niraparib (NIRA) and abiraterone acetate plus prednisone (AAP) for metastatic castration-sensitive prostate cancer (mCSPC) patients (pts) with alterations in homologous recombination repair (HRR) genes. J Clin Oncol. 2025;43(17_suppl):LBA5006.
- Buteau JP, Martin AJ, Emmett L, et al. PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): a biomarker analysis from a randomised, open-label, phase 2 trial. Lancet Oncol. 2022;23(11):1389–1397.
- Kuo PH, Morris MJ, Hesterman J, et al. Quantitative ^68Ga-PSMA-11 PET and clinical outcomes in metastatic castration-resistant prostate cancer following ^177Lu-PSMA-617 (VISION trial). Radiology. 2024;312(2):e233460.
- Emmett L, Papa N, Subramaniam S, et al. Prognostic and predictive value of baseline PSMA-PET total tumour volume and SUVmean in metastatic castration-resistant prostate cancer in ENZA-p (ANZUP1901): a substudy from a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2025;26(9):1168–1177.
- Azad AA, Sweeney CJ, Armstrong AJ, et al. Sequential [177Lu]Lu-PSMA-617 and docetaxel versus docetaxel in patients with metastatic hormone-sensitive prostate cancer (UpFrontPSMA): a multicentre, open-label, randomised, phase 2 study. Lancet Oncol. 2024;25(10):1345–1356.
- Truillet C, Brenot-Rossi I, Lavigne C, et al. Therapy-related myeloid neoplasms after [177Lu]Lu-PSMA-617 therapy in patients with metastatic castration-resistant prostate cancer: incidence, risk factors, and outcomes. J Nucl Med. 2025;66(4):579–584.