(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to a prostate, penile, and testicular cancers proffered paper session. Dr. Rahul Aggarwal presented the final results of PRESTO (AFT-19), an open-label phase III trial of combined androgen blockade in patients with high-risk, biochemically relapsed prostate cancer.
Men with biochemically recurrent prostate cancer following radical prostatectomy and a short PSA doubling time (PSADT) are at high risk for the development of distant metastases and prostate cancer-related mortality. Intermittent androgen deprivation therapy (ADT) is a standard of care treatment to reduce the risk of metastasis, while balancing the risk of side effects. The PRESTO study investigators hypothesized that combination hormone therapy may lead to more durable PSA suppression, enabling longer treatment-free intervals within a framework of intermittent therapy
PRESTO is a randomized phase III, open-label trial in patients with biochemically relapsed prostate cancer and PSA doubling time ≤ 9 months, without distant metastases on conventional imaging (NCT03009981). Patients were randomized 1:1:1 to receive a finite 52-week treatment course with ADT, ADT + apalutamide, or ADT + apalutamide + abiraterone acetate plus prednisone, stratified by PSA doubling time (< 3 vs 3–9 months).
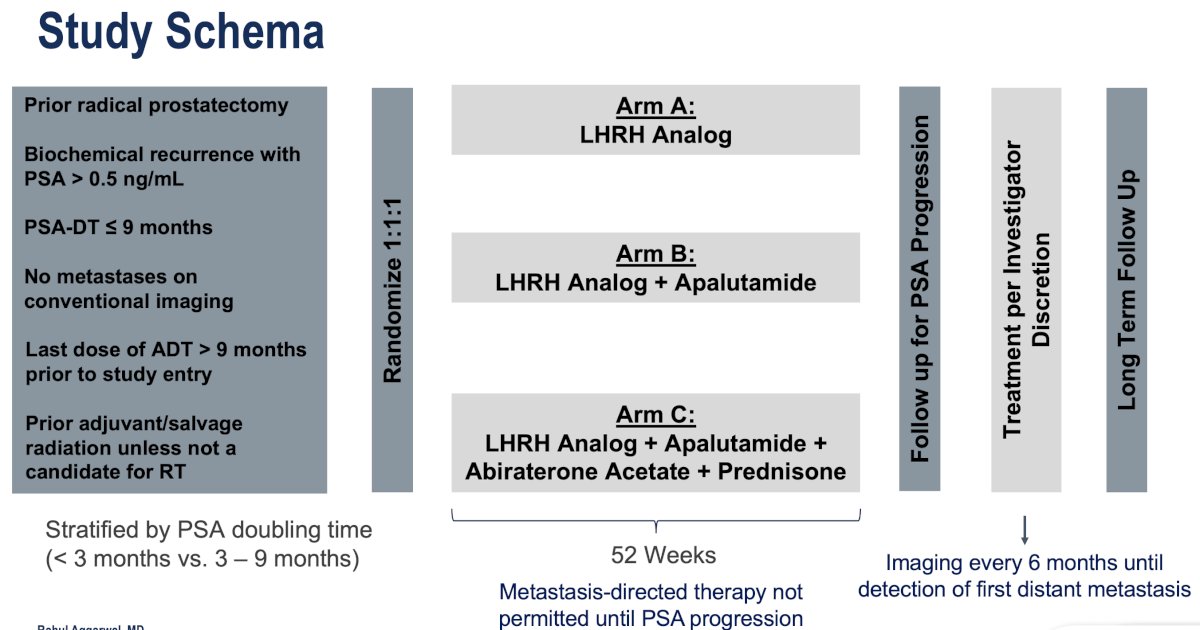
Study comparisons were performed between each of the experimental arms (Arms B and C) and the control arm A. The study objectives were as follows:
- Primary: PSA progression-free survival (PSA-PFS)
- Results have previously been published in the Journal of Clinical Oncology.1
- Both arms significantly prolonged PSA-PFS (ADT + apalutamide: 25 versus 20 months, HR: 0.52, p<0.001; ADT + apalutamide + abiraterone: 26 versus 20 months; HR: 0.48, p<0.001)
- Results have previously been published in the Journal of Clinical Oncology.1
- Secondary:
- Metastasis-free survival
- Time to castration resistance
- PSA progression-free survival in a testosterone-recovered population (serum Testosterone >50 ng/dL)
- Safety
- Quality of life (QoL)
- Presented at ASCO 2024: No difference in on-treatment QoL between the study arms
In this report, Dr. Aggarwal presented the results of the 1st four secondary outcomes above. The statistical plan was to compare each experimental arm versus the control arm with respect to:
- Metastasis-free survival: Time from randomization to detection of first distant metastasis by any imaging modality (conventional or next-generation) or death
- Cox proportional hazards (pre-planned)
- 48-month restricted mean survival time (post hoc)
- Time to castration resistance: Time from randomization to castration resistance as defined by progression by PCWG3 in setting of castrate serum T (< 50 ng/dL)
- PSA progression-free survival in testosterone-evaluable population (T > 50 ng/dL)
- Time to subsequent treatment: Time from randomization to first subsequent treatment (focal or systemic)
- This was a post-hoc secondary objective, whereas the other three were pre-planned
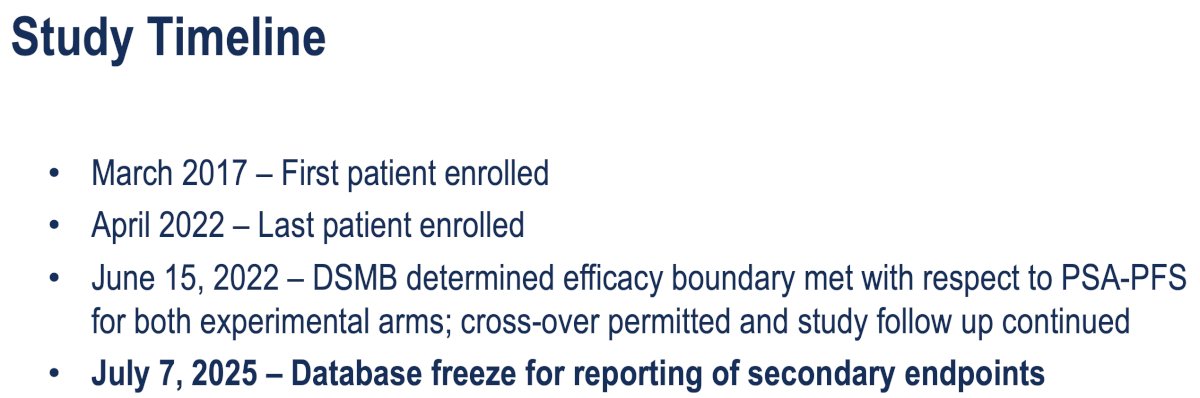
The study timeline is summarized below:
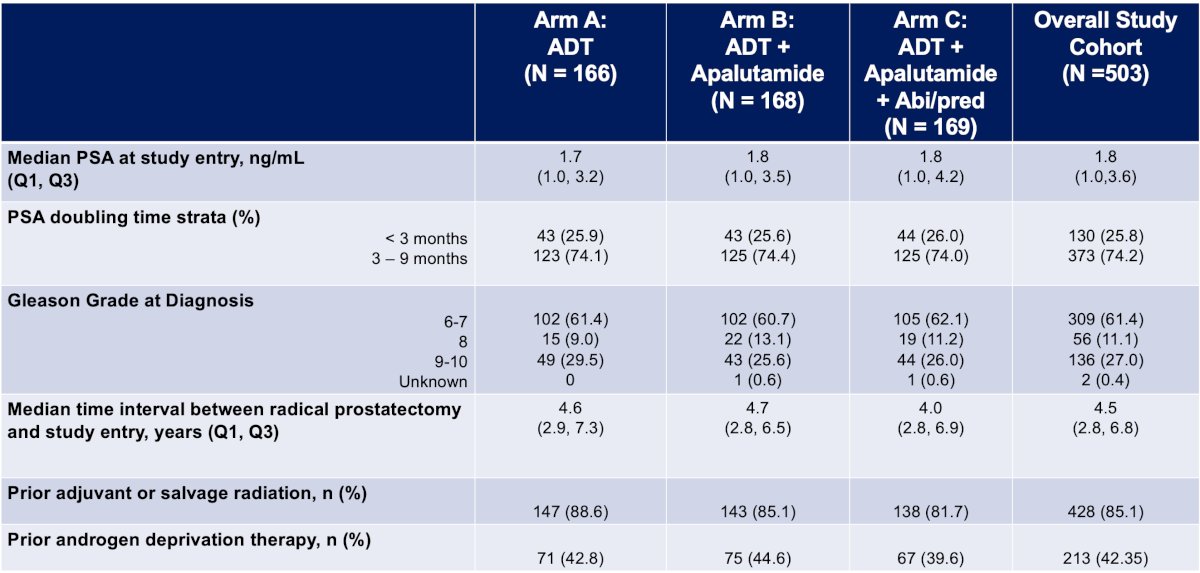
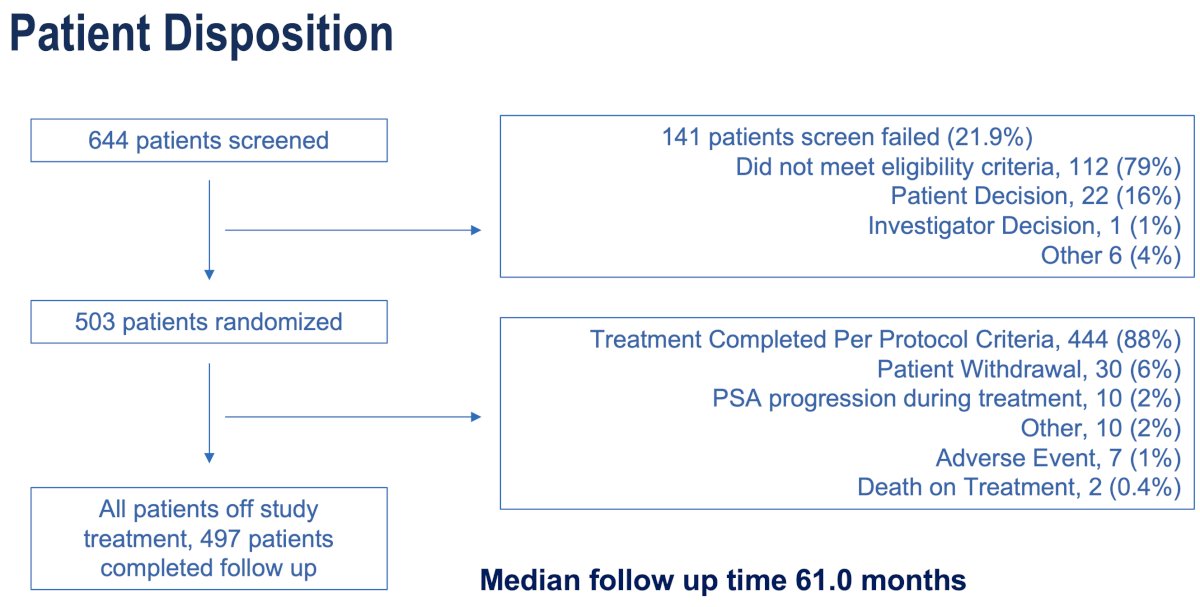
The baseline study population characteristics are summarized below. The median patient age was 67 years. The median serum PSA level at study entry was 1.8 ng/ml. The PSADT was <3 months in 26% and 3–9 months in 74%. The median time interval between radical prostatectomy and study entry was 4.5 years and was well-balanced between the study arms. 85% of patients had received prior adjuvant or salvage radiation, and 42% had received prior ADT.
