(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between September 17th and 21st was host to the session Proffered Paper Session: Radioligand Therapeutics. Dr. Jeremie Calais presented the LBA90: 177Lutetium-PSMA Therapy Neoadjuvant to Stereotactic Ablative Radiotherapy for Recurrent Oligo-Metastatic Hormone Sensitive Prostate Cancer: a Randomized Phase 2 trial (LUNAR)
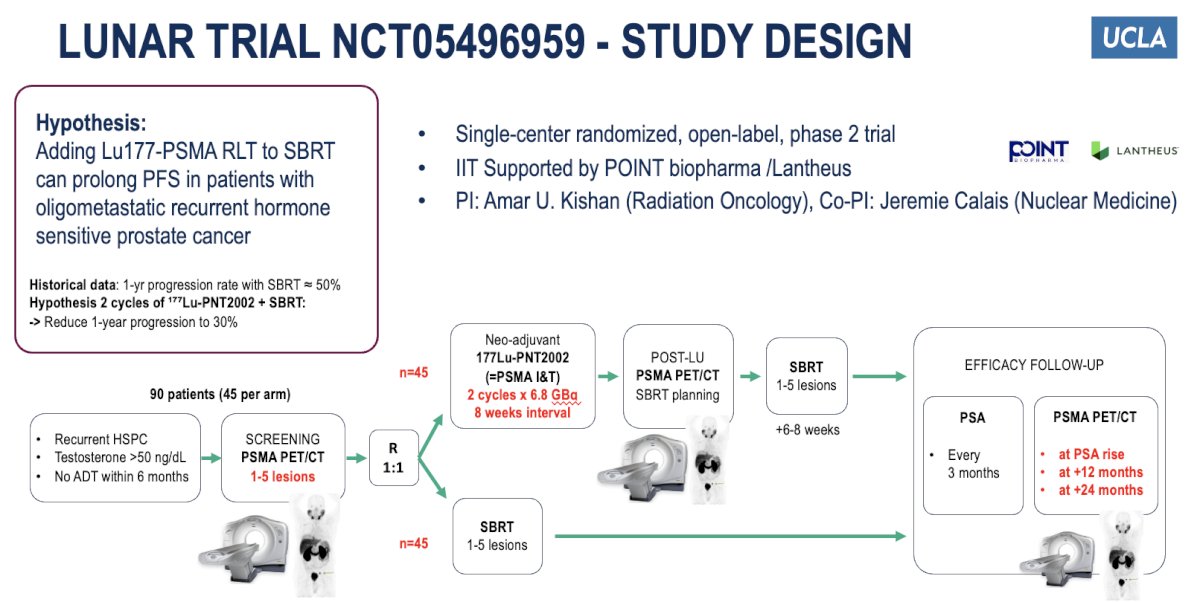
Dr. Calais began by outlining LUNAR, a phase 2 trial (NCT05496959), a single-center, open-label, randomized study evaluating whether adding 177Lu-PSMA RLT (Lu-PNT2002) to SBRT can prolong PFS in patients with oligometastatic, recurrent hormone-sensitive prostate cancer. Ninety patients with 1–5 PSMA PET–positive lesions are randomized 1:1 to receive either SBRT alone or two cycles of 177Lu-PNT2002 (6.8 GBq every 8 weeks) followed by SBRT. The trial aims to reduce the 1-year progression rate from 50% to 30%. Follow-up includes PSA assessments every 3 months and PSMA PET/CT at PSA rise, 12, and 24 months. The trial planned to accrue 90 patients (45 per arm) over 18 months with 36 months of follow-up, providing 80% power at α=0.1, and accounted for a 10% dropout rate for a total enrollment goal of 100 patients. The study design is shown below.
Dr. Calais outlined that the primary endpoint of the LUNAR trial is progression-free survival (PFS), defined as the time from randomization until PSMA PET/CT-based progression, initiation of salvage hormonal therapy, or death. PET/CT progression includes new lesions, local progression with more than 30% increase in SUV, or more than 20% increase in target lesion size. Secondary endpoints include CTCAE-graded toxicity, hormonal therapy-free survival, dosimetry of organs and tumors, overall survival, and local control. Follow-up imaging is performed at 12 and 24 months post-SBRT or at the time of PSA rise defined as either an increase of ≥0.2 ng/mL for patients with a pre-enrollment PSA <0.5 ng/mL, or a ≥50% rise above the post-SBRT nadir for those with a baseline PSA ≥0.5 ng/mL. PSMA PET/CT-based progression was defined as a new lesion on PSMA PET/CT or local progression on PSMA PET/CT as outlined below.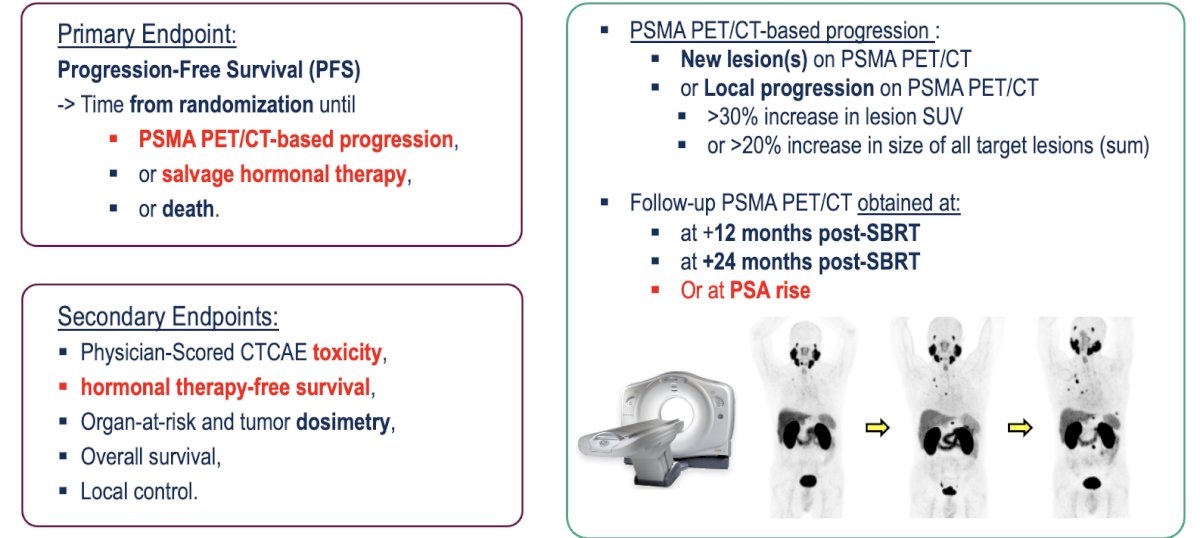
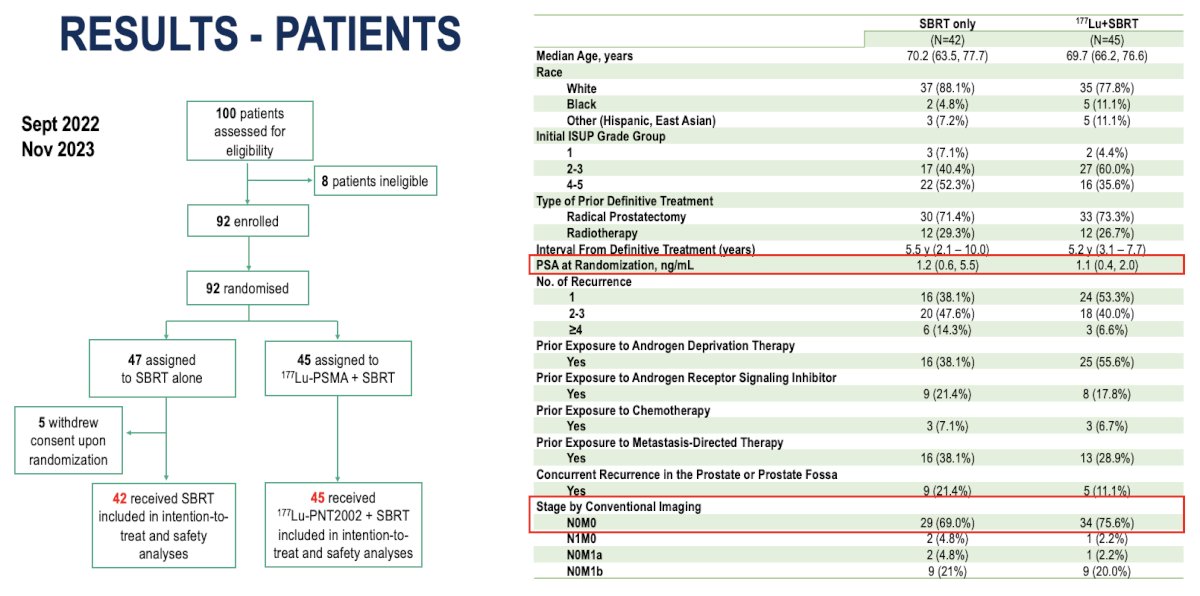
From September 2022 to November 2023, 100 patients were screened and 92 enrolled, all of whom were randomized to receive either SBRT alone (n=47) or 177Lu-PSMA plus SBRT (n=45). Five patients withdrew consent, leaving 87 for intention-to-treat and safety analyses. The median age was 70 years in the SBRT arm and 69 in the combination arm. The median PSA at randomization was 1.2 ng/mL (IQR 0.6–5.5) for SBRT and 1.1 ng/mL (IQR 0.4–2.0) for the combination group. Most patients had undergone prior radical prostatectomy, and around half had ISUP grade 4–5 disease. The majority were staged as M0 by conventional imaging as illustrated in the table below.
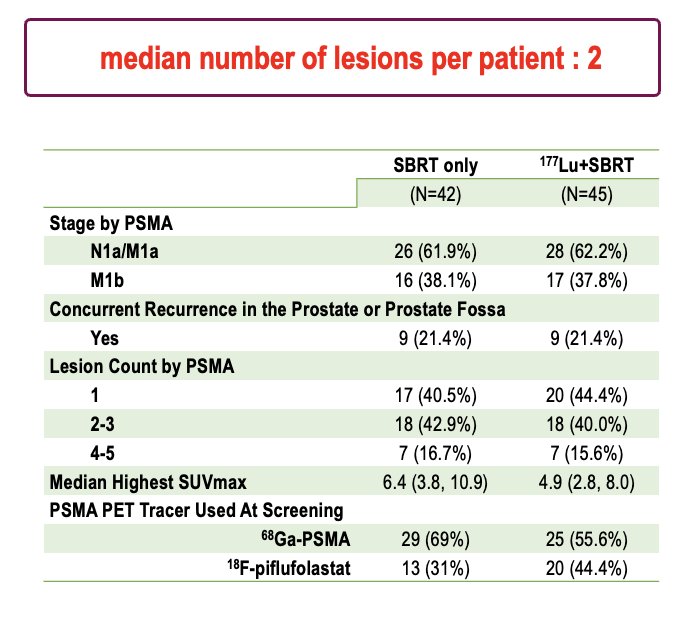
Dr. Calais highlighted that the median number of PSMA-detected lesions per patient was two. Most patients presented with N1a/M1a disease, and about 21% had concurrent local recurrence in the prostate or prostate fossa. The median highest SUVmax was 6.4 in the SBRT arm and 4.9 in the 177Lu+SBRT arm. For imaging, 68Ga-PSMA was used in the majority, while 18F-piflufolastat was utilized in roughly one-third in the SBRT group to nearly half of the patients in the experimental group.
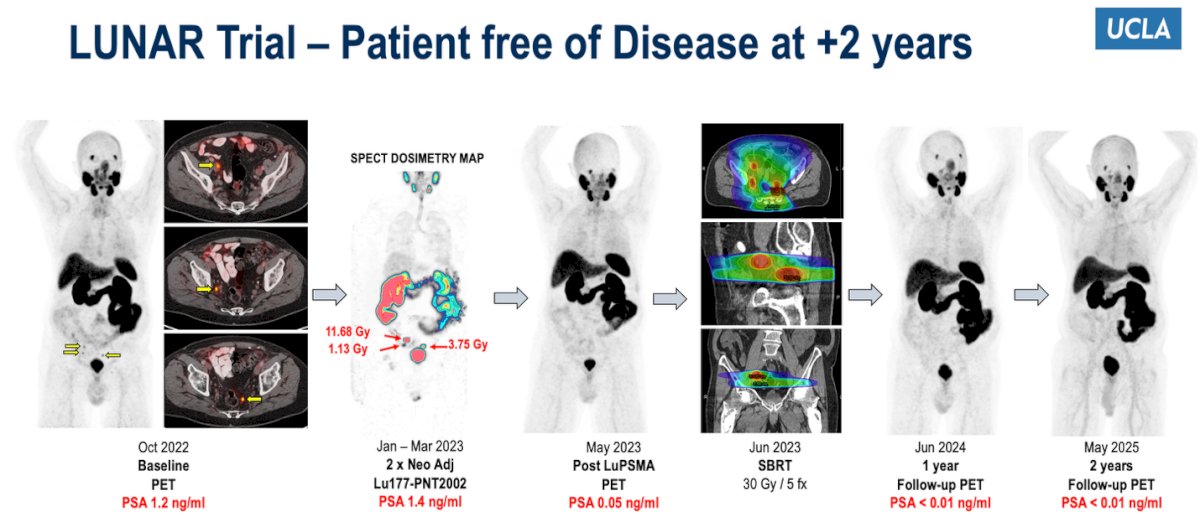
Dr. Calais presented a representative case from the LUNAR trial showing a patient with oligometastatic recurrence who achieved complete disease remission two years after treatment. The patient received two cycles of neoadjuvant 177Lu-PNT2002 followed by SBRT (30 Gy in 5 fractions), resulting in a progressive PSA decline from 1.2 ng/mL at baseline to <0.01 ng/mL at 24 months, with sustained disease-free status on serial PSMA PET/CT imaging.
Among patients receiving two neoadjuvant cycles of 177Lu-PNT2002, 71% experienced a PSA decline with a median decrease of 51.9% (IQR 26.0–78.1%), while 27% showed an increase (median +18.2%, IQR 12.1–30.1%) and one patient (2%) had no change. On interval PSMA PET scans, 16% of patients achieved at least a 30% reduction in one or more target lesions, allowing for treatment volume reduction and SBRT dose adjustment. Two patients (4%) had a complete resolution of all disease, whereas one patient (2%) developed progressive disease and did not proceed to SBRT. Overall, 44 of 45 patients (98%) successfully completed protocol-specified SBRT following 177Lu-PNT2002, with a median interval of 5.9 weeks (IQR 5.0–7.1 weeks) between the second RLT cycle and radiation therapy.
Dr. Calais highlighted that the PSA50 response rate (≥50% PSA decline from baseline) was notably higher in the experimental arm receiving 177Lu-PNT2002 plus SBRT, at 52%, compared to 31% in the SBRT-only control arm (p=0.04). Additionally, PSA increases were observed in 23% of patients treated with 177Lu-PNT2002 versus 45% in the control group, suggesting enhanced biochemical response with the addition of radioligand therapy.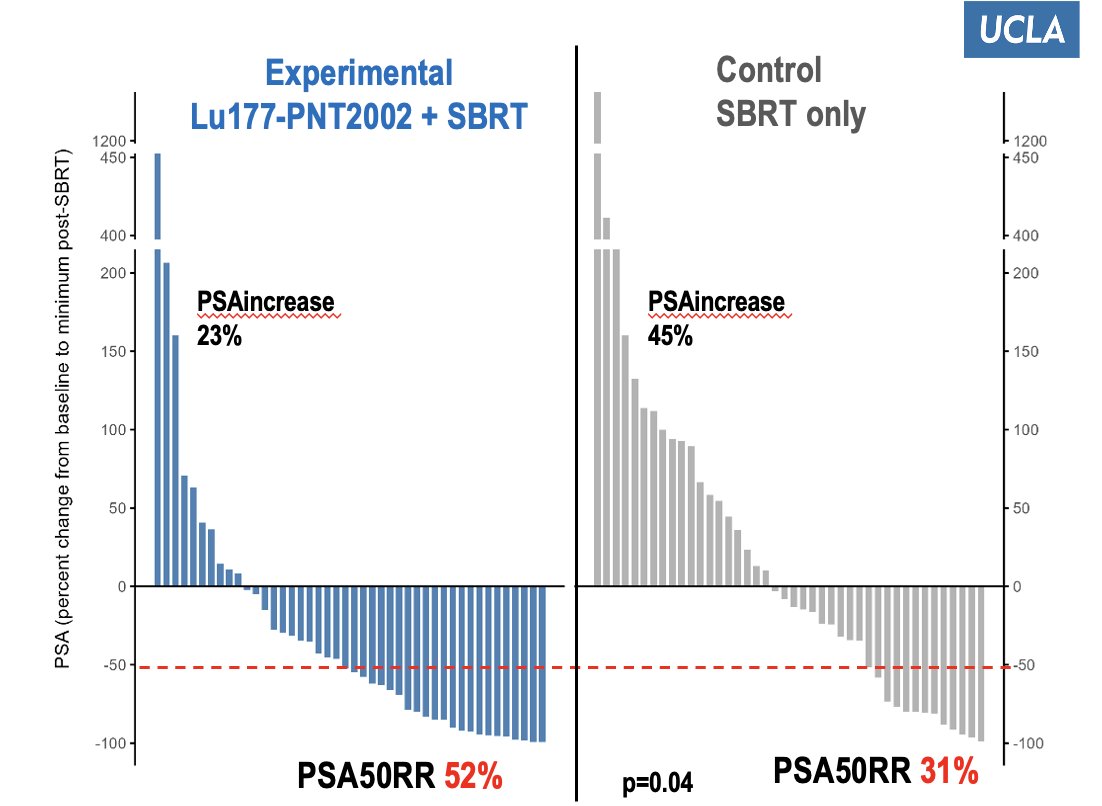
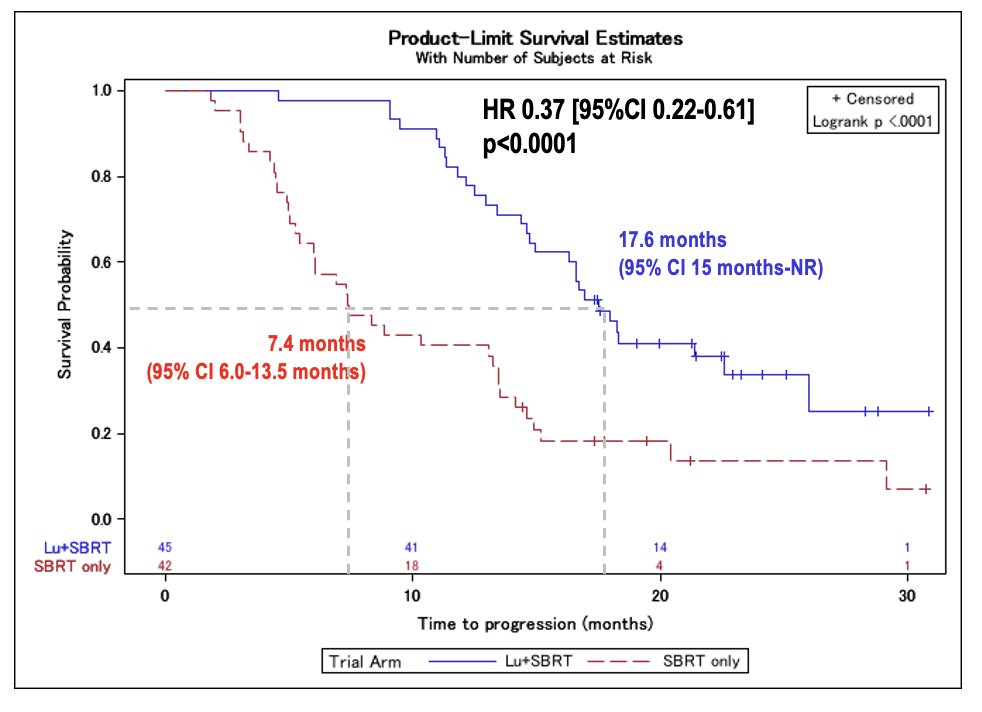
After a median follow-up of 22 months (IQR 19–26), the LUNAR trial met its primary endpoint of progression-free survival. A total of 65 progression events (75%) occurred 36 of 42 patients (86%) in the SBRT-only arm and 29 of 45 (64%) in the 77Lu-PNT2002 + SBRT arm. The addition of radioligand therapy significantly prolonged median PFS to 17.6 months (95% CI 15–NR) compared to 7.4 months (95% CI 6.0–13.5) with SBRT alone (HR 0.37, 95% CI 0.22–0.61, p<0.0001). Most progression events (98%) were due to new lesions rather than in-field recurrence; notably, only 2% of SBRT-treated lesions and none in the 177Lu-PNT2002 arm showed in-field progression, underscoring the high local control achieved with combined therapy.
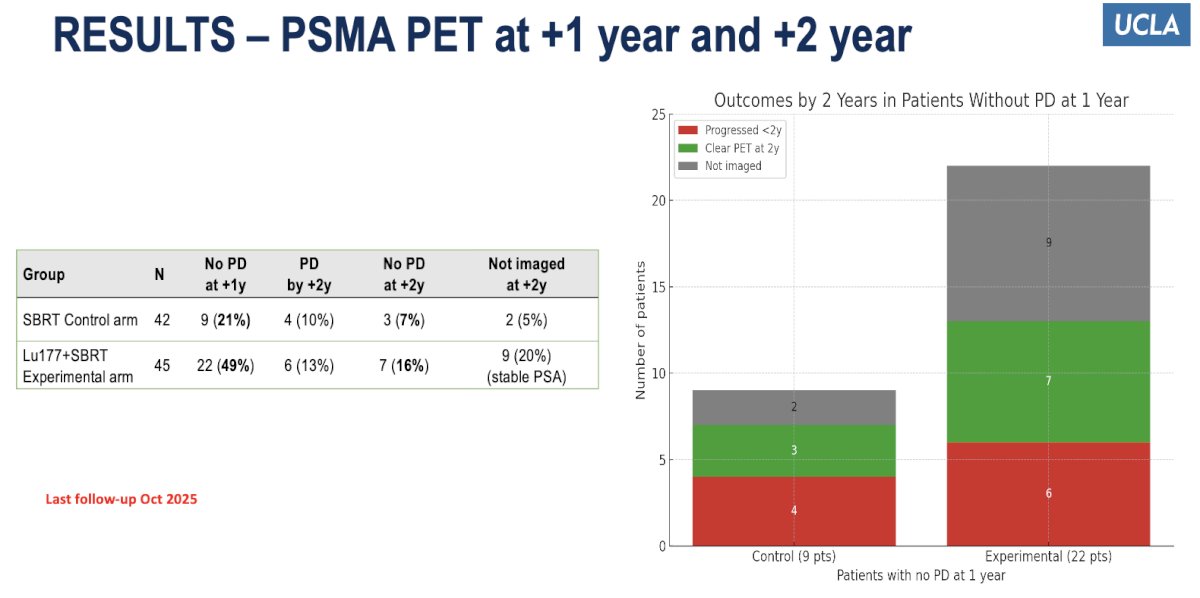
Moreover, PSMA PET assessments at one and two years demonstrated sustained disease control favoring the 177Lu-PNT2002 + SBRT arm. At one year, 49% of patients in the experimental arm showed no progression compared to 21% in the SBRT-only group. By two years, 16% of patients in the combination arm remained progression-free versus 7% in the control arm, with an additional 20% of patients in the experimental group maintaining stable PSA levels but not yet re-imaged.
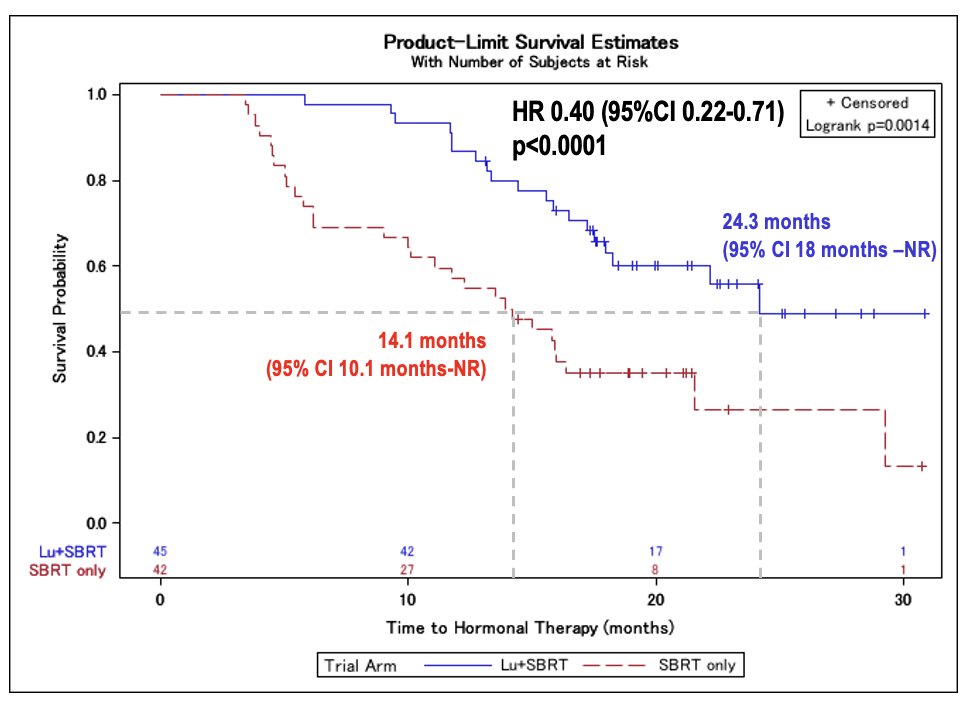
Another important endpoint was time to salvage hormonal therapy. Dr. Calais showed that the addition of 177Lu-PNT2002 to SBRT significantly delayed the need for systemic therapy. Median HT-free survival was 24.3 months (95% CI 18–NR) with 177Lu-PNT2002 + SBRT versus 14.1 months (95% CI 10.1–NR) with SBRT alone (HR 0.40, 95% CI 0.22–0.71; p=0.0014). Salvage HT was initiated in 38% of patients in the SBRT arm compared to 20% in the experimental arm. Additionally, 24% and 22% of patients, respectively, received a combination of HT and repeat SBRT, while repeat SBRT alone was performed in 19% and 20% of patients in each group.
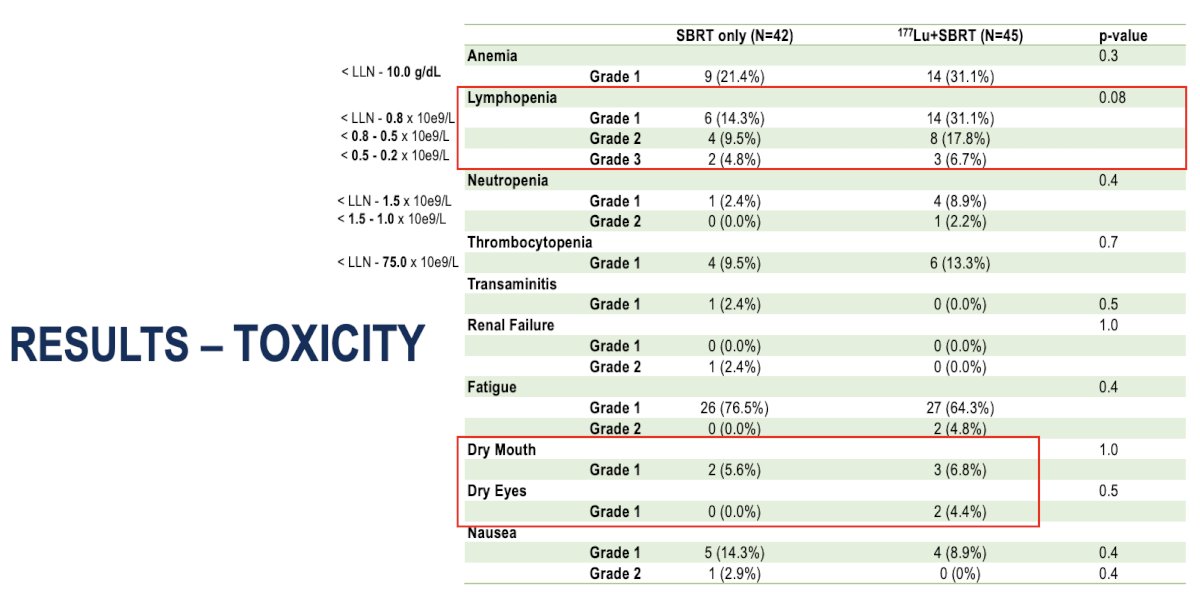
In terms of toxicity, treatment was generally well tolerated in both groups. The most common laboratory abnormality was lymphopenia, observed in 31% of patients in the 177Lu-PNT2002 + SBRT arm (including 8 grade 2 and 3 grade 3 cases) versus 14% in the SBRT-only group (p=0.08). Mild xerostomia and dry eyes were reported exclusively in the combination arm (6.8% and 4.4%, respectively), consistent with expected radioligand-related side effects. No grade ≥3 non-hematologic toxicities were observed, and the overall safety profile supported the feasibility of combining 177Lu-PNT2002 with SBRT.
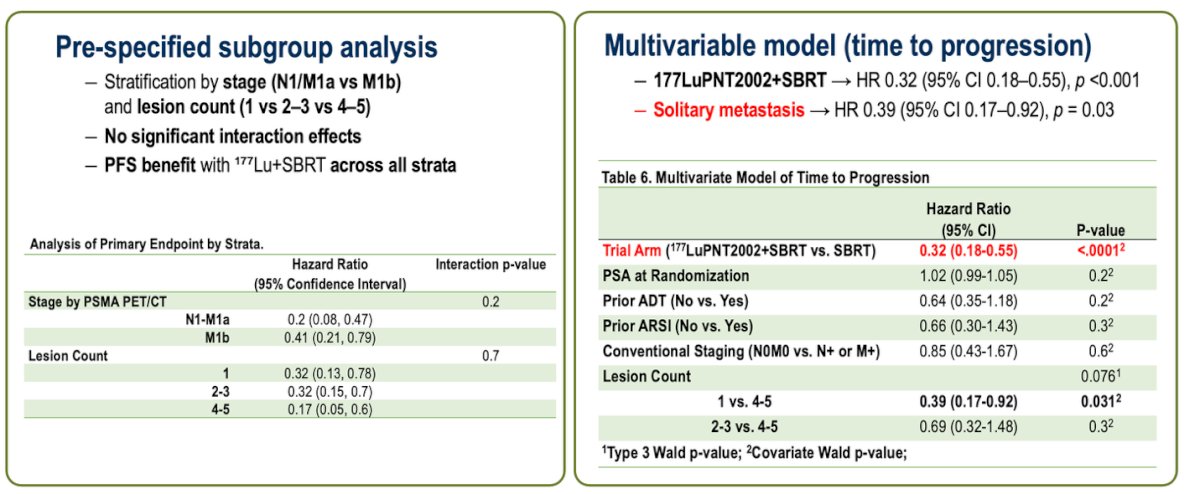
 Lastly, in a pre-specified subgroup analysis stratified by stage (N1/M1a vs M1b) and lesion count (1 vs 2–3 vs 4–5), the PFS benefit with 177Lu-PNT2002 + SBRT was consistent across all strata, with no significant interaction effects. Similarly, the multivariable model for time to progression demonstrated that treatment with 177Lu-PNT2002 + SBRT remained an independent predictor of improved outcomes (HR 0.32, 95% CI 0.18–0.55, p<0.001). Additionally, patients with solitary metastases showed a significantly lower risk of progression (HR 0.39, 95% CI 0.17–0.92, p=0.03), reinforcing the potential value of this approach in oligometastatic disease.
Lastly, in a pre-specified subgroup analysis stratified by stage (N1/M1a vs M1b) and lesion count (1 vs 2–3 vs 4–5), the PFS benefit with 177Lu-PNT2002 + SBRT was consistent across all strata, with no significant interaction effects. Similarly, the multivariable model for time to progression demonstrated that treatment with 177Lu-PNT2002 + SBRT remained an independent predictor of improved outcomes (HR 0.32, 95% CI 0.18–0.55, p<0.001). Additionally, patients with solitary metastases showed a significantly lower risk of progression (HR 0.39, 95% CI 0.17–0.92, p=0.03), reinforcing the potential value of this approach in oligometastatic disease.
Dr. Calais concluded his presentation with the following key takeaways:
- In this phase 2 randomized trial of 92 patients with oligometastatic recurrent HSPC, adding two cycles of neoadjuvant 177Lu-PNT2002 (PSMA I&T) to SBRT significantly improved PFS (based on PSA and PSMA PET).
- This combination reduced the risk of recurrence, need for ADT, or death by 63% (HR 0.37; 95% CI 0.22–0.61), with benefit consistent across all subgroups.
- No increase in toxicity was observed compared to SBRT alone.
- The benefit is likely related to the eradication of occult micrometastatic disease, though 64% of patients in the Lu177+SBRT arm still experienced progression.
- Future efforts will focus on translational correlative analyses, dosimetry optimization, and evaluating alpha emitters.
Presented by: Jeremie Calais, MD, MSc, PhD, Certified Principal Investigator, ACRIP, Associate Professor, Department of Molecular and Medical Pharmacology, Director, Theranostics Program, Director, Clinical Research Program, Ahmanson Translational Theranostics Division, David Geffen School of Medicine, University of California, Los Angeles (UCLA), Los Angeles, CA
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.