(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress was host to a prostate, penile, and testicular cancers proffered paper session. Dr. Karim Fizazi presented CAPItello-281, a phase III trial of capivasertib + abiraterone versus placebo + abiraterone in PTEN-deficient patients with de novo metastatic hormone-sensitive prostate cancer (mHSPC).
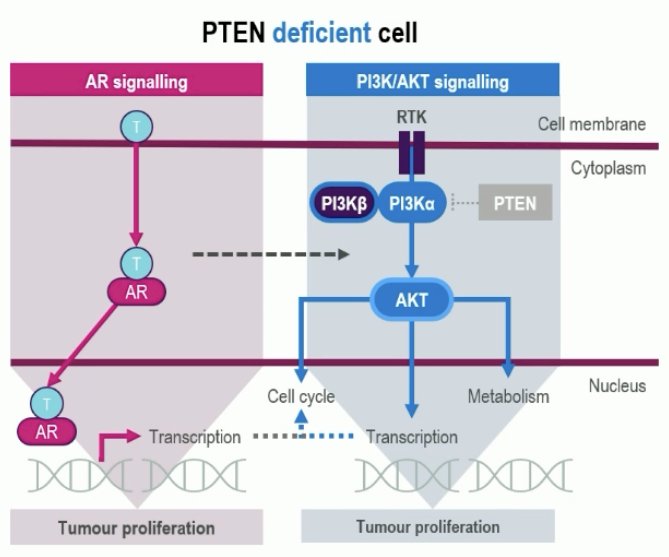
In PTEN-proficient hormone-sensitive tumor cells, androgen receptor (AR) signaling is the key driver of cellular proliferation.1 However, in PTEN-deficient tumor cells, there is an additional proliferative drive from upregulation of the PI3K/AKT pathway that complements and provides an alternative survival mechanism to AR signaling.2 Importantly, PTEN deficiency is associated with poor prognosis.2-4
Capivasertib is a potent, selective inhibitor of all three AKT isoforms (AKT1/2/3). Phase 2/3 studies have demonstrated a benefit for ipatasertib + abiraterone in PTEN-deficient mCRPC.2,3
CAPItello-281 is a global, multicenter, randomized, double-blind, phase III trial that included patients meeting the following eligibility criteria:
- De novo mHSPC
- PTEN deficiency: ≤10% of cells expressing PTEN by immunohistochemistry (IHC)