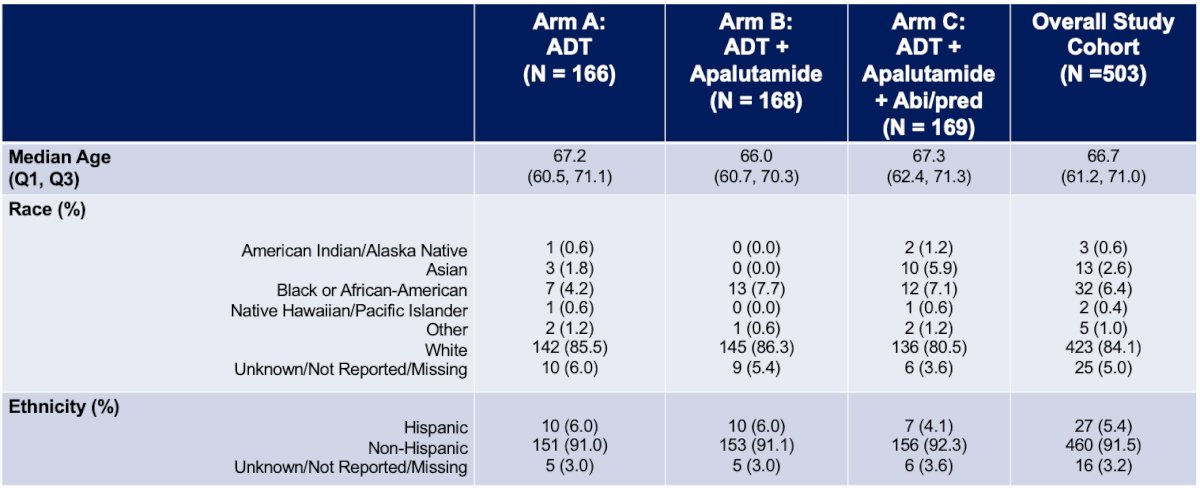
The study cohort included 503 patients who underwent randomization. The median follow-up was 61 months.
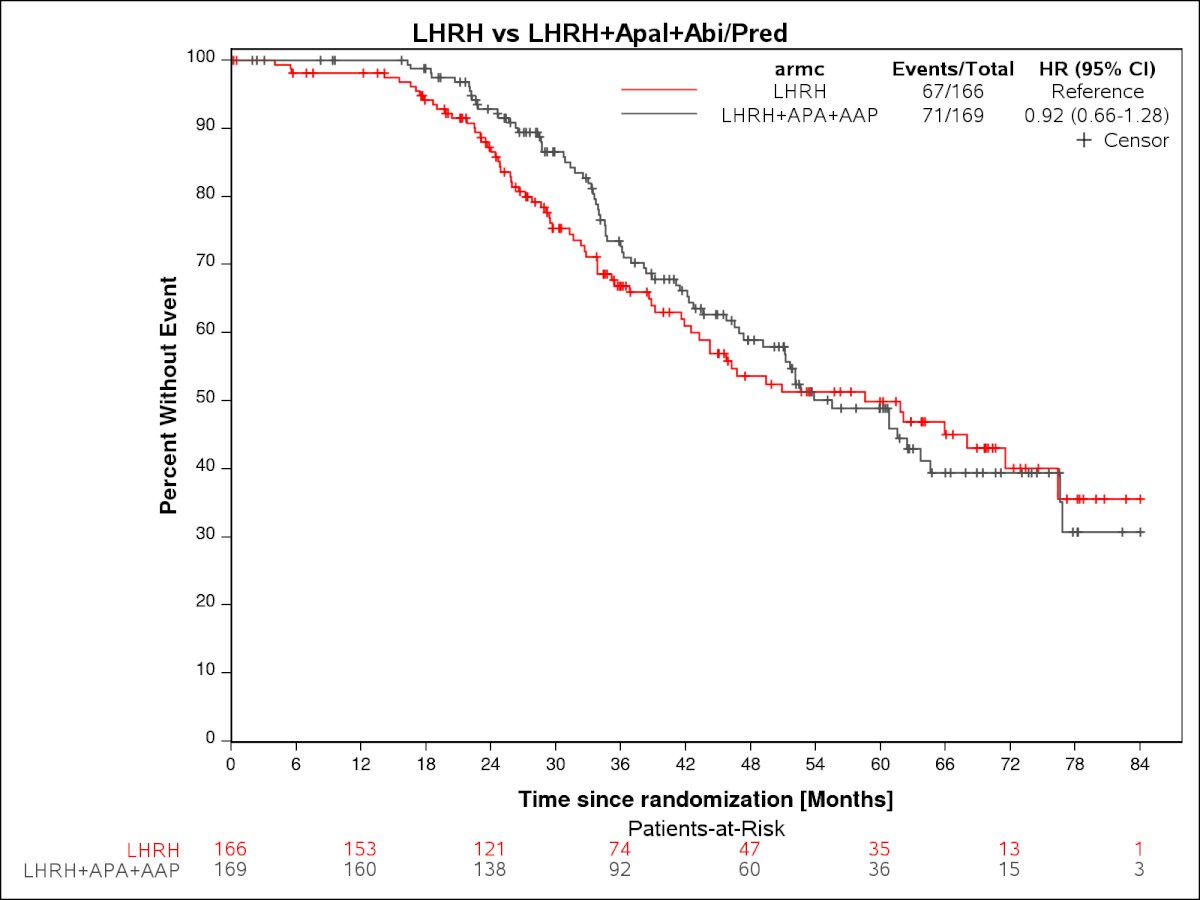
For the outcome of metastasis-free survival:
- ADT + apalutamide vs. ADT: HR=0.80, 95% CI: 0.56–1.13
- Difference in restricted mean survival over the first 48 months between ADT + apalutamide vs. ADT was 2.92 months (95% CI: 0.45–5.39)
- ADT + apalutamide + abiraterone vs. ADT: HR=0.92, 95% CI: 0.56–1.13
- Difference in restricted mean survival over the first 48 months between ADT + apalutamide vs. ADT was 2.41 months (95% CI: -0.20–4.62)
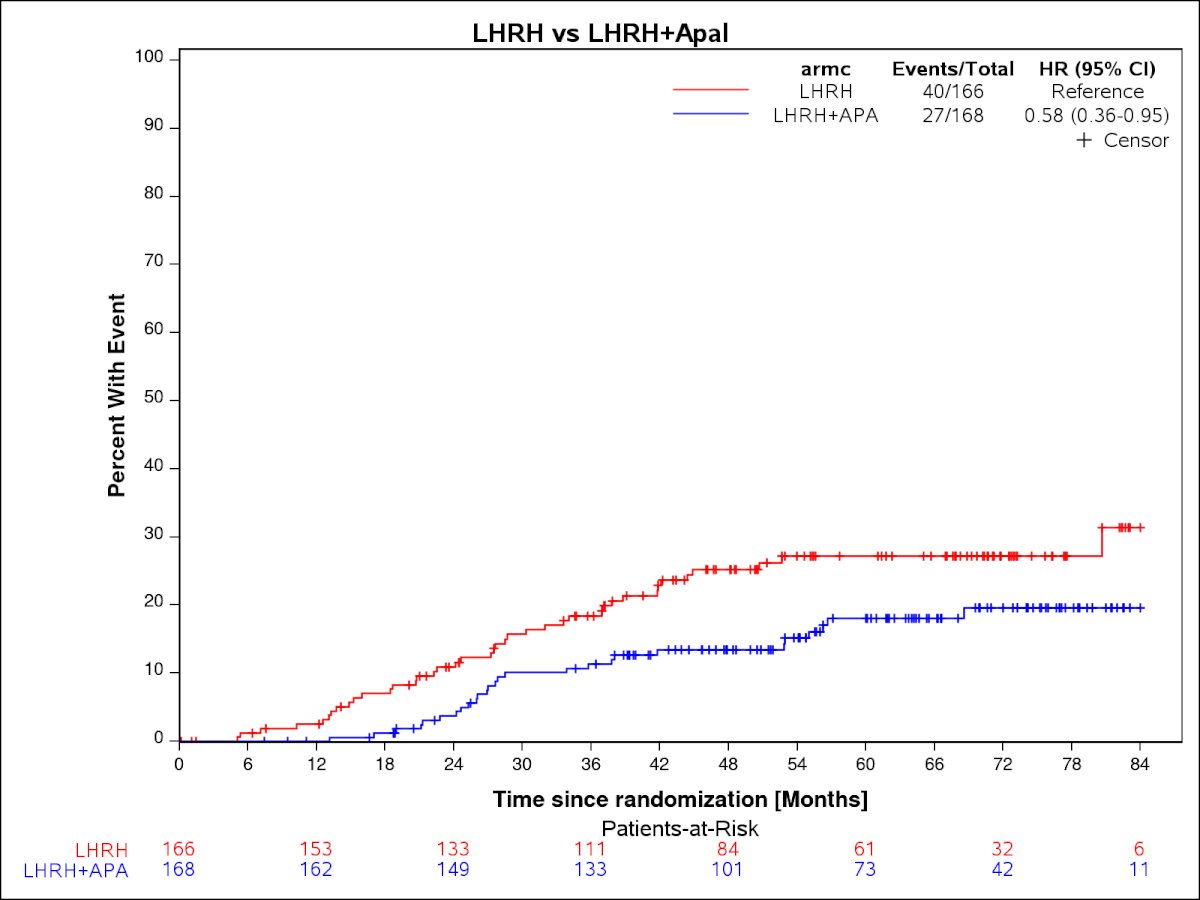
