(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress was host to a prostate, penile, and testicular cancers proffered paper session. Dr. Nicholas James discussed ENZARAD (ANZUP 1303), a randomized phase II trial of ADT + radiation therapy +/- enzalutamide for high-risk, clinically localized prostate cancer, presented earlier by Dr. Paul Nguyen.
It has long been established that adding local radiotherapy to continuous androgen suppression improves overall survival in high-risk or locally advanced prostate cancer, compared to systemic therapy alone, with the SPCG-7 and NCIC/MRC trials demonstrating 12% and 11% overall survival benefits at 10 and 7 years, respectively.1,2

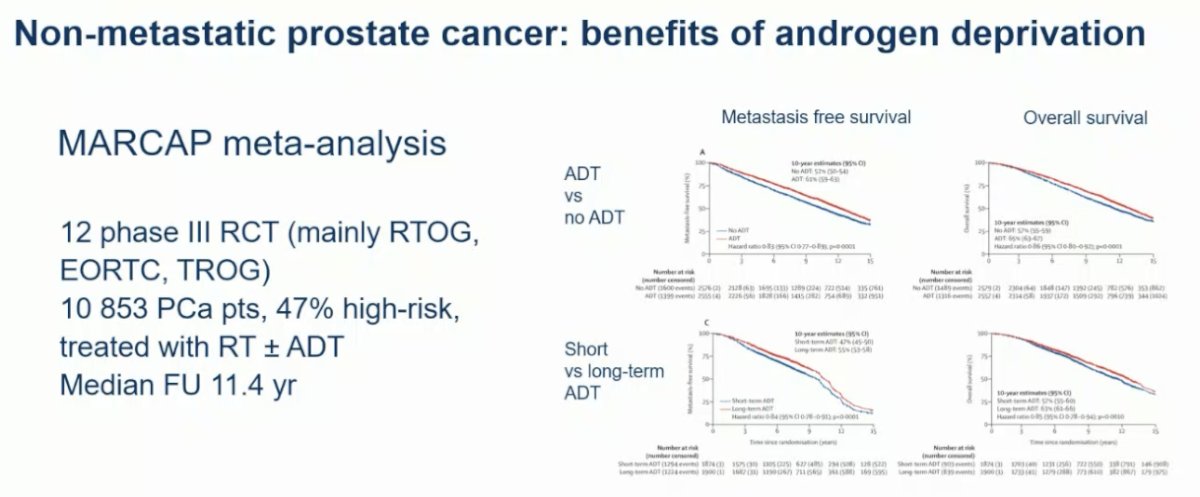
Additionally, it has been shown that treatment intensification with ADT (versus no ADT) and the use of long-term ADT (versus short-term ADT) improves metastasis-free and overall survivals in localized or locally advanced prostate cancer treated with radiotherapy.
However, Dr. James noted that more does not always mean better. Lower-grade and stage prostate cancer have excellent prognoses, and more androgen deprivation can be toxic, with worse death rates from non-cancer causes.