- Of 6,200 patients submitting tumor tissue, 97% had a valid IHC result, and 25% were PTEN-deficient
Eligible participants (n=1,012) were randomized 1:1 to:
- Capivasertib (400 mg BID, 4 days on & 3 days off) + abiraterone acetate (1,000 mg daily) + prednisone (5 mg daily) + ADT
- Placebo + abiraterone acetate +prednisone + ADT
The primary endpoint was investigator-assessed radiographic progression-free survival (rPFS). Secondary endpoints were:
- Overall survival (OS)
- Time to first subsequent therapy
- Symptomatic skeletal event-free survival
- Time to pain progression
- Time to castration resistance
- Time to PSA progression

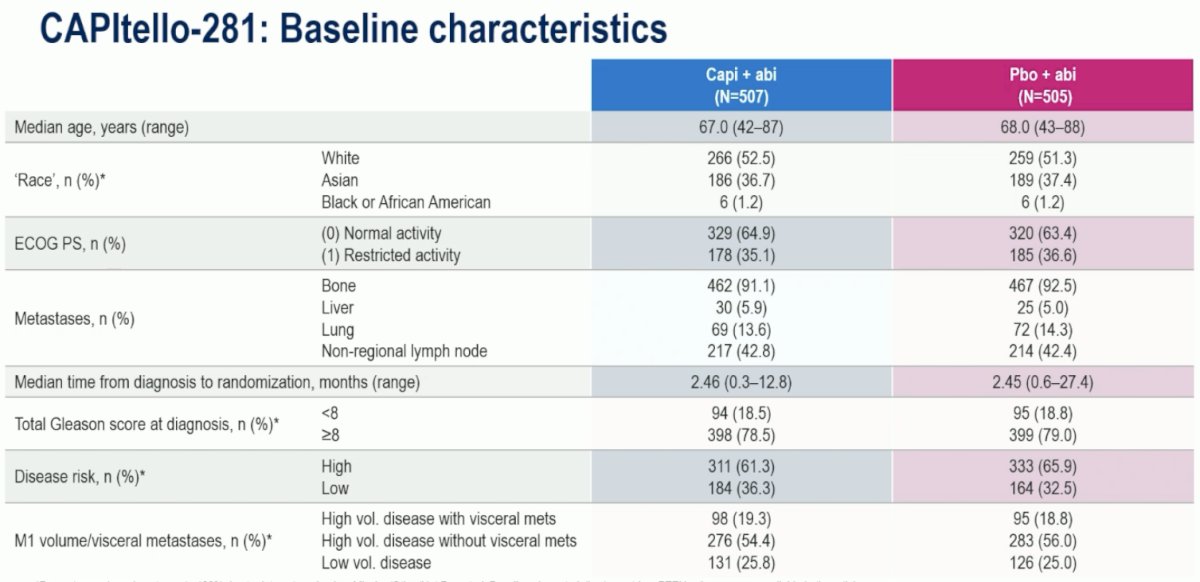
The baseline characteristics were well-balanced between the study arms. Consistent with the poor-risk profile of PTEN-deficient tumors, most patients had high Gleason Scores (≥8: ~80%), high-risk disease (61-66%), and high-volume disease (75%).
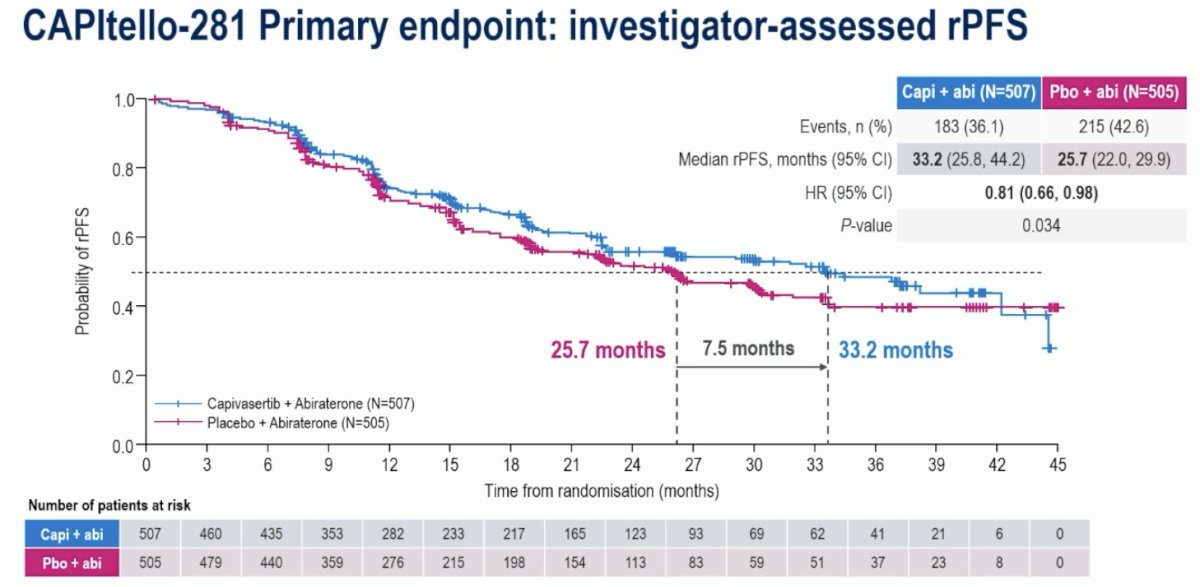
The study met its primary endpoint with capivasertib prolonging rPFS by 7.5 months (median: 33.2 vs 25.7 months; HR: 0.81, 95% CI: 0.66-0.98, p=0.034). Dr. Fizazi noted that despite this improvement, the median OS of 33.2 months in the capivasertib arm, and especially 25.7 months in the placebo arm, underscores the poor prognoses of PTEN-deficient mHSPC.
Subgroup analyses demonstrated consistent benefits across all subgroups in favor of capivasertib + abiraterone:

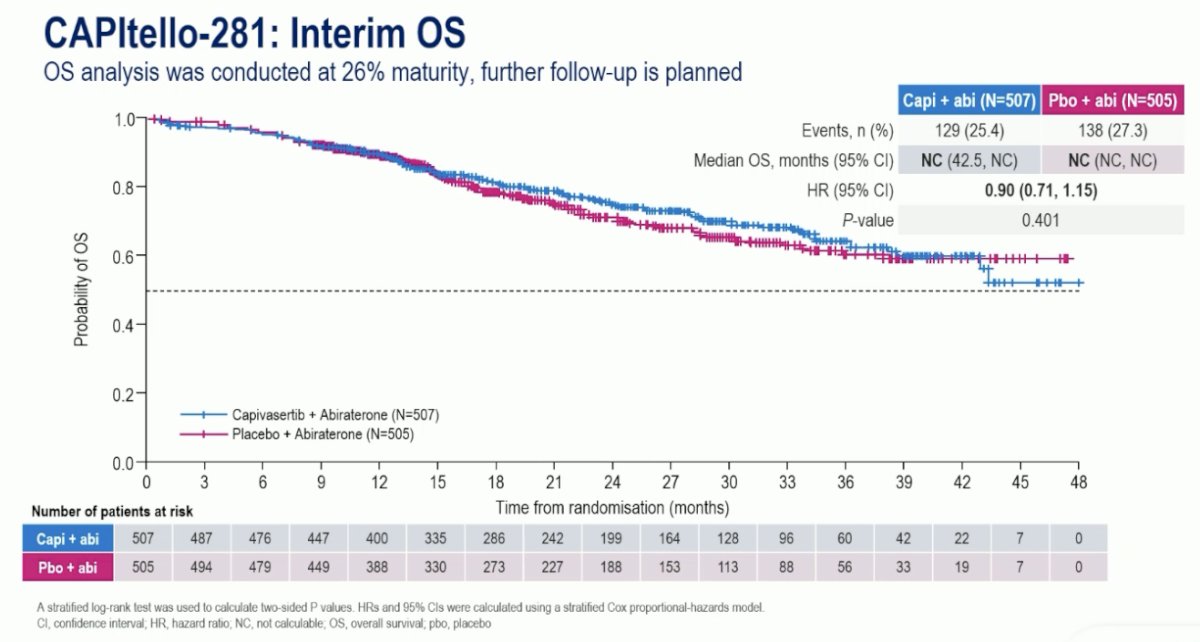
Key secondary endpoints were tested according to the hierarchical testing procedure. OS data are immature to date but demonstrate a favorable early benefit in favor of capivasertib + abiraterone (HR: 0.90, 95% CI: 0.71-1.15). Formal testing was halted following OS analysis, given the hierarchical nature. Key secondary endpoints are summarized below and consistently favored capivasertib + abiraterone.
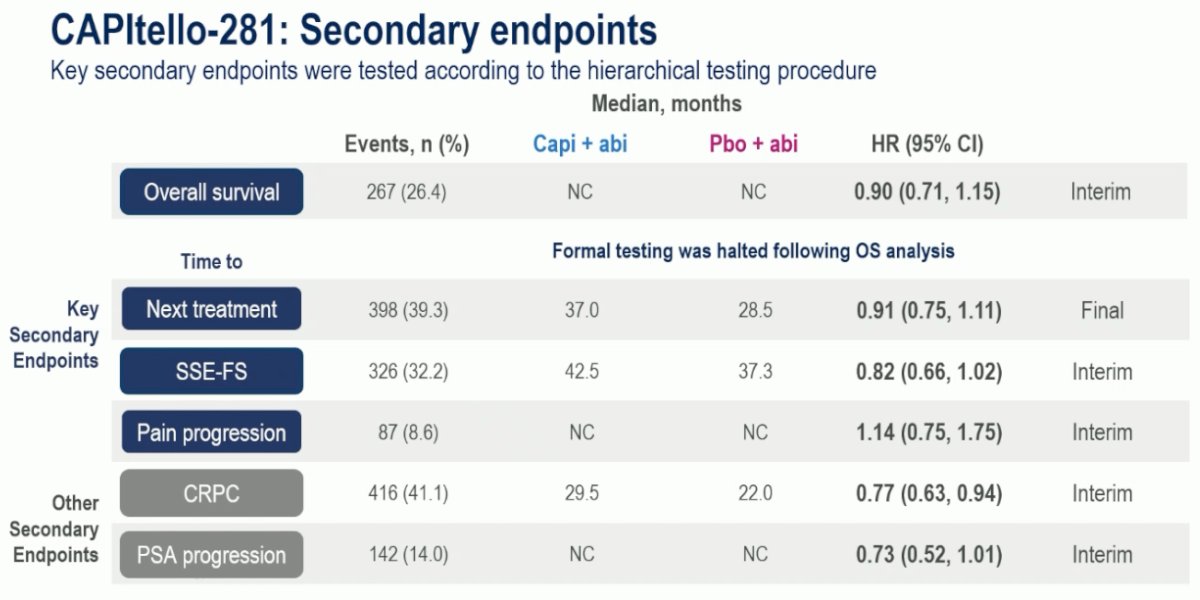
Diving deeper into the secondary endpoints, Dr. Fizazi noted that the OS analysis was conducted at 26% maturity (HR: 0.90, 95% CI: 0.71–1.15, p=0.401):
Patients in the capivasertib + abiraterone arm had an 18% reduction in the rate of symptomatic skeletal events, with a 5-month improvement in the median symptomatic skeletal event-free survival (median: 42.5 vs 37.3 months; HR: 0.82, 95% CI: 0.66-1.02, p=0.08):

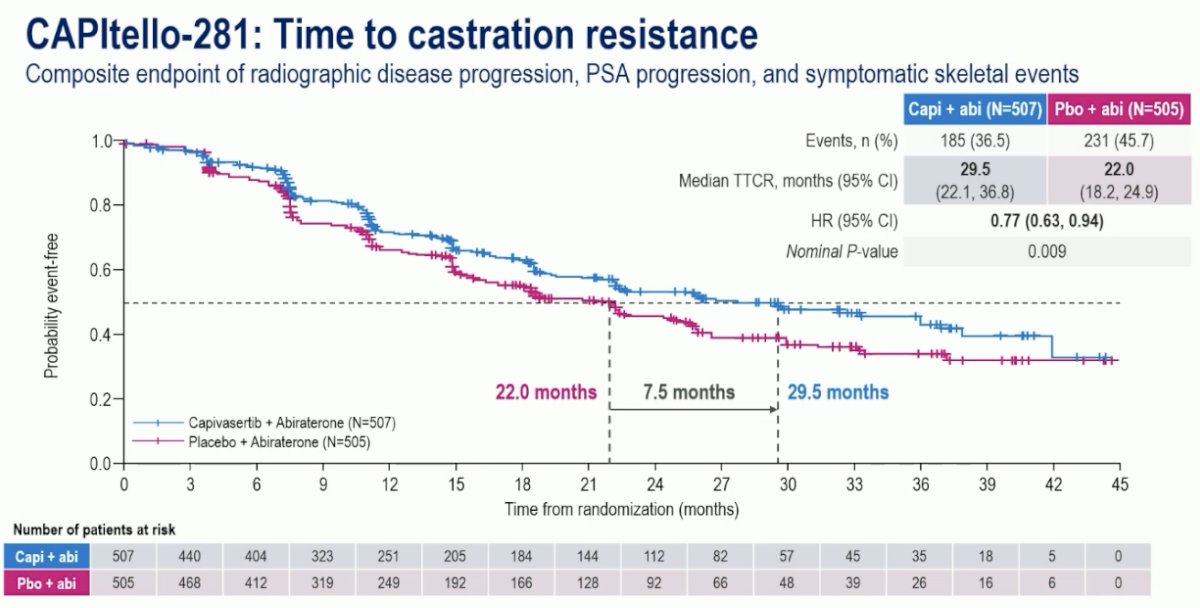
Time to castration resistance was similarly improved by 7.5 months with capivasertib + abiraterone (median: 29.5 vs 22 months; HR: 0.77, 95% CI: 0.63-0.94, p=0.09):
Dr. Fizazi highlighted that early PSA progression events were less common in both arms, particularly when compared to clinical progression events, highlighting that clinical progression often occurs earlier than PSA progression in PTEN-deficient mHSPC. Regardless, capivasertib + abiraterone delayed PSA progression-free survival by 27% (HR: 0.73, p=0.06).