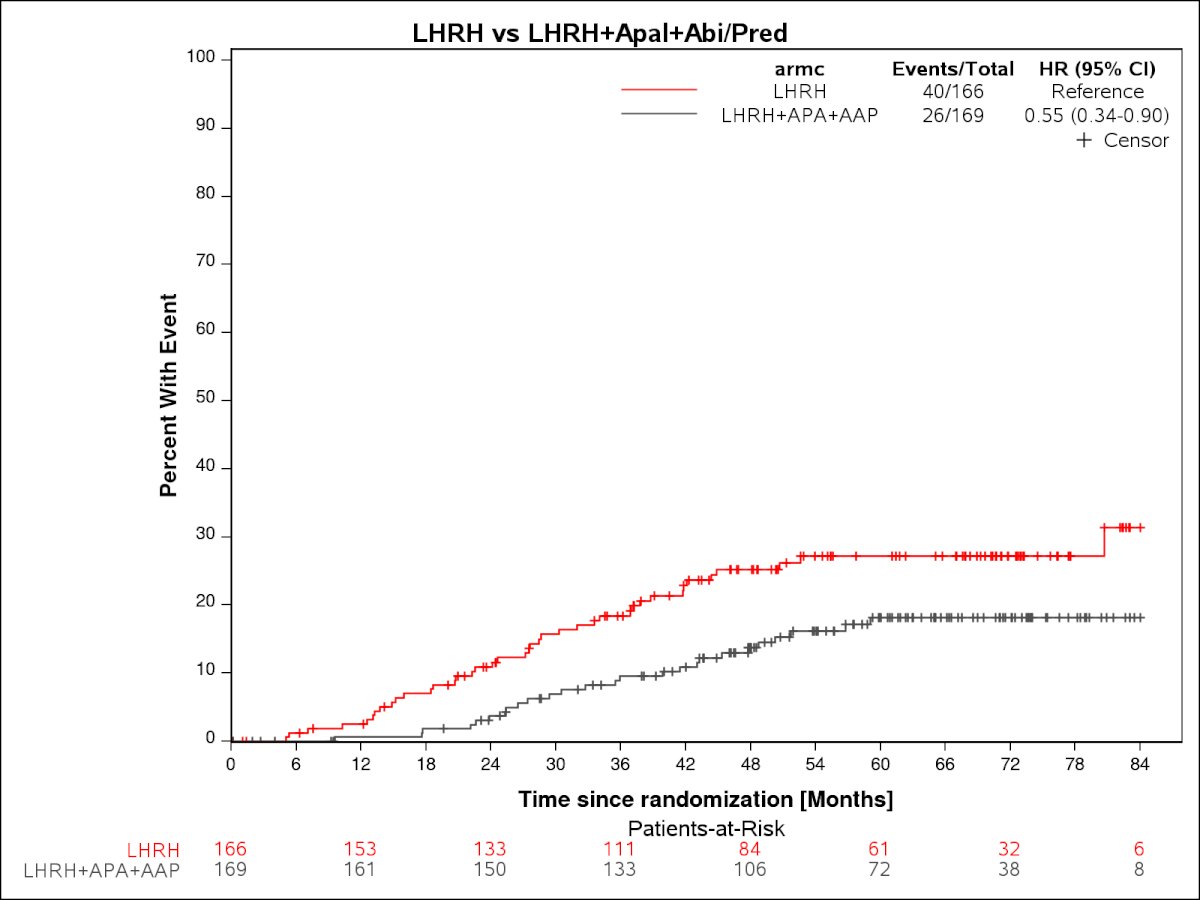
Time to CRPC:
- ADT + apalutamide vs. ADT: HR=0.58, 95% CI: 0.36–0.95, p=0.03
- ADT + apalutamide + abiraterone vs. ADT: HR=0.55, 95% CI: 0.34–0.90, p=0.02
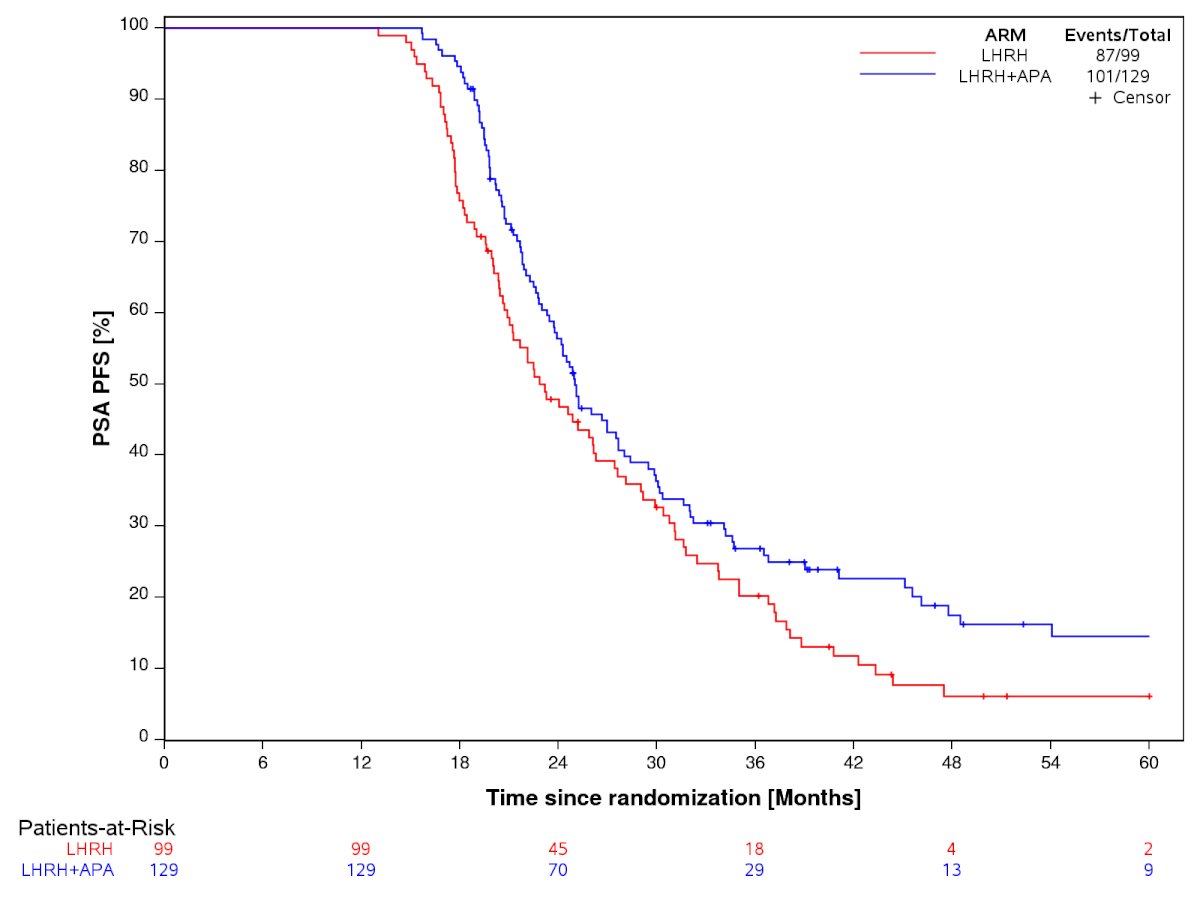
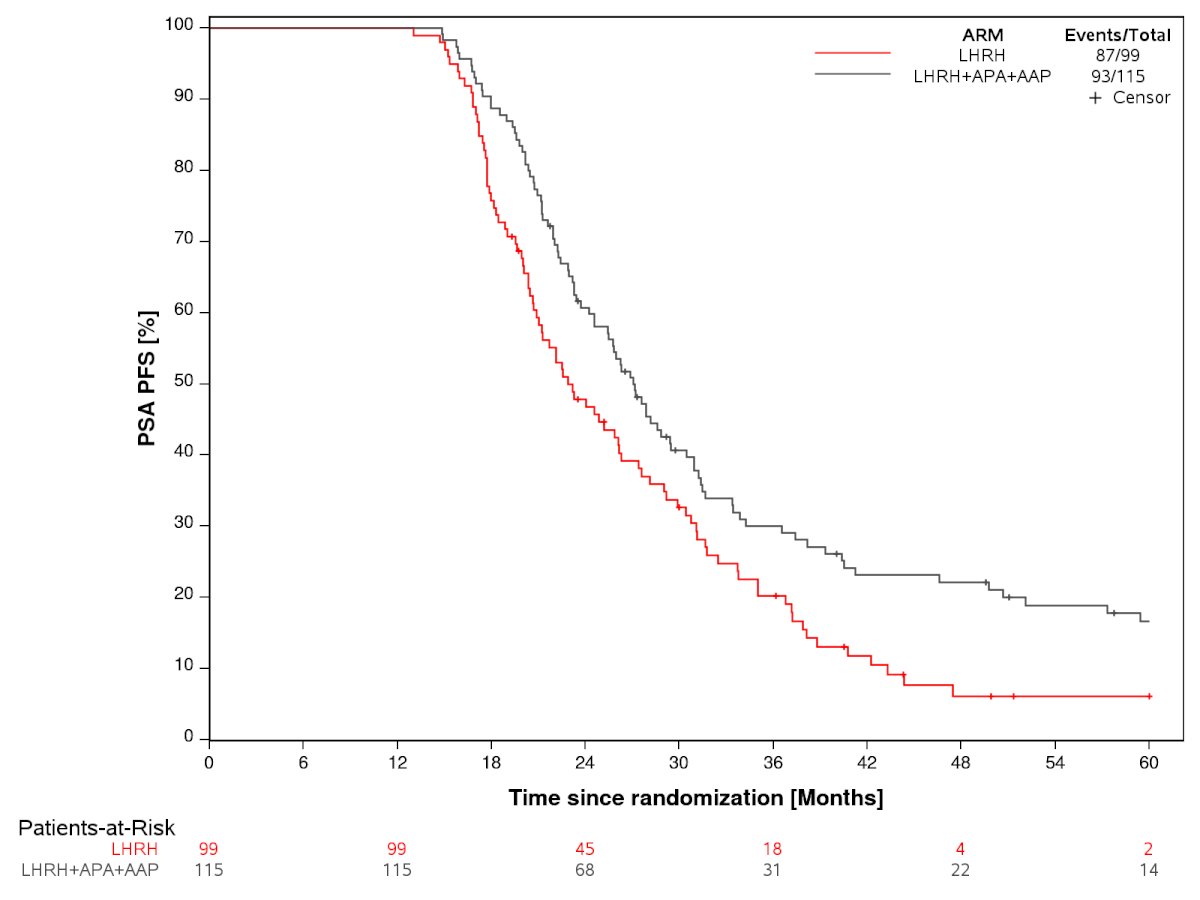
PSA-PFS in the testosterone recovered subset:
- ADT + apalutamide vs. ADT: HR=0.72, 95% CI: 0.55–0.93, p=0.03
- 78% of patients recovered their testosterone levels
- ADT + apalutamide + abiraterone vs. ADT: HR=0.67, 95% CI: 0.50–0.90, p=0.008
- 68% of patients recovered their testosterone levels
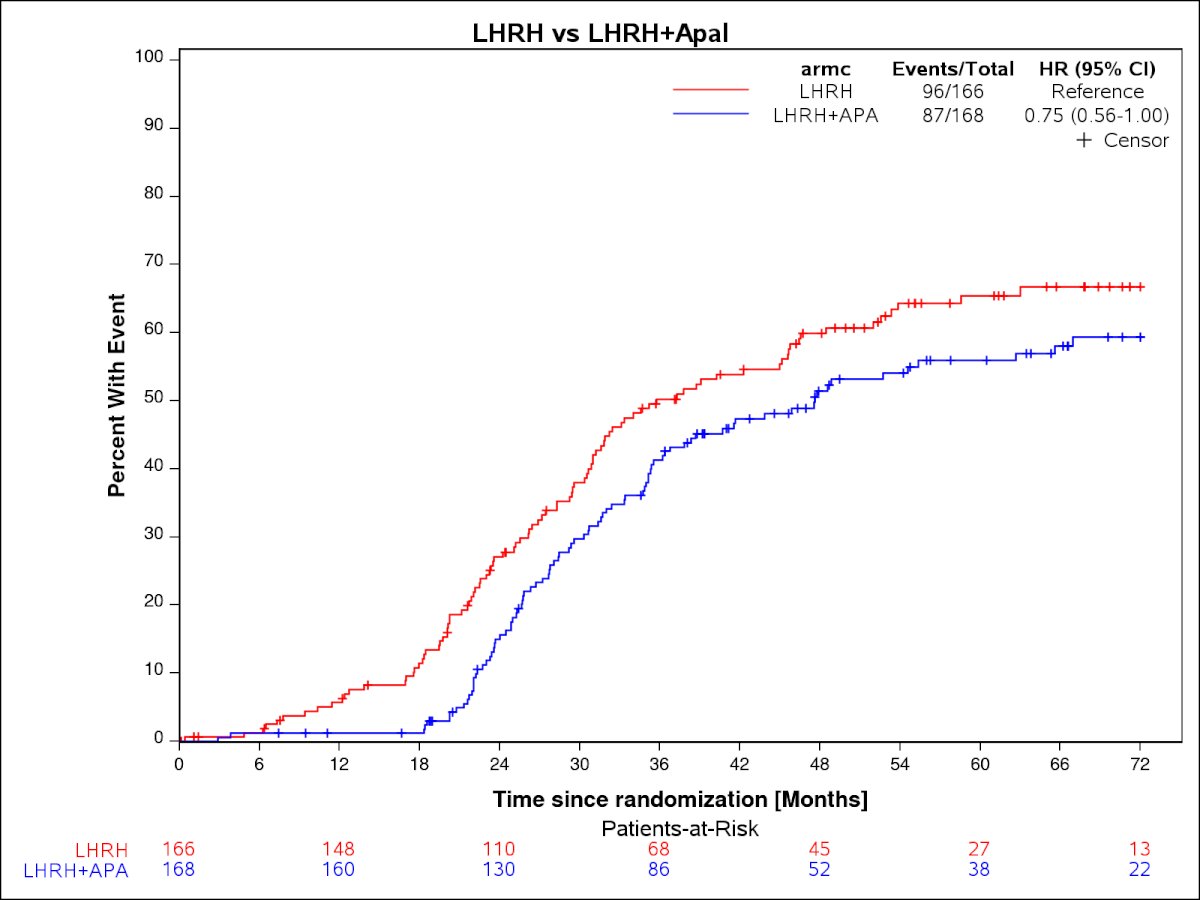
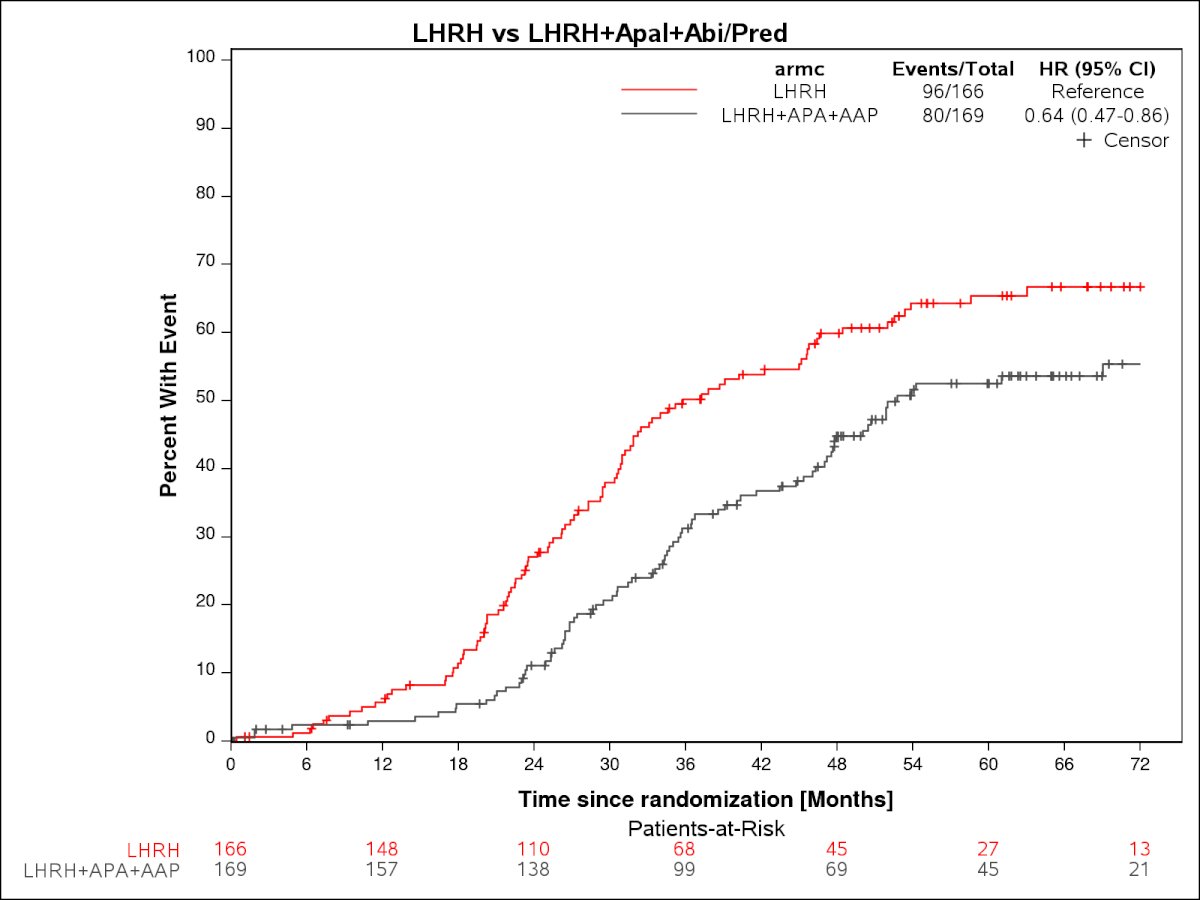