While most trials of treatment intensification have been in the metastatic setting, the STAMPEDE M0 trial has demonstrated a survival benefit to the addition of abiraterone to radiotherapy + ADT in high/very high-risk prostate cancer patients.4
How do the ENZARAD and STAMPEDE M0 patient cohorts compare? Firstly, the sample size in STAMPEDE M0 was significantly larger (n=1974 versus 802). Patients in the ENZARAD trial had:
- Lower median serum PSA levels (only 35% with PSA>20 ng/ml versus median PSA of 32 ng/ml in STAMPEDE M0)
- Lower stage disease (cT3-4: 47% vs 94%)
- Less clinical nodal involvement (12% vs 35%)
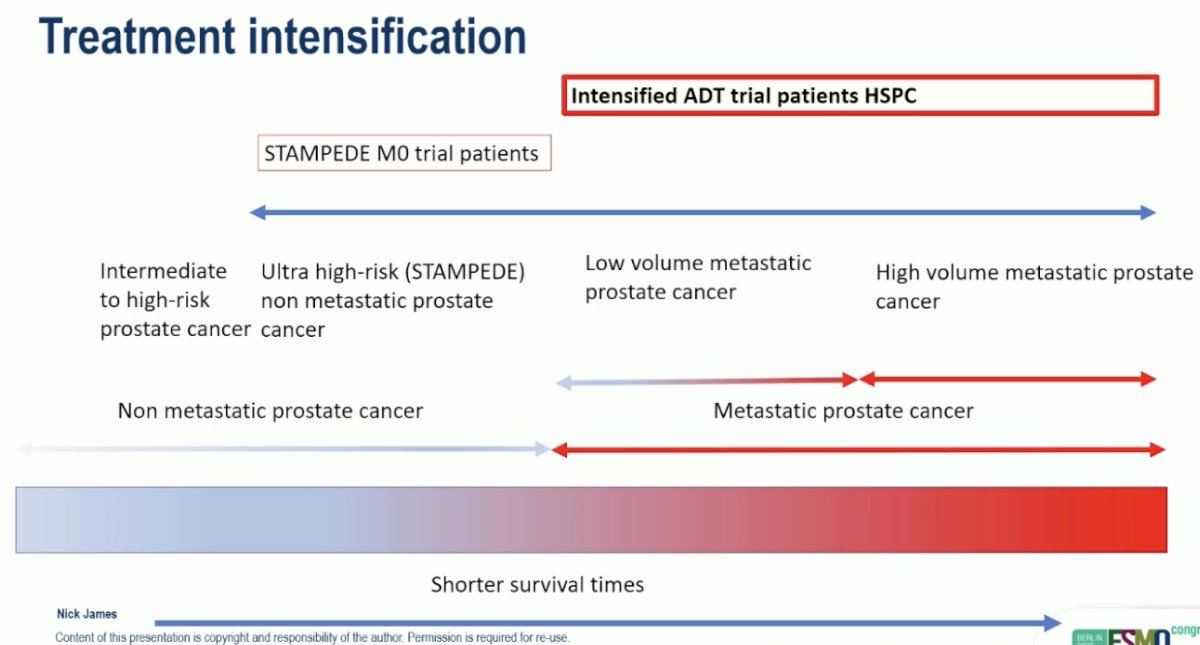
Overall, Dr. James argued that the ‘upper ends’ of risk groups were probably similar between the trials; however, ENZARAD extends into lower risk groups, compared to STAMPEDE M0, and it is a smaller trial with more limited power for subgroup analyses.

As such, Dr. James argued that this is where ENZARAD ‘sits’ in comparison to STAMPEDE along the disease risk continuum:

The ENZARAD study design is illustrated below. Men with high-risk, localized prostate cancer suitable for external beam radiotherapy (EBRT) were randomized to:
- Experimental arm: Enzalutamide (160 mg daily x 24 months) + LHRH agonist (24 months) + prostate EBRT +/- brachytherapy +/- nodal irradiation 16 weeks after starting hormonal therapy
- Control arm: Conventional NSAA (6 months) + LHRH agonist (24 months) + prostate EBRT +/- brachytherapy +/- nodal irradiation 16 weeks after starting hormonal therapy
The primary endpoint was metastasis-free survival (MFS), with a sample size of 800 patients having 80% power to detect a hazard ratio (HR) benefit of 0.67. The secondary endpoints were:
- Overall survival (OS)
- Of note, OS was the original primary endpoint, but this was changed to MFS due to lower rates of deaths observed than anticipated
- Cause-specific survival (CSS)
- PSA progression-free survival (PSA PFS)
- Clinical progression-free survival
- Castration resistance
- Health-related quality of life (HRQoL)
- Adverse events

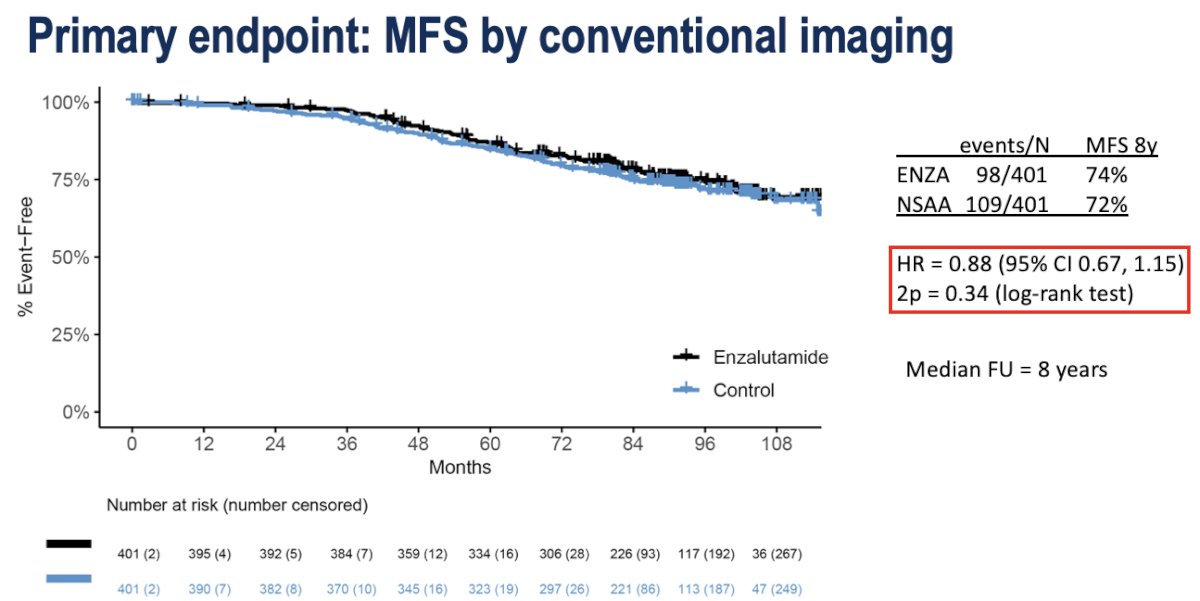
The study failed to meet its primary endpoint of an MFS benefit (8-year: 74% versus 72%; HR: 0.88, 95% CI: 0.67–1.15, p=0.34).