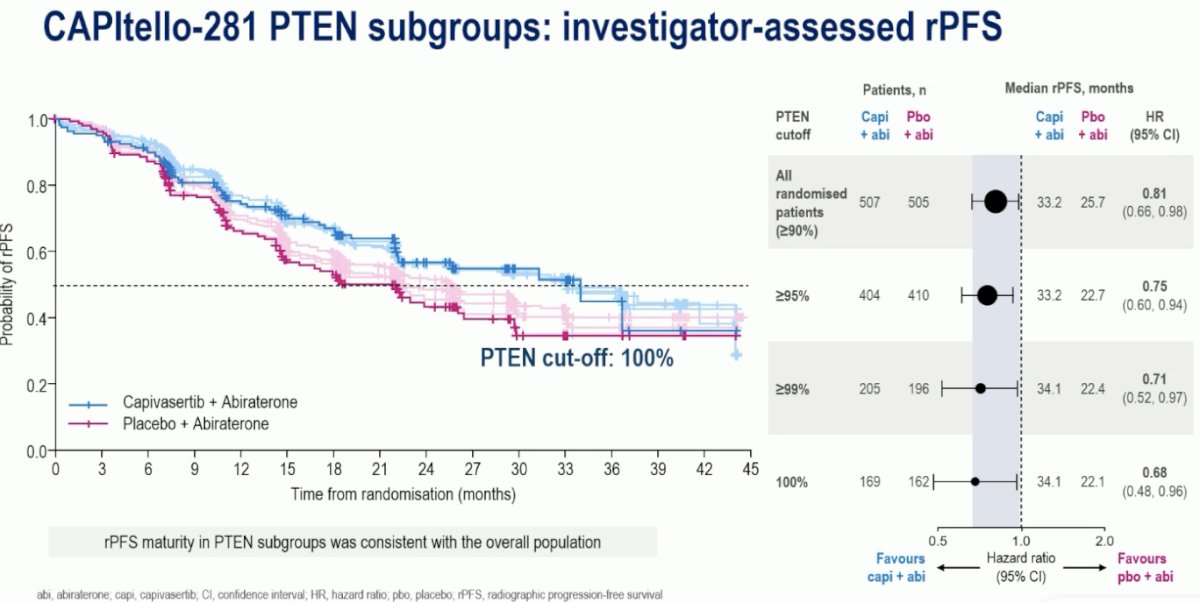
Increasing PTEN deficiency was associated with a progressive relative improvement in the rPFS hazard ratio with the addition of capivasertib to abiraterone acetate:

Notably, the rPFS survival outcomes worsened as PTEN deficiency increased:
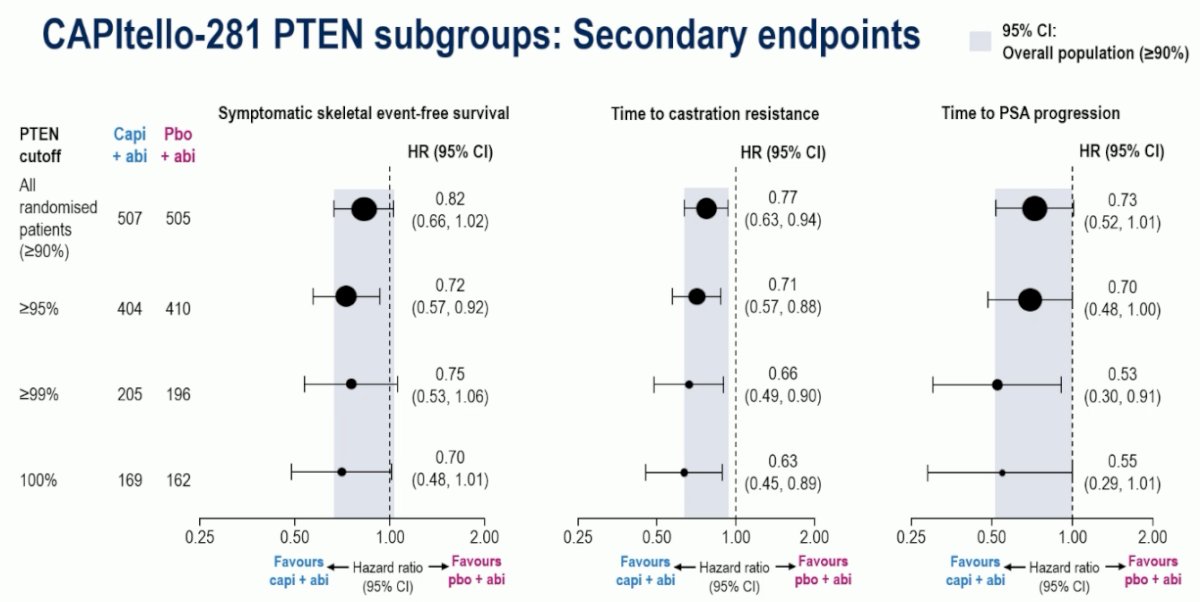
A relative improvement with capivasertib addition was also observed across the secondary endpoints as PTEN deficiency increased:
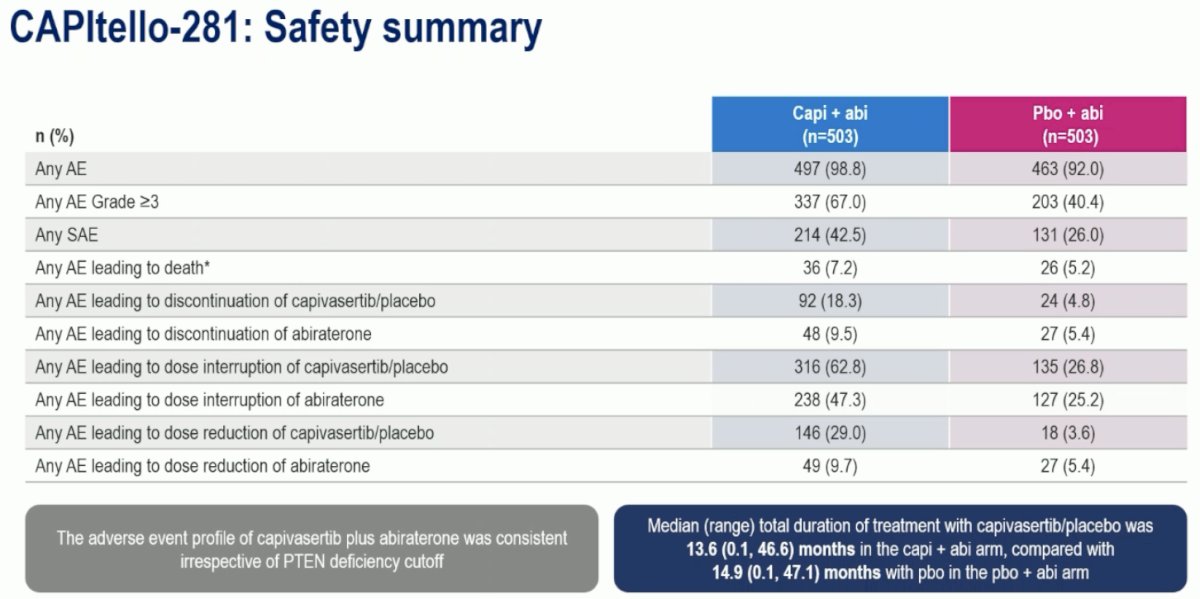
The incidence of grade ≥3 adverse events was increased with capivasertib (67% vs 40.4%). Adverse events leading to treatment discontinuation were observed in 18% and 5%, respectively. The median duration of treatment was ~14 months in both arms.