Time to subsequent therapy, including both focal and systemic therapies administered:
- ADT + apalutamide vs. ADT: HR=0.75, 95% CI: 0.56–1.00, p=0.0078
- ADT + apalutamide + abiraterone vs. ADT: HR=0.64, 95% CI: 0.47–0.86, p=0.0028
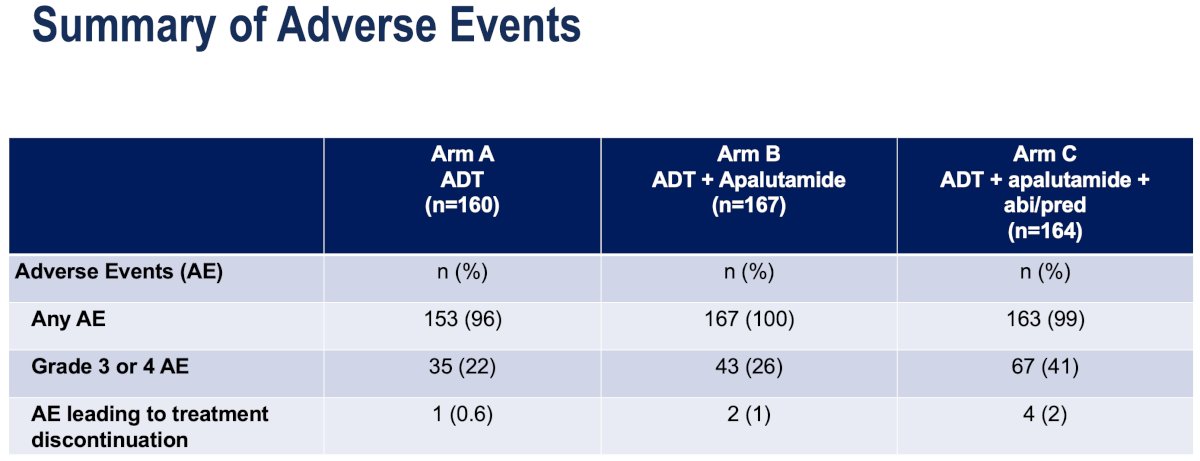
Grade 3-4 adverse events were most common in the ADT + apalutamide + abiraterone arm (41%), compared to 26% and 22% in the ADT + apalutamide and ADT arms, respectively. Adverse events leading to treatment discontinuation were uncommon.
The most common grade ≥2 adverse events by treatment arm are summarized below:

Notable study limitations were as follows:
- Next-generation imaging (e.g. Fluciclovine or PSMA PET) was not required at screening
- Truly M0 biochemically recurrent CSPC population shrinking with stage migration
- The study was relatively underpowered to estimate the impact on longer term endpoints
- Relatively few MFS and CRPC events observed with median follow up of approximately 5 years
- Pragmatic MFS endpoint by either conventional or next-generation imaging
- Reflective of the shifting landscape in the restaging of patients with biochemical recurrence during the course of the study
- This was an open-label study without central imaging review
- Metastasis-directed treatment was not permitted during study treatment until PSA progression was met
Dr. Aggarwal concluded with the following take home messages:
- Combined androgen signaling blockade with ADT plus apalutamide, given for a finite treatment period of 12 months, improves clinically relevant long term endpoints including metastasis-free survival, time to castration resistance, and time to subsequent treatment in patients with high-risk biochemically recurrent prostate cancer.
- There did not appear to be additional benefit with the further inclusion of abiraterone acetate + prednisone, along with added toxicity.
- The role of combined androgen blockade in the current era of next-generation imaging and metastasis-directed treatment for recurrent oligometastatic HSPC remains to be defined.
Presented by: Rahul Raj Aggarwal, MD, Professor, Department of Medicine, University of California, San Francisco, CA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: PRESTO Trial Final Results for High-Risk Biochemically Recurrent Prostate Cancer - Rahul Aggarwal
References:
- Aggarwal R, Heller G, Hillman DW, et al. PRESTO: A Phase III, Open-Label Study of Intensification of Androgen Blockade in Patients With High-Risk Biochemically Relapsed Castration-Sensitive Prostate Cancer (AFT-19). J Clin Oncol. 2024; 42(10):1114-1123.