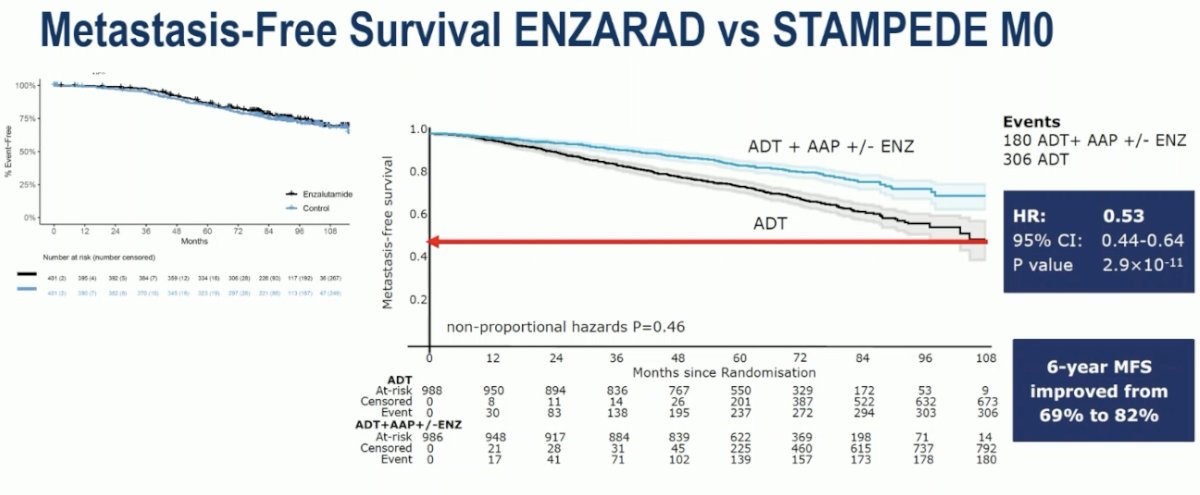
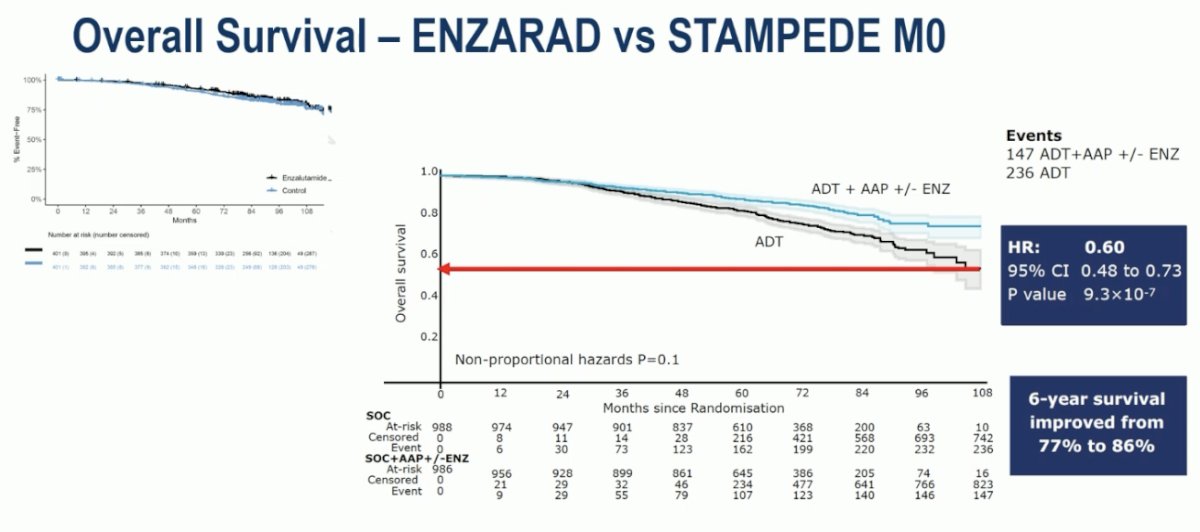
The differences between the study populations of ENZARAD and STAMPEDE M0 are clearly reflected in the MFS Kaplan-Meier curves. While the 10-year MFS was ~70% in the ENZARAD trial, it was close to 50% at 10 years in the STAMPEDE M0 control arm, highlighting the higher risk nature of the STAMPEDE M0 cohort.
Similar to MFS, no significant difference in OS was observed with enzalutamide in the ENZARAD trial (8-year: 83% versus 80%; HR: 0.87, 95% CI: 0.63–1.20, p=0.40).

Similarly, the 10-year OS in the ENZARAD trial significantly outperformed that observed in the STAMPEDE M0 control arm (~75% vs 50%), again reflecting the contrasting risk profiles of the two study populations.
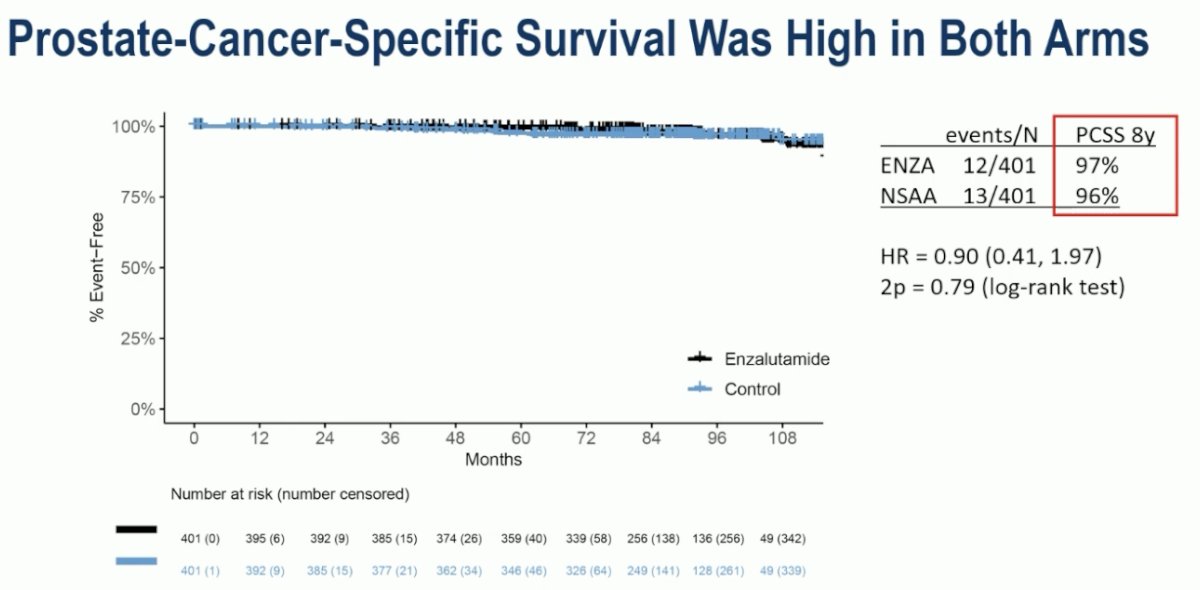
Prostate cancer-specific survival was high in both arms, with 8-year rates of 97% and 96% in the experimental and control arms, respectively, highlighting that enzalutamide likely represents overtreatment in this population of patients with a relatively good prognosis.
How do we explain the differences between the results of the ENZARAD and STAMPEDE M0 trials?
- Random variation – no underlying differences
- Difference in case mix
- Different efficacies for abiraterone and enzalutamide
- Different efficacies for ARPIs in different risk groups
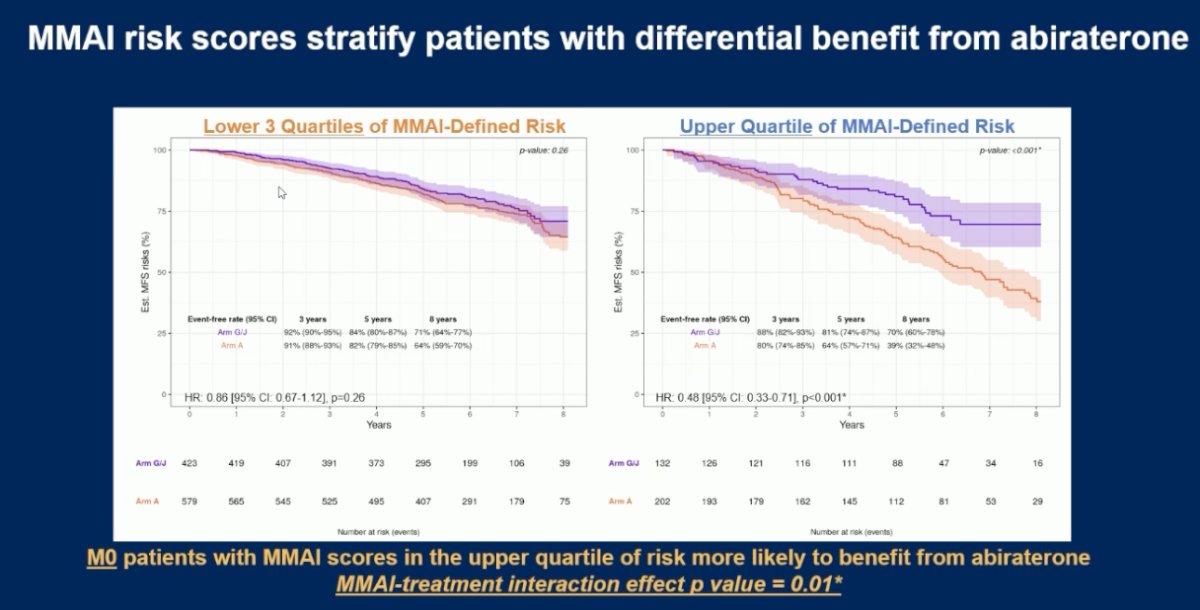
Dr. James noted that support for this last point, different efficacies for ARPIs in different risk groups, comes from his group’s work presented at ASCO 2025. This was a substudy embedded within the STAMPEDE platform, designed to evaluate the feasibility of digital pathology AI-guided treatment selection for high-risk localized prostate cancer. The objective was to explore whether a prognostic AI-derived pathology score could identify a subgroup of clinically high-risk patients more likely to benefit from the addition of abiraterone to standard of care therapy.