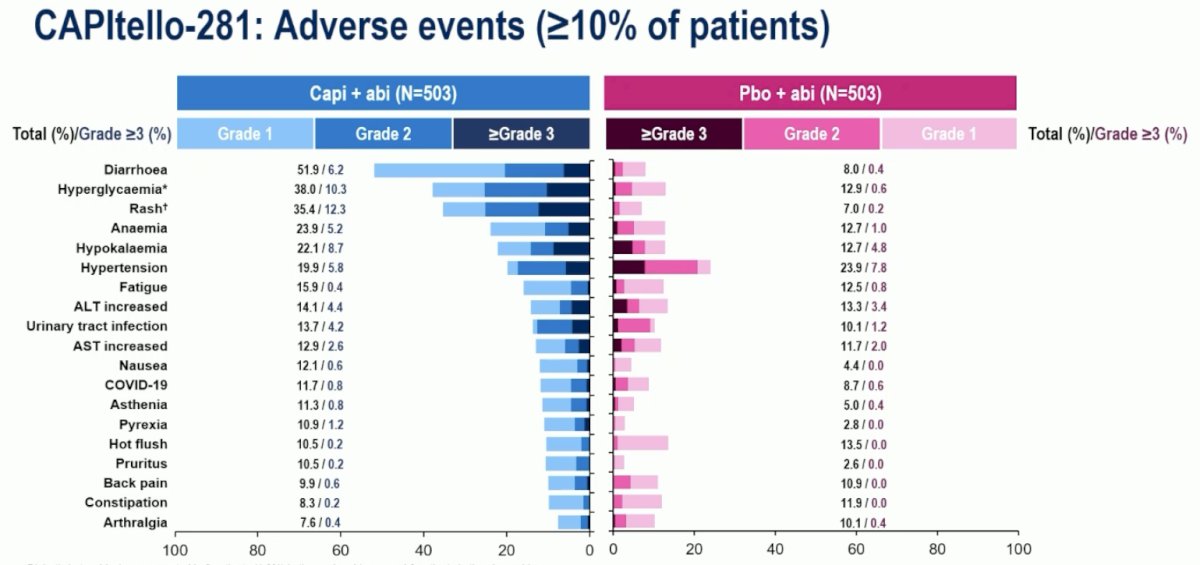
The most common adverse events in the capivasertib arm were diarrhea (52%), hyperglycemia (38%), and rash (35%). Abiraterone-specific adverse events (i.e., hypertension, hypokalemia) were similar between both arms.
Dr. Fizazi concluded his presentation of the CAPItello-281 trial as follows:
- Patients with PTEN-deficient mHSPC have a poor prognosis and reduced benefit from the current standard of care therapy
- CAPltello-281 met its primary objective, showing a statistically significant PFS benefit with capivasertib + abiraterone versus placebo + abiraterone
- Median rPFS: Capivasertib + abiraterone: 33.2 months versus placebo + abiraterone: 25.7 months (HR: 0.81, 95% Cl: 0.66–0.98; p=0.034)
- Consistent benefits were also observed in secondary endpoints and clinically relevant pre-defined subgroups
- Overall survival data were immature, and further follow-up is planned
- Post-hoc analyses evaluating increased PTEN cutoffs showed greater treatment effect with capivasertib + abiraterone
- The most common Grade ≥3 adverse events of rash and hyperglycemia are expected with AKT inhibition
- Capivasertib + abiraterone represents a potential first-in-class targeted treatment for patients with PTEN-deficient mHSPC
Presented by: Karim Fizazi, MD, PhD, Professor, Department of Medicine, Institut Gustave Roussy, Paris, France
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Quistini A, Rossi G, Bianchi M, et al. Disitamab vedotin in HER2-expressing urothelial carcinoma: current evidence and future perspectives. Res Rep Urol. 2025; 17:211–223.
- de Bono JS, Scher HI, Montgomery RB, et al. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res. 2019; 25:928–936.
- Sweeney C, Chen Y-H, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: long-term survival analysis of the randomized CHAARTED trial. Lancet. 2021; 398:131–142.
- Rathkopf D, Smith MR, Sternberg CN, et al. Results from the phase 3 ARASENS trial of darolutamide plus ADT and docetaxel in metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2025; 43:abstr 5096.
Related Content:
PTEN Loss in mHSPC: Why It Changes How We Monitor and Treat Patients - Daniel George, Neal Shore, David Morris, & Neeraj Agarwal
PTEN Loss and the Future of Precision Treatment in mHSPC - Karim Fizazi & Noel Clarke