(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to a prostate, penile, and testicular cancers proffered paper session. Dr. Paul Nguyen presented ENZARAD (ANZUP 1303), a randomized phase II trial of ADT + radiation therapy +/- enzalutamide for high-risk, clinically localized prostate cancer.
ENZARAD (ANZUP 1303) is an international phase III investigator-initiated trial that aims to determine whether two years of enzalutamide improves metastasis-free survival (MFS) when added to two years of LHRH agonist and high-quality radiation for patients with high risk, clinically-localized or locally-advanced prostate cancer.
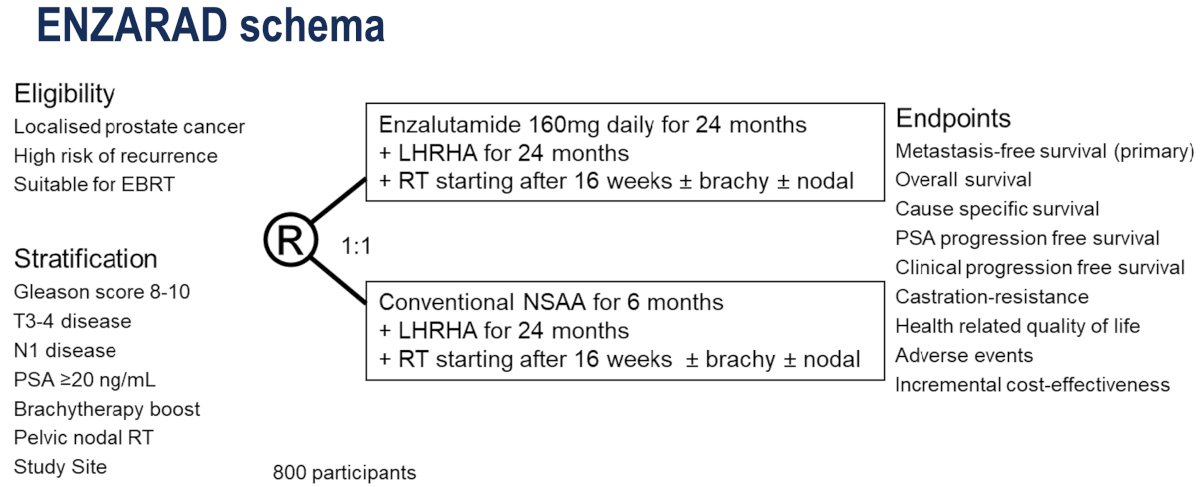
The ENZARAD study design is illustrated below. Men with high-risk, localized prostate cancer suitable for external beam radiotherapy (EBRT) were randomized to:
- Experimental arm: Enzalutamide (160 mg daily x 24 months) + LHRH agonist (24 months) + prostate EBRT +/- brachytherapy +/- nodal irradiation 16 weeks after starting hormonal therapy
- Control arm: Conventional NSAA (6 months) + LHRH agonist (24 months) + prostate EBRT +/- brachytherapy +/- nodal irradiation 16 weeks after starting hormonal therapy
The primary endpoint was metastasis-free survival (MFS), with a sample size of 800 patients having 80% power to detect a hazard ratio (HR) benefit of 0.67. The secondary endpoints were:
- Overall survival (OS)
- Of note, OS was the original primary endpoint, but this was changed to MFS due to lower rates of deaths observed than anticipated
- Cause-specific survival (CSS)
- PSA progression-free survival (PSA PFS)
- Clinical progression-free survival
- Castration resistance
- Health related quality of life (HRQoL)
- Adverse events
- Incremental cost-effectiveness
The key statistical considerations were as follows:
- Main effects were tested with unstratified log-rank tests (alpha=0.05).
- HRs & 95% CI were calculated using Cox proportional hazards models
- All p-values were 2-sided and nominal without adjustment for multiple comparisons
- Five subgroups of interest were prespecified and tested with interaction p-values.
The radiation details and quality assurances were as follows:
- Prostate treated with modern, high dose regimens: 78Gy or to 46Gy plus brachy boost
- Pelvic nodal radiotherapy
- Required for cN1 (46Gy elective nodes + boost to gross nodes)
- Optional for cN0; had to be declared prior to randomization
- Intensive radiation quality assurances were performed:
- Credentialing
- Benchmarking exercise
- Real-time QA of first 5 patient plans at each site
- Random sampling of 20% of the patients thereafter for real-time QA
Overall, 802 participants were recruited from 8 countries between March 2014 and June 2018. The median follow-up was 8 years.
The baseline patient characteristics are summarized below. Notably, 12% of patients had cN1 disease by conventional imaging, 90% had Gleason Score 8-10 disease, and 36% had a serum PSA level >20 ng/ml. 40% were planned for pelvic radiotherapy, and 8% were planned for a brachytherapy boost.
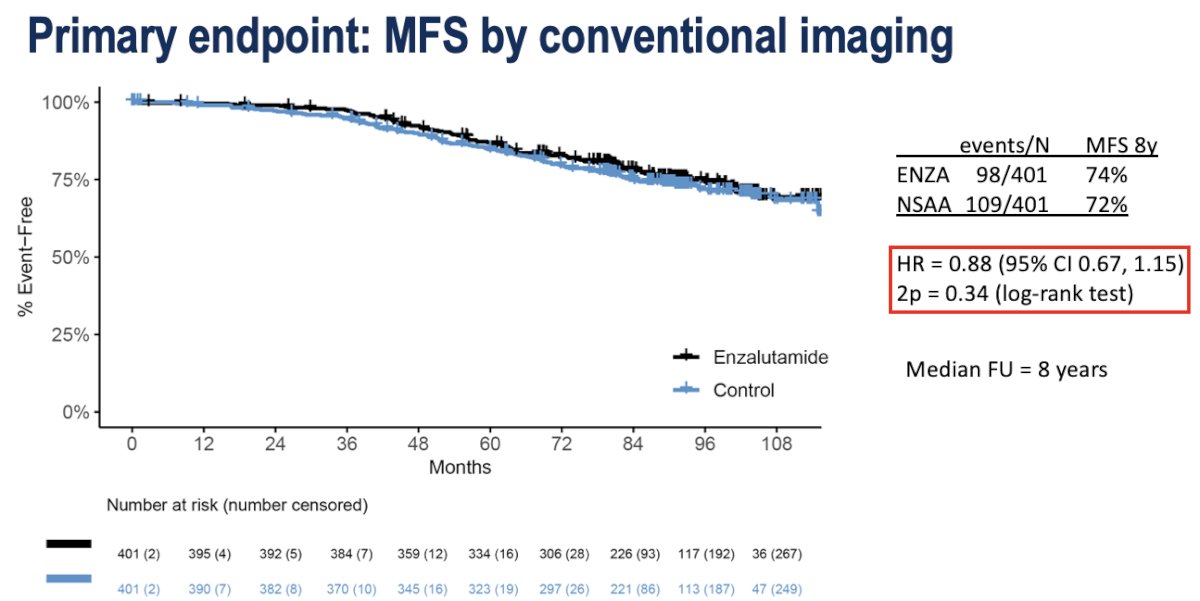
The study failed to meet its primary endpoint of an MFS benefit (8-year: 74% versus 72%; HR: 0.88, 95% CI: 0.67–1.15, p=0.34).
