(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st was host to the session Mini oral session: GU tumours, prostate, penile and testis. Dr. Dana E. Rathkopf presented the Late-breaking abstract 91 - