(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress was host to a prostate, penile, and testicular cancers proffered paper session. Derya Tilki, MD, discussed the overall survival (OS) results from EMBARK, a randomized phase III trial of enzalutamide or placebo plus leuprolide acetate and enzalutamide monotherapy in high-risk biochemically recurrent prostate cancer, and the final results from PRESTO, a phase III trial of combined androgen blockade in patients with high-risk biochemically relapsed prostate cancer.
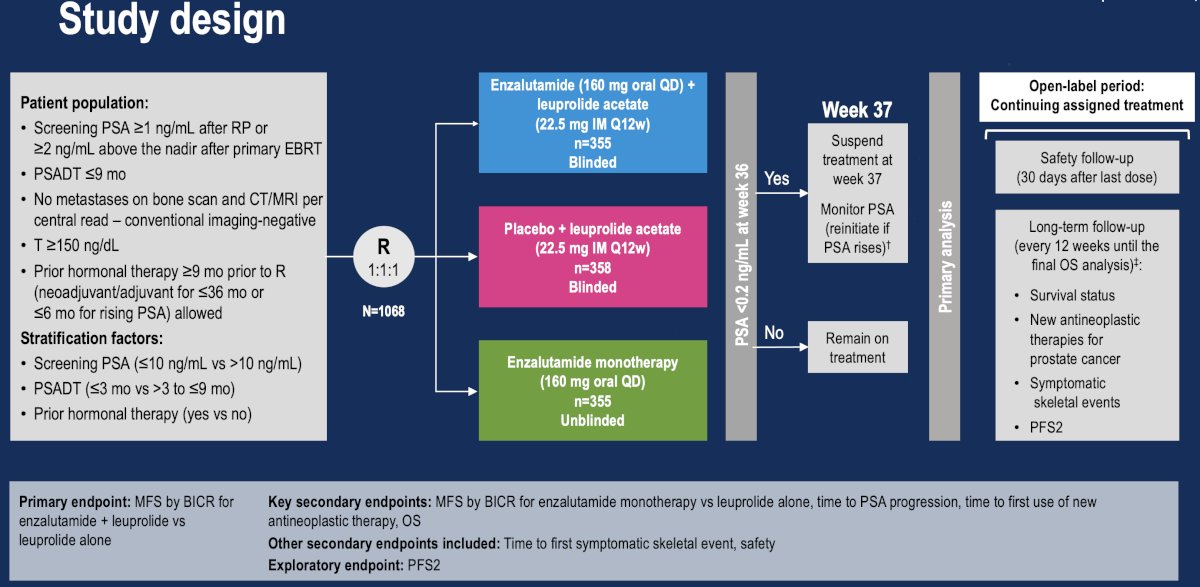
EMBARK is a phase III trial that included patients with a PSA ≥1 ng/ml after radical prostatectomy or ≥2 ng/ml above nadir after primary external beam radiotherapy (EBRT), with a PSA doubling time (PSADT) of ≤9 months. Patients had no evidence of metastasis on conventional imaging, and baseline testosterone was ≥150 ng/dL. Hormone therapy ≥9 months prior to enrolment was permitted. Patients underwent stratified randomization to one of three arms:
- Enzalutamide 160 mg (standard dose) + leuprolide acetate (blinded arm)
- Placebo + leuprolide acetate (blinded)
- Enzalutamide monotherapy (unblinded)
PSA was assessed at 36 weeks, and if patients had:
- PSA<0.2 Treatment was suspended at week 37, and PSA was monitored with treatment reinitiated if PSA rose again
- PSA>0.2 Treatment was continued
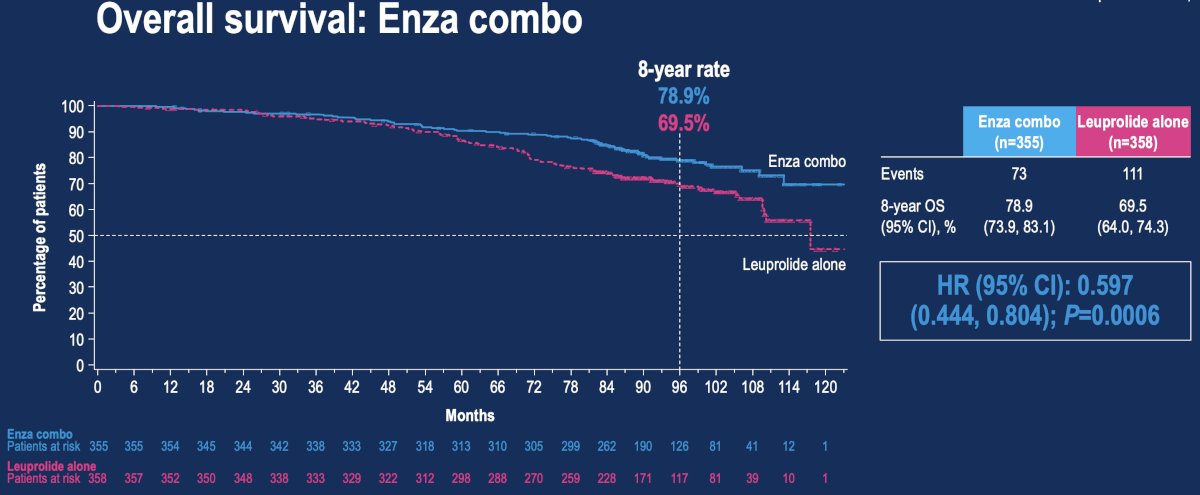
The final OS analysis demonstrated that enzalutamide combination therapy was associated with a 40.3% lower rate of overall deaths, compared with leuprolide alone (8-year OS: 79% versus 69.5%; HR: 0.60, 95% CI: 0.44–0.80, p=0.0006):
In the comparison of enzalutamide monotherapy to leuprolide alone, the risk of death was 17% lower with enzalutamide monotherapy; however, this did not reach statistical significance (HR: 0.83, 95% CI: 0.63–1.10, p=0.19).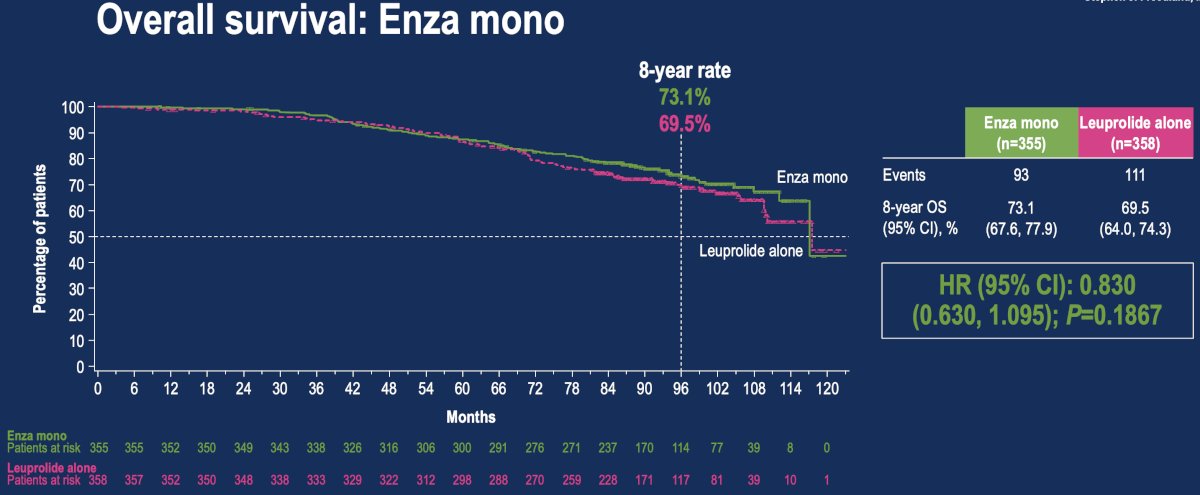
PRESTO is a randomized phase III, open-label trial in patients with biochemically relapsed prostate cancer and PSA doubling time ≤ 9 months, without distant metastases on conventional imaging (NCT03009981). Patients were randomized 1:1:1 to receive a finite 52-week treatment course with ADT, ADT + apalutamide, or ADT + apalutamide + abiraterone acetate plus prednisone, stratified by PSA doubling time (< 3 vs 3–9 months).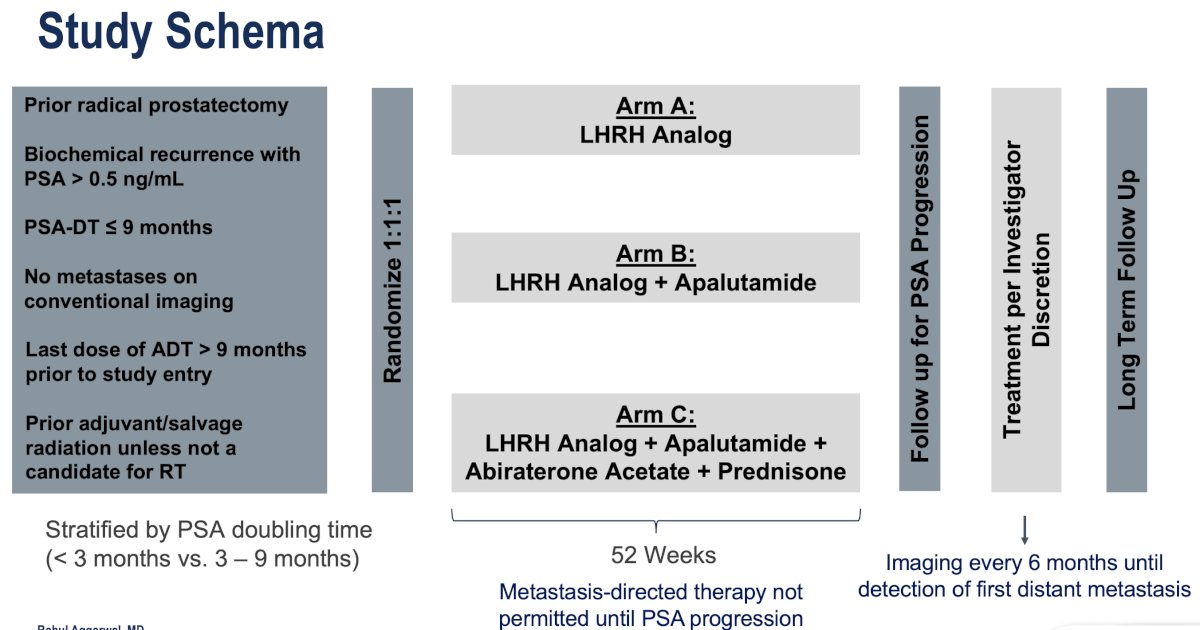