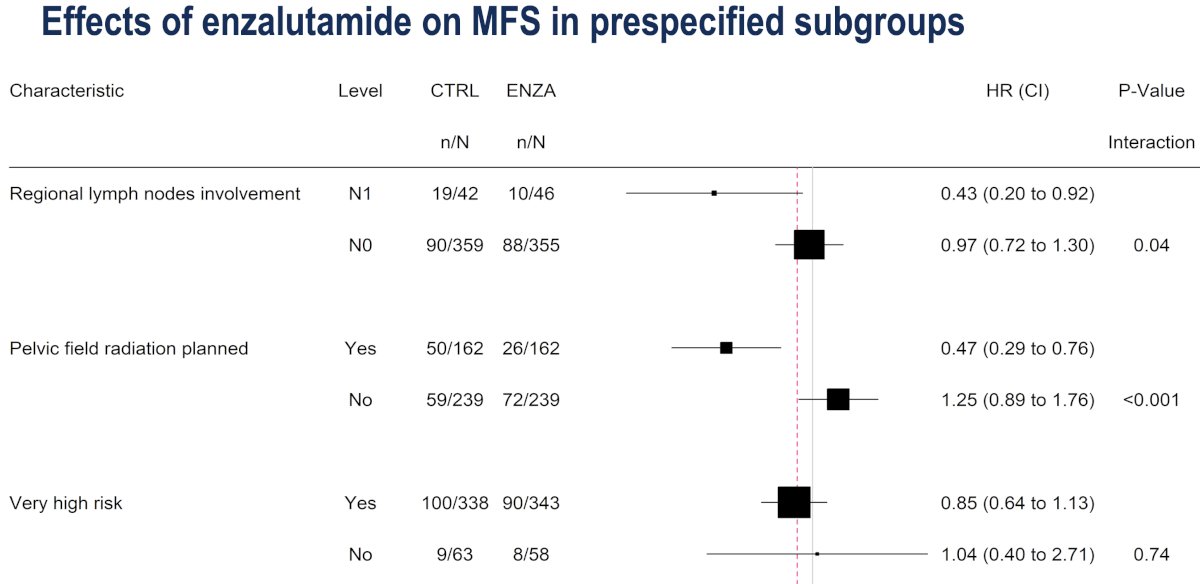
Subgroup analyses demonstrated that a significant MFS benefit may be observed in patients with:
- Regional lymph node involvement (cN1): HR=0.43, 95% CI: 0.20–0.92
- Pelvic field radiation planned: HR=0.47, 95% CI: 0.29–0.76
- No benefit in ‘very high-risk’ disease: HR=0.85, 95% CI: 0.64–1.13