They demonstrated that the MMAI score is prognostic even within clinically high-risk prostate cancer populations. Applying established clinical prognostic cut-offs, 89% (N=1,189) of M0 patients in the cohort were classified as MMAI high-risk, demonstrating the model's ability to further stratify risk within an already high-risk population. Importantly, M0 patients with MMAI scores in the upper quartile of risk were significantly more likely to benefit from the addition of abiraterone, with an MFS HR of 0.48 (95% CI: 0.33–0.71; p < 0.001). Notably, the interaction between MMAI risk score and treatment effect was statistically significant (interaction p = 0.01), supporting the potential role of MMAI as a predictive biomarker to guide selective treatment intensification with abiraterone in high-risk prostate cancer.5
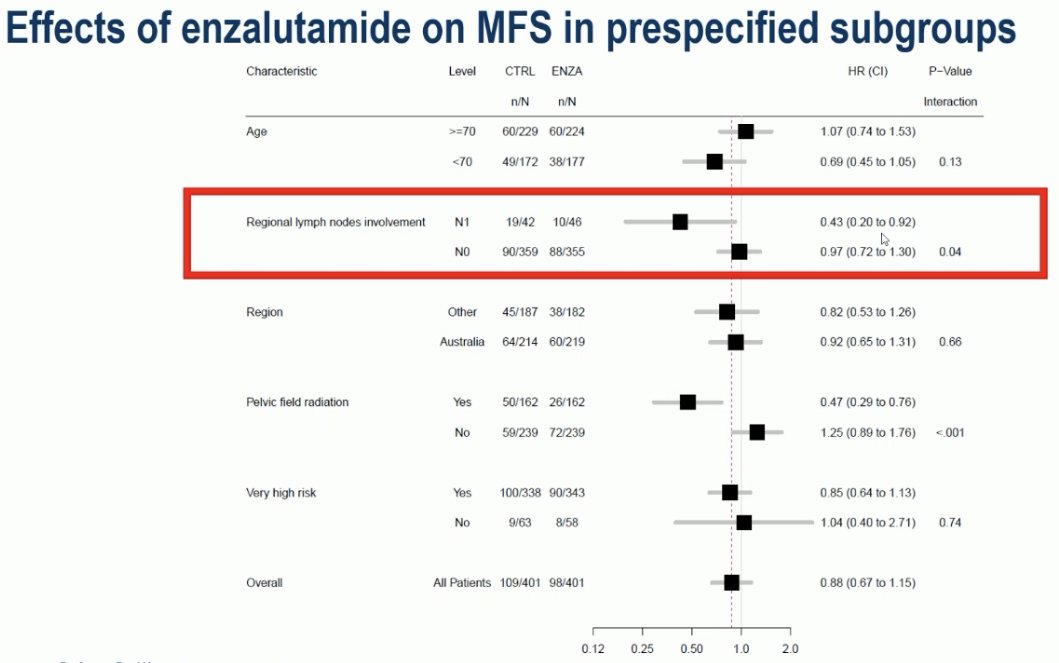
Can we identify a subgroup within ENZARAD that may benefit from enzalutamide intensification? Yes, it appears that patient cN1 disease derive a significant benefit from the addition of enzalutamide to ADT + radiotherapy.
Dr. James concluded as follows:
- Although a ‘negative’ trial, the differences between ENZARAD and STAMPEDE can be explained by:
- Case mix: Not enough events to detect an effect
- Differential ARPI effects with tumor biology
- Possibly, but less likely, related to differential ARPI efficacy for enzalutamide versus abiraterone
- Individual patient data meta-analyses will be valuable in separating these hypotheses
- Assessment with additional translational methods will also be valuable
- Data from ATLAS (with apalutamide) and DASL-HiCaP (with darolutamide) are pending
- Adjuvant ARPI is probably not of significant value outside of STAMPEDE high-risk M0
Presented by: Nicholas James, MBBS, PhD, Professor of Prostate and Bladder Cancer Research at The Institute of Cancer Research and The Royal Marsden NHS Foundation Trust, London, UK
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: The Phase III ENZARAD Trial: Enzalutamide with Radiation and ADT in High-Risk Prostate Cancer - Paul Nguyen
References:
- Widmark A, Klepp O, Solberg A, et al. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): an open, randomised phase III trial. Lancet. 2009; 373(9660):301–308.
- Mason MD, Parulekar WR, Sydes MR, et al. Combined androgen deprivation therapy and radiation therapy for locally advanced prostate cancer: a randomised, phase 3 trial. Lancet. 2015; 386(9998):52–60.
- Kishan AU, King CR, Spratt DE, et al. Androgen deprivation therapy use and duration with definitive radiotherapy for localized prostate cancer: an individual patient data meta-analysis of the MARCAP consortium. Lancet Oncol. 2022; 23(2):267–279.
- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomized controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022; 399(10323):447-460.
- Parker CTA, Liu VYT, Mendes L, et al. Multimodal artificial intelligence (MMAI) model to identify benefit from 2nd-generation androgen receptor pathway inhibitors (ARPI) in high-risk non-metastatic prostate cancer patients from STAMPEDE. J Clin Oncol. 2025; 43(16_suppl):5001 (abstract).