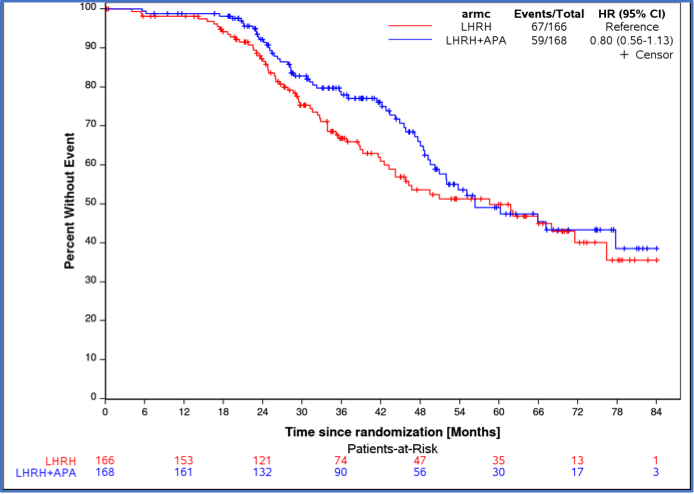
For the outcome of metastasis-free survival:
- ADT + apalutamide vs. ADT: HR=0.80, 95% CI: 0.56–1.13
- Difference in restricted mean survival over the first 48 months between ADT + apalutamide vs. ADT was 2.92 months (95% CI: 0.45–5.39)
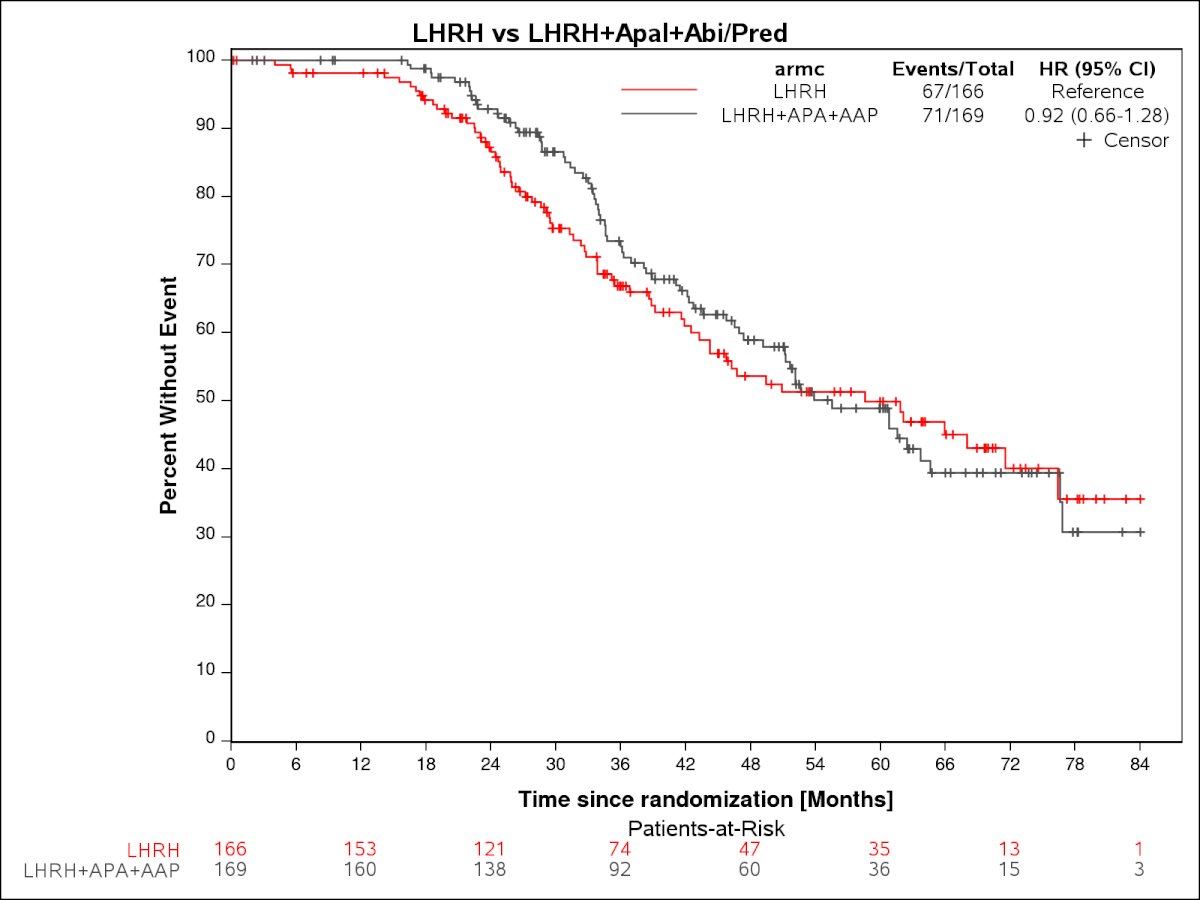
- ADT + apalutamide + abiraterone vs. ADT: HR=0.92, 95% CI: 0.56–1.13
- Difference in restricted mean survival over the first 48 months between ADT + apalutamide vs. ADT was 2.41 months (95% CI: -0.20–4.62)
PSA-PFS in the testosterone recovered subset:
- ADT + apalutamide vs. ADT: HR=0.72, 95% CI: 0.55–0.93, p=0.03
- 78% of patients recovered their testosterone levels

- ADT + apalutamide + abiraterone vs. ADT: HR=0.67, 95% CI: 0.50–0.90, p=0.008
- 68% of patients recovered their testosterone levels

Notable differences between the two trials were as follows:
- EMBARK allowed for the inclusion of patients who had received radiotherapy, in addition to radical prostatectomy, whereas PRESTO included only post-radical prostatectomy patients
- EMBARK included an ARPI (enzalutamide) monotherapy arm, whereas PRESTO did not
- EMBARK incorporated a ‘treatment holiday’ period in PSA responders by week 37, whereas treatment in PRESTO was for a fixed duration of 52 weeks
- The primary endpoint in EMBARK was metastasis-free survival (MFS) by conventional imaging, whereas MFS was a secondary endpoint in PRESTO (conventional or next-generation imaging)

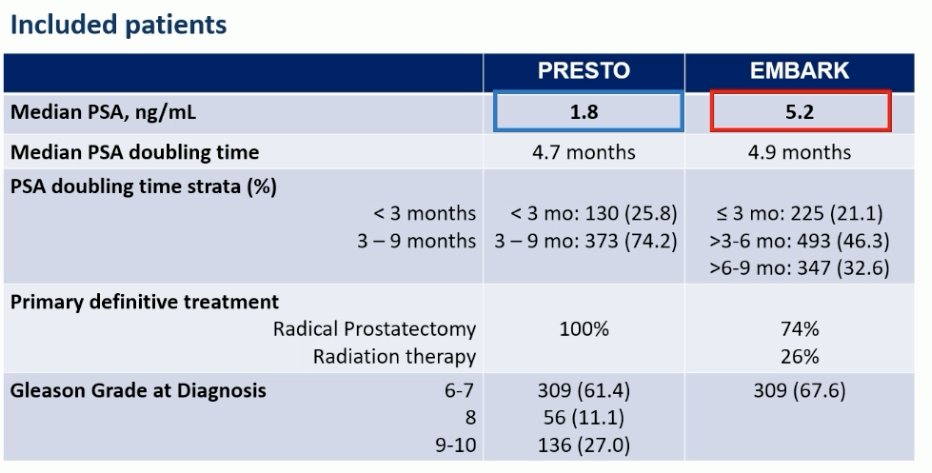
Furthermore, the PSA cut-off at study entry in the EMBARK trial was higher (≥1 ng/ml post-radical prostatectomy versus >0.5 ng/ml in PRESTO). Both trials included patients with a PSA doubling time of ≤9 months. These differences in the eligibility criteria were reflected in the baseline patient characteristics of each study.
Dr. Tilki noted that had the patients in PRESTO and EMBARK undergone a PSMA PET/CT, then it is estimated that ~80% would have had PET-detected metastases.1

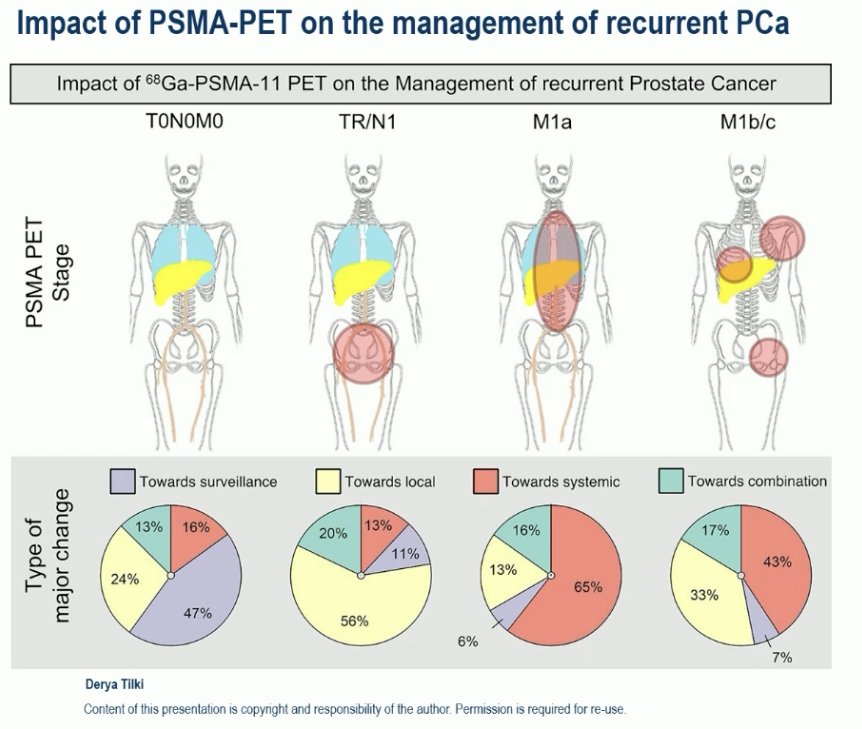
Why is this significant? Dr. Tilki noted that the utilization of PSMA PET in this patient population leads to management changes in more than half of patients with biochemical recurrence.2
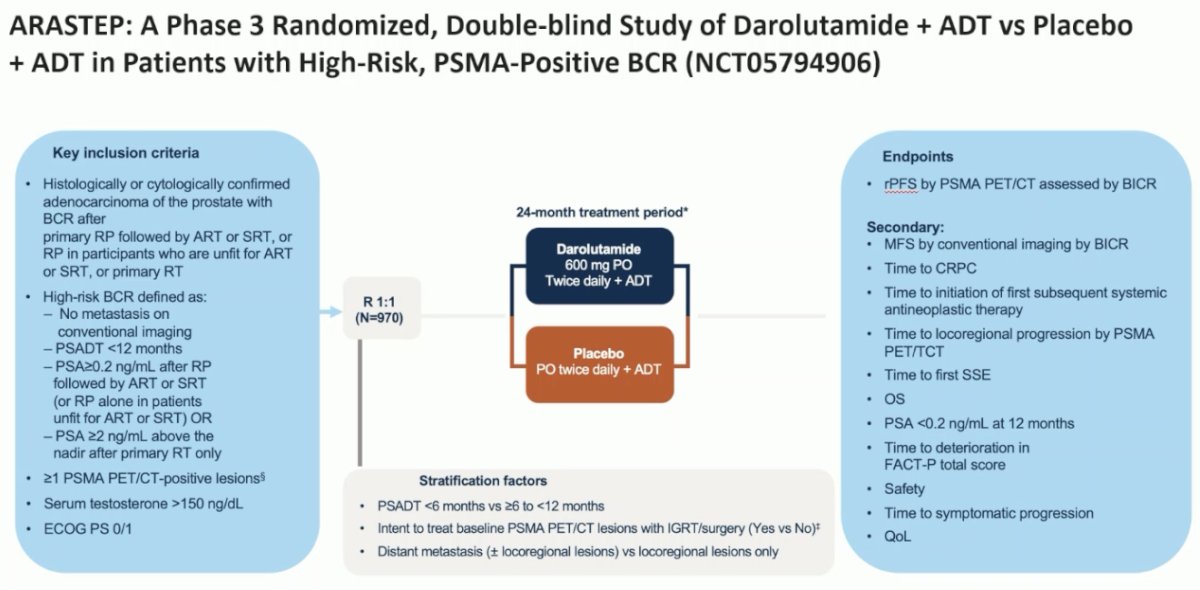
There are ongoing studies that are incorporating PSMA PET into their study design. ARASTEP (NCT05794906) will evaluate whether darolutamide, when added to ADT, improves radiologic progression-free survival by PSMA PET/CT versus placebo + ADT in patients with biochemically recurrent prostate cancer following primary therapy and PSMA PET/CT-positive lesions.
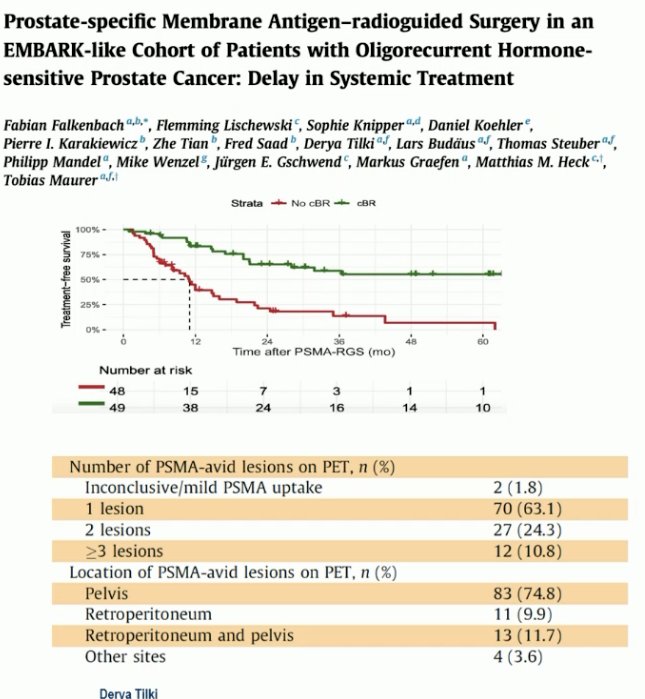
In addition to ARPI intensification in the BCR setting, additional treatment modalities evaluated have included metastasis-directed therapy (MDT), both to delay use of hormone therapy and in conjunction with systemic therapy. She highlighted a recent paper from her group that evaluated PSMA-radioguided surgery in an EMBARK-like cohort of patients with oligorecurrent hormone-sensitive prostate cancer. At study inclusion (n=111), the median PSA was 2 ng/ml and the median PSA doubling time was 4 months. A complete biochemical response (PSA ≤0.2) was observed in 48% of men. In this group of responders, the two-year BCR-free and treatment-free survivals were 50% and 65%, respectively.4
She highlighted the EXTEND trial, which evaluated the addition of MDT to intermittent hormone therapy. This was a phase II trial that included men with oligometastatic prostate cancer (≤5 metastases) and were randomized 1:1 to MDT, consisting of definitive radiation therapy to all sites of disease and intermittent hormone therapy (combined therapy arm; n = 43) or to hormone therapy only (n = 44). A planned break in hormone therapy occurred 6 months after enrollment, after which hormone therapy was withheld until progression. At a median follow-up of 22 months, progression-free survival (PFS) was improved in the combined therapy arm (HR: 0.25, p<0.001. Eugonadal PFS was also improved with MDT compared with hormone therapy only (HR: 0.32, p=0.03).5 An updated report from this trial has also recently demonstrated that the addition of MDT improves radiographic progression-free survival (rPFS).6 Notably, only a small proportion of patients in either arm used an ARPI as part of their hormonal therapy regimen.

Dr. Tilki concluded with the following take-home messages from her discussant of PRESTO and EMBARK:
- EMBARK demonstrates both MFS and OS benefits for doublet therapy versus ADT alone (but no OS benefit for enzalutamide monotherapy), establishing enzalutamide plus ADT as a standard of care in high-risk biochemically recurrent prostate cancer
- Enzalutamide monotherapy remains a treatment option after weighing the risks and benefits in the context of shared decision-making
- Intensification when moved earlier in high-risk disease prolongs survival
- PRESTO provides supportive data for class effect in this regard (doublet better than singlet), but triplet not better than doublet
- The interpretation of PRESTO is limited by being underpowered for estimating the impact on longer-term endpoints and by the lack of intermittent scheduling
- Whether further intensification of treatment, potentially with additional PSMA PET metastasis-directed therapy, can lead to increased efficacy and longer treatment-free intervals requires prospective evaluation
- Concepts that are worthy of further prospective randomized evaluation
- ARPI doublet +/- MDT vs MDT monotherapy vs ARPI monotherapy + MDT
- Biomarker-selected combination therapies
- Cycle length: intermittent versus prolonged first cycle
Presented by: Derya Tilki, MD, Professor of Urology, Martini-Klinik Prostate Cancer Center, University Hospital Hamburg-Eppendorf, Hamburg, Germany
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: EMBARK Trial Reports Overall Survival Benefit for Enzalutamide with ADT in High-Risk Non-Metastatic Prostate Cancer - Stephen Freedland
- Holzgreve A, Armstrong WR, Clark KJ, et al. PSMA-PET/CT findings in patients with high-risk biochemically recurrent prostate cancer with no metastatic disease by conventional imaging. JAMA Netw Open. 2025; 8(1): e2452971.
- Fendler WP, Calais J, Eiber M, et al. Impact of ⁶⁸Ga-PSMA-11 PET on management of recurrent prostate cancer. J Nucl Med. 2020; 61(12):1793–1800.
- Morgans AK, Niazi T, Shore N, et al. Darolutamide plus androgen-deprivation therapy (ADT) in patients with high-risk biochemical recurrence (BCR) of prostate cancer: a phase 3, randomized, double-blind, placebo-controlled study (ARASTEP). J Clin Oncol. 2025;43(suppl 17):TPS5131.
- Falkenbach F, Lischewski F, Knipper S, et al. Prostate-specific membrane antigen-radioguided surgery in an EMBARK-like cohort of patients with oligorecurrent hormone-sensitive prostate cancer: delay in systemic treatment. Eur Urol Oncol. 2025; [epub ahead of print].
- Tang C, Sherry AD, Haymaker C, et al. Addition of metastasis-directed therapy to intermittent hormone therapy for oligometastatic prostate cancer: The EXTEND phase 2 randomized clinical trial. JAMA Oncol. 2023;9(6):825–834.
- Sherry AD, Siddiqui BA, Haymaker C, et al. Continuous androgen deprivation therapy with or without metastasis-directed therapy for oligometastatic prostate cancer: The multicenter phase 2 randomized EXTEND trial. Eur Urol. 2025;88(5):496–509.