(UroToday.com) The 2025 ESMO annual meeting featured a prostate cancer session and a presentation by Dr. Shahneen K. Sandhu discussing LuPARP, a phase 1 trial of 177Lu-PSMA-617 and olaparib in patients with metastatic castration resistant prostate cancer (mCRPC). 177Lu-PSMA-617 improved radiological progression free survival (median 8.7 months) and overall survival (median 15.3 months) for mCRPC in the VISION trial.1 However, approximately a third have primary resistance, and all patients inevitably relapse. 177Lu-PSMA-617 primarily causes DNA single strand breaks, which can be repaired by PARP-dependent base excision repair. Blocking PARP could result in the conversion of DNA single strand breaks to lethal double strand breaks, potentially radiosensitizing cells exposed to radioligand therapy. Preclinical studies support using potent PARP inhibitors, such as olaparib, as a radiosensitizer to enhance radioligand therapy activity. Thus, LuPARP evaluated the safety and preliminary efficacy of 177Lu-PSMA-617 with olaparib.
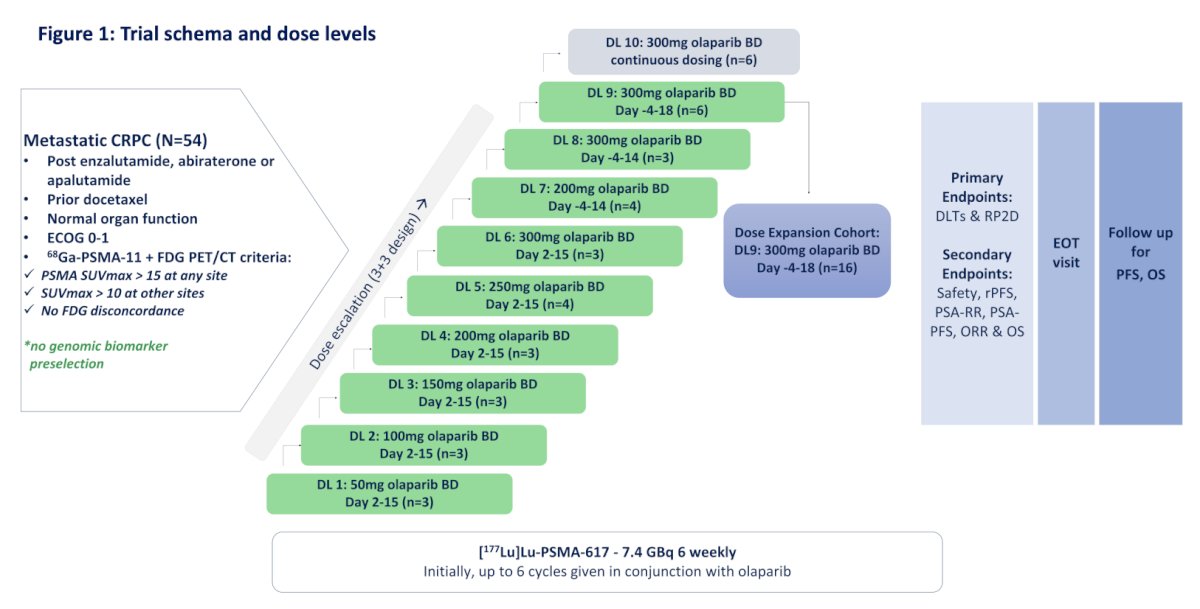
LuPARP is an investigator initiated phase 1 trial utilizing a 3+3 design for dose escalation followed by dose expansion. Between September 2019 and August 2024, 54 patients were enrolled across 2 Australian sites. Patients with mCRPC with high PSMA expression (SUVmax ≥15) without discordant FDG+ /PSMA- sites were enrolled. All patients received 177Lu-PSMA-617 7.4 GBq every 6 weeks for up to 6 cycles. Olaparib was dosed across 10 dose levels:
- Dose level 1-6: 50 mg – 300 mg BD days 2 to 15
- Dose level 7: 200 mg BD days -4 to 14
- Dose level 8: 300 mg BD days -4 to 14
- Dose level 9: 300mg BD days -4 to 18
- Dose level 10: 300 mg BD, days -4 to day 42
Primary endpoints were safety and dose limiting toxicity. Key secondary endpoints were radiological progression free survival, PSA response rate, PSA progression free survival, objective response rate, and overall survival:
Patients who achieved a deep response by PSA and based on loss of PSMA target were allowed to suspend treatment and recommence at the time of disease progression. In March 2024, an amendment permitted retreatment with 2-3 doses of 177Lu-PSMA-617 in conjunction with olaparib if a patient achieved a deep response and subsequently progressed.
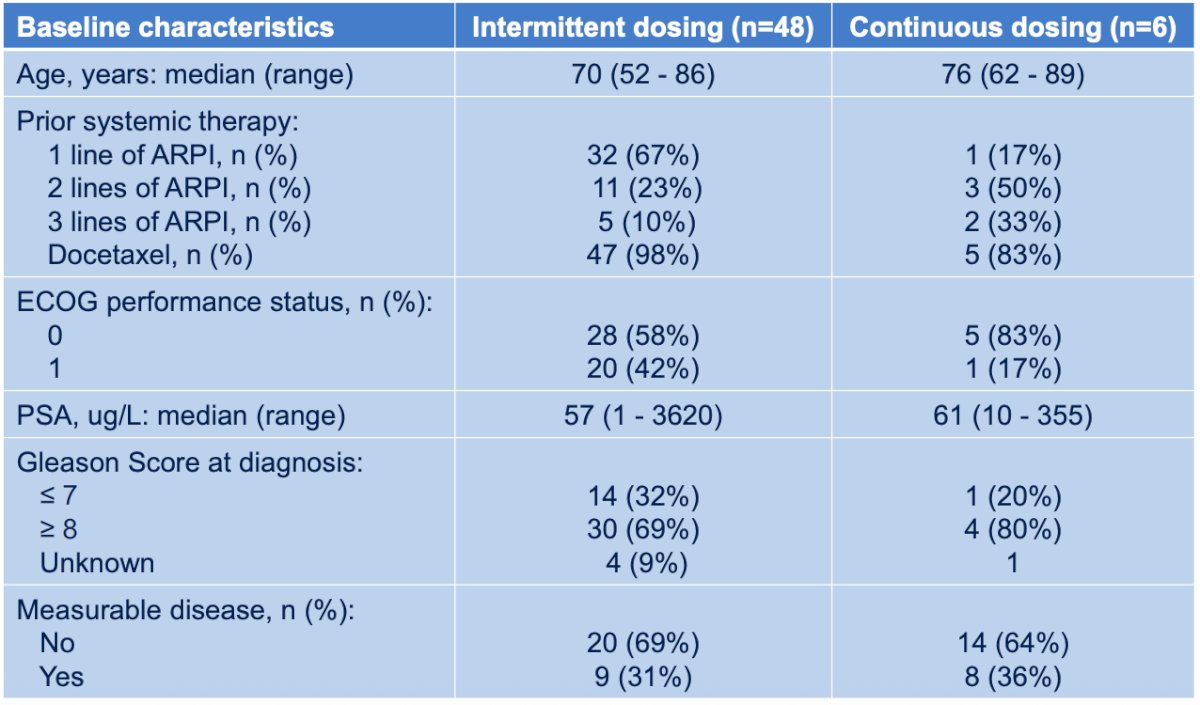
The baseline characteristics of intermittent and continuous dosing cohorts are highlighted in the following table:
The response for the intermittent cohort was grouped according to Day -4 (29 patients for DL7, DL8, and DL9) and DL9 expansion (22 patients):
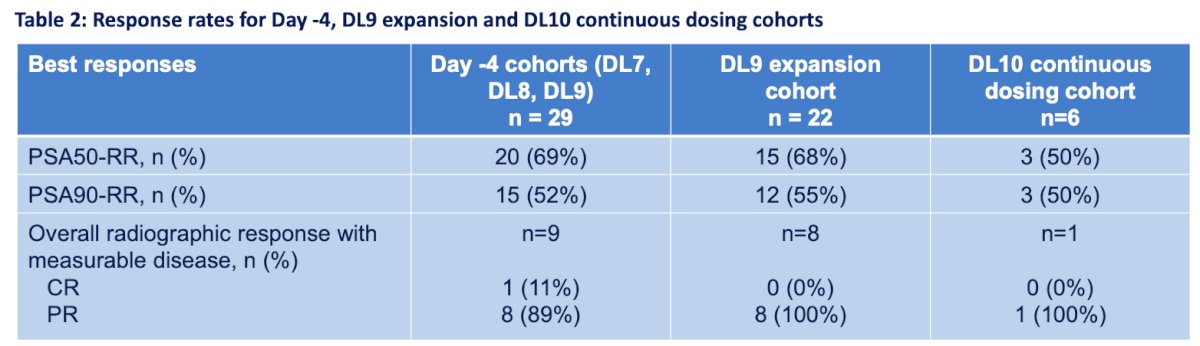
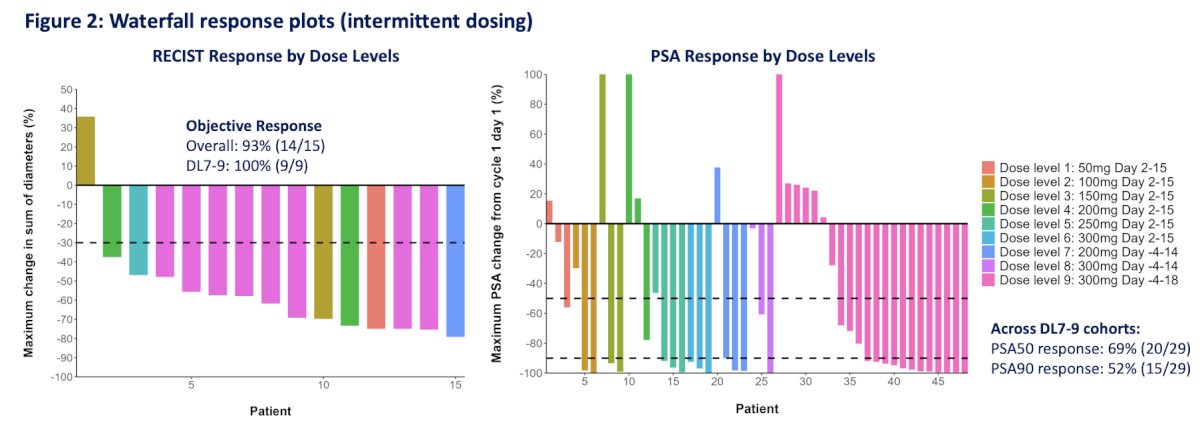
This grouping reflects the cohorts where olaparib was at Cmax when Lu-PSMA-617 was administered. In the Day -4 and the DL9 cohorts, 52% and 55% achieved ≥ 90% reduction in PSA levels, and all patients with measurable disease achieved an objective response:
The Swimmer plot of treatment duration, responses, and events (intermittent dosing) is as follows:
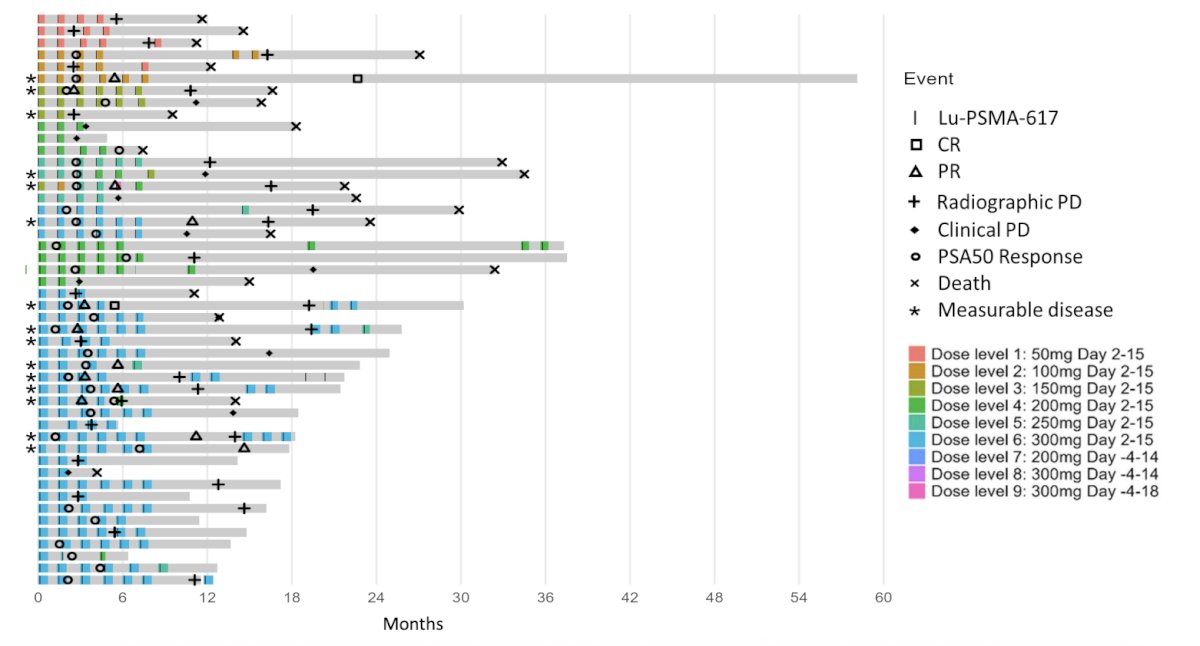
DL10 was deemed not tenable due to the early and higher rates of myelosuppression, which resulted in significant delays to subsequent Lu-PSMA-617 administration and dose reductions. Therefore, DL9 was determined to be the recommended phase 2 dose.
Treatment related adverse events for the DL9 expansion cohort, the DL10 continuous dosing cohort, and overall population are listed in the following table:
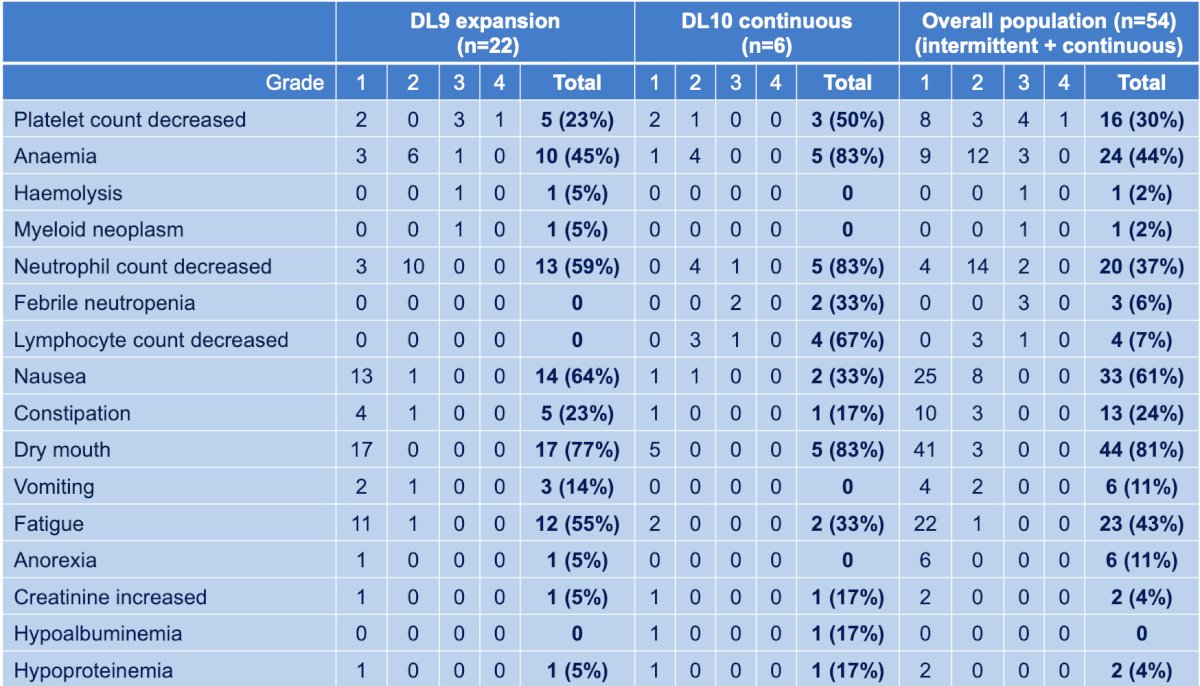
The most common treatment related adverse events of any grade included dry mouth (81%), nausea (61%), anemia (44%), fatigue (43%), neutropenia (37%), thrombocytopenia (30%). Eight patients (15%) had a grade 3 or 4 treatment related adverse events, with one patient experiencing grade 4 thrombocytopenia (2%). One patient (in DL9) has a diagnosis of treatment related myelodysplastic syndrome 20 months post commencing Lu-PSMA-617 and olaparib.
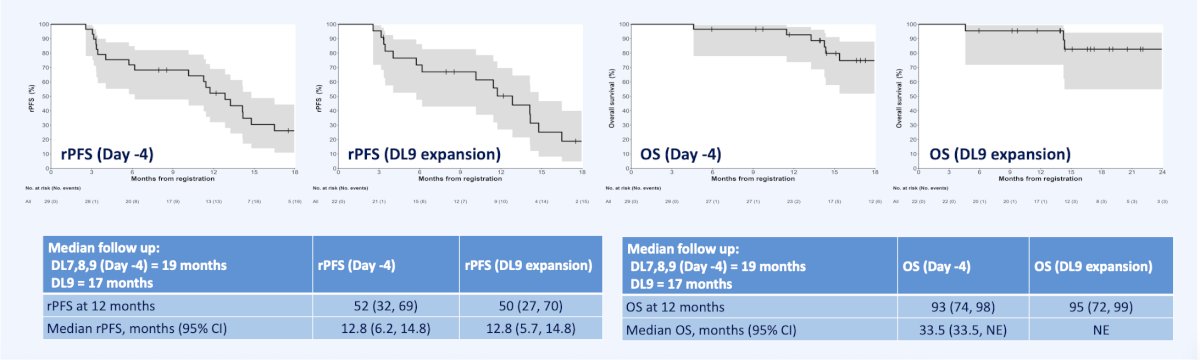
The following figure demonstrates radiographic progression free survival, and overall survival in Day – 4 and DL9 expansion:
Dr. Sandhu concluded her presentation discussing LuPARP with the following take home points:
- LuPARP is the first trial to evaluate the combination of a PARP inhibitor with Lu-PSMA-617
- With a median follow-up of 19 months, intermittent dosing of olaparib (Day −4 cohorts) in combination with Lu-PSMA-617 demonstrated promising antitumor activity in men with mCRPC, with toxicities as expected, mainly given the biodistribution of Lu-PSMA-617
- The recommended phase II dose (DL9) was established as olaparib 300 mg administered on Days −4 to 18 together with Lu-PSMA-617 7.4 GBq every 6 weeks for up to six cycles. At this dose level, the median radiographic progression free survival was 12.8 months, median overall survival was not yet estimable, and the PSA90 response rate was 55%, while toxicities were manageable
- Across the Day-4 cohorts (DL7, DL8, DL9), the median overall survival reached 33.5 months, which compares favorably with that in the VISION trial
- Continuous daily dosing of olaparib was associated with higher rates of myelosuppression, supporting the intermittent-dosing strategy for further evaluation in a phase 2 setting
Presented by: Shahneen K. Sandhu, Peter MacCallum Cancer Centre, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.