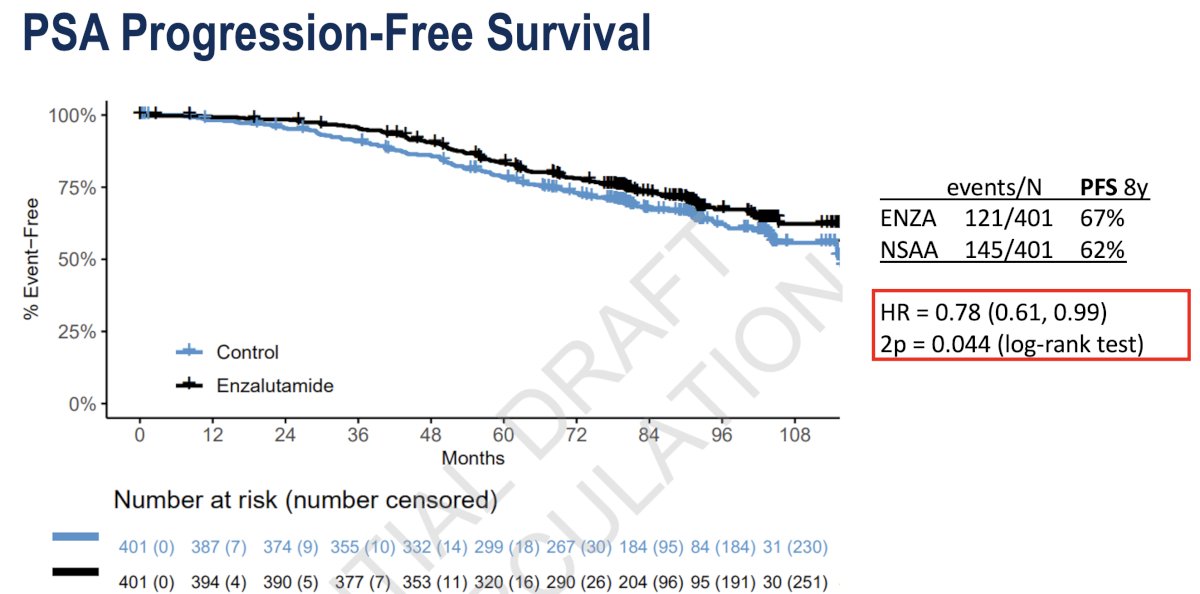
A significant PFS benefit was observed in favor of enzalutamide (8-year: 67% versus 62%; HR: 0.78, 95% CI: 0.61–0.99, p=0.044):
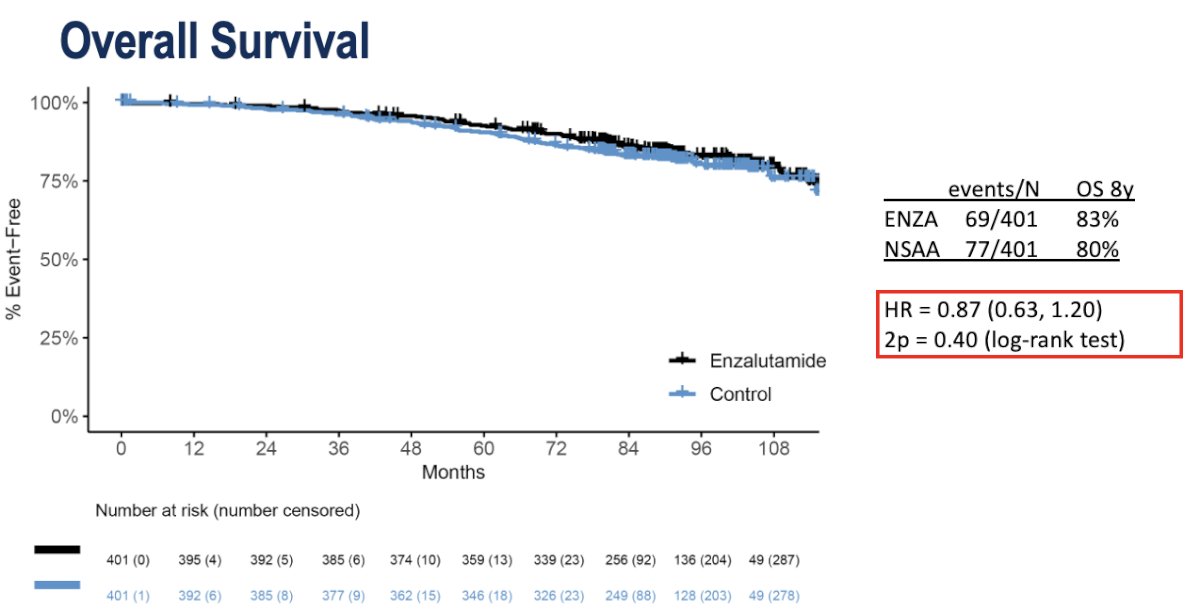
No significant difference in OS was observed (8-year: 83% versus 80%; HR: 0.87, 95% CI: 0.63–1.20, p=0.40).
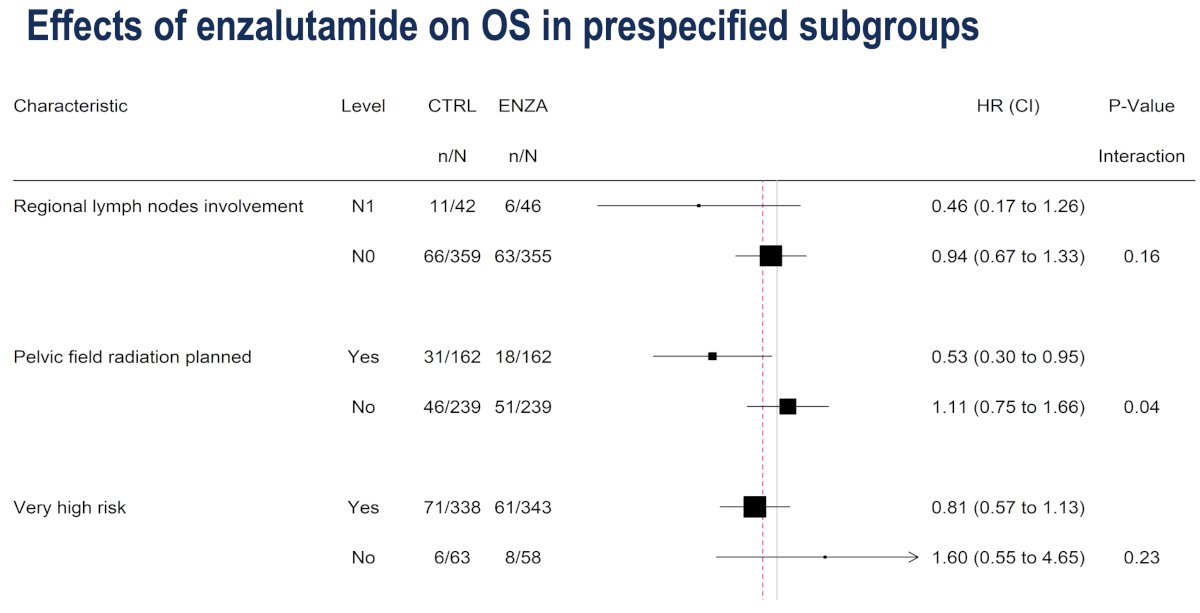
However, on OS subgroup analyses, similar to what was observed with MFS, a potential OS benefit was observed in patients with:
- Regional lymph node involvement (cN1): HR=0.46, 95% CI: 0.17-1.26
- Pelvic field radiation planned: HR=0.53, 95% CI: 0.30–0.95
- No benefit in ‘very high-risk’ disease: HR=0.81, 95% CI: 0.57–1.13
- Of note, the HRs for OS mirrored those of MFS on subgroup analyses, as predicted by ICECaP surrogacy
- No benefit in ‘very high-risk’ disease: HR=0.81, 95% CI: 0.57–1.13
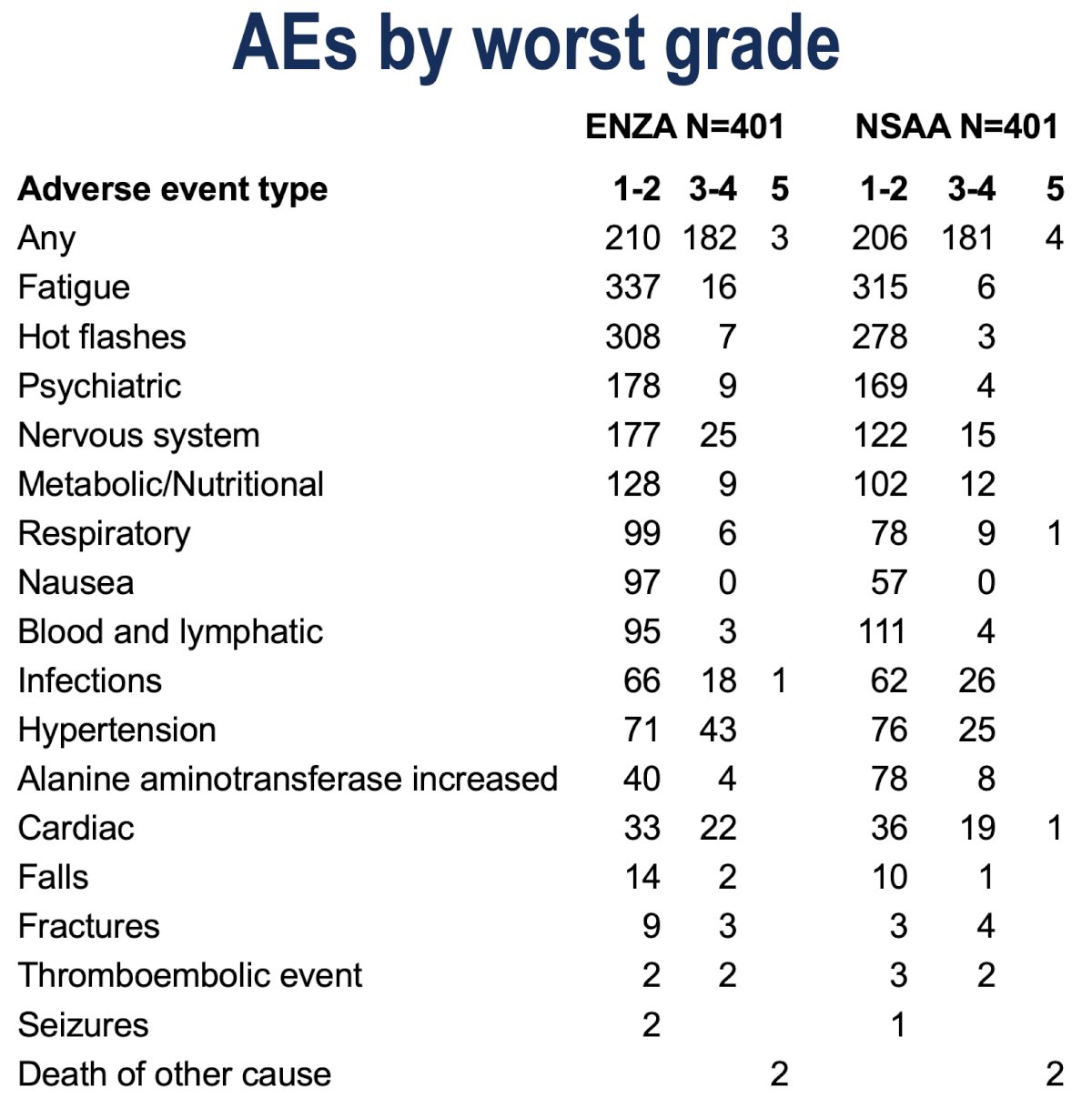
Dr. Nguyen highlighted key adverse events as follows:
What are the implications for practice?
- Most patients with clinically-localized or locally-advanced prostate cancer receiving high-quality radiation and 2 years of ADT do not need enzalutamide
- For patients with positive nodes on CT or other indications for pelvic radiation, ENZARAD provides good evidence of a benefit to enzalutamide
What are the future directions in this space?
- A deeper dive is needed to better understand which patient subgroups receiving pelvic radiotherapy ‘drive’ the benefit of enzalutamide
- There is potential for a meta-analysis with other ARPI trials to identify patients who may benefit most from intensification (e.g. STAMPEDE, ATLAS, DASL-HiCaP, NRG GU-009/PREDICT-RT)
- Biomarkers to identify which patients require intensification need to be evaluated in translational studies
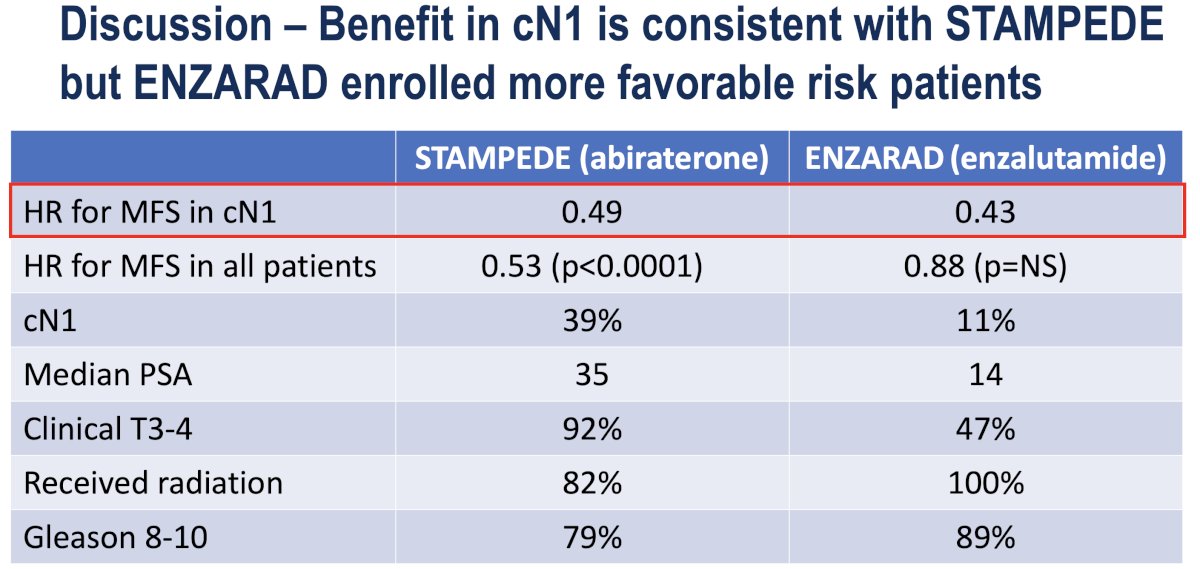
Contextualizing these results within the paradigm of existing studies, Dr. Nguyen noted that the MFS benefit of enzalutamide in ENZARAD patients with cN1 disease mirrors that observed in the STAMPEDE abiraterone patients.1 However, the HR for MFS in all patients was significantly weaker in the ENZARAD trial (0.88 versus 0.53), which may reflect the more favorable risk profile of the ENZARAD patients:
- cN1
- STAMPEDE: 39%
- ENZARAD: 11%
- PSA, median
- STAMPEDE: 35 ng/ml
- ENZARAD: 14 ng/ml
- cT3-4
- STAMPEDE: 92%
- ENZARAD: 47%
Why does enzalutamide benefit patients receiving pelvic radiotherapy? Possible explanations include:
- Higher risk patients got selected for pelvic RT and may benefit more from enzalutamide
- Pelvic RT group: 28% N1, 62% Gleason 9/10
- No Pelvic RT group: 0% N1, 49% Gleason 9/10
- Perhaps sterilizing the pelvic nodes with radiation is necessary to observe a benefit of enzalutamide on distant metastases
- 1 & 2 may both be true
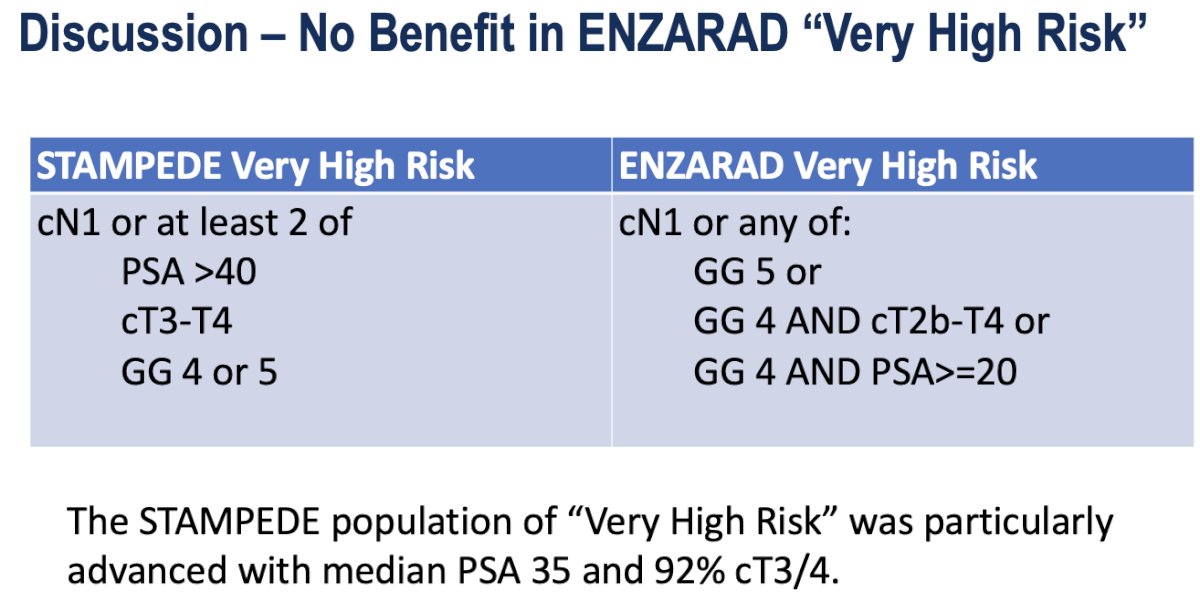
Dr. Nguyen next discussed why no benefit was observed with enzalutamide in the ENZARAD ‘very high risk’ cohort:
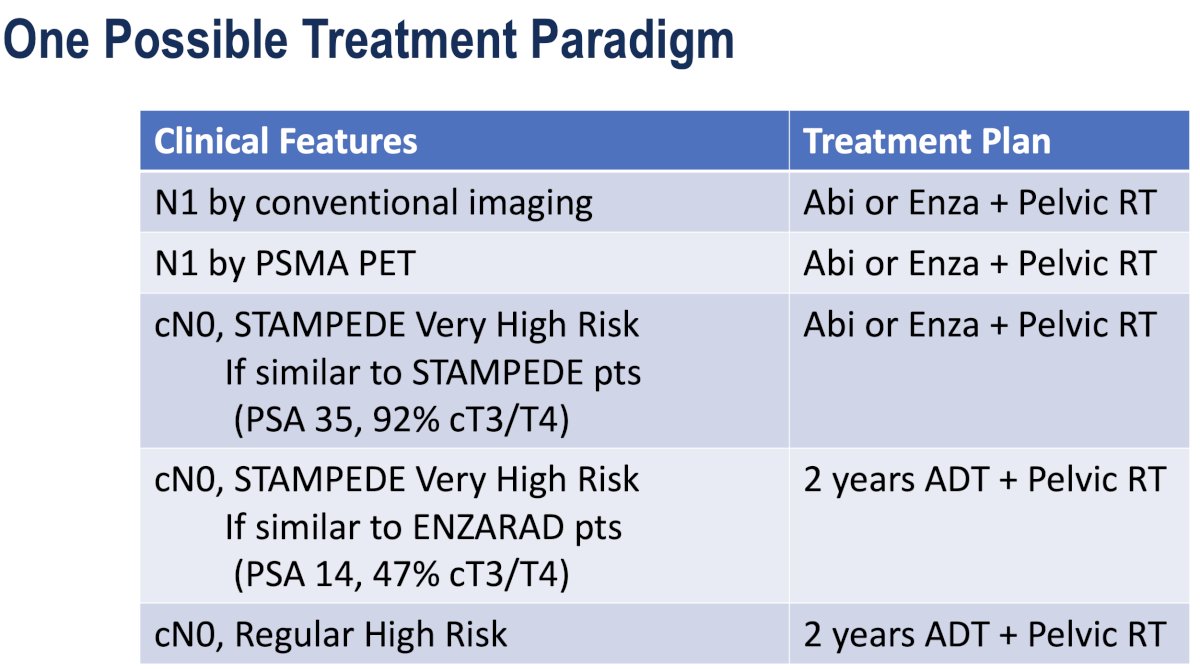
Based on the existing literature, incorporating the results of both the STAMPEDE and ENZARAD trials, Dr. Nguyen proposed the following treatment paradigm:
Dr. Nguyen concluded his presentation with the following key take home messages:
- ENZARAD showed an overall limited effect of enzalutamide versus an active NSAA control on metastasis-free survival in high risk, localized prostate cancer
- Two preplanned subgroups (clinical N1 and patients who received pelvic RT) showed evidence of benefit
Presented by: Paul L. Nguyen, MD, MBA, Professor, Director of Genitourinary Radiation Oncology, Harvard Medical School, Dana-Farber Cancer Institute, Boston, MA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: The Phase III ENZARAD Trial: Enzalutamide with Radiation and ADT in High-Risk Prostate Cancer - Paul Nguyen
Optimizing Advanced Prostate Cancer Care: Balancing Intensification and Overtreatment - Gerhardt Attard
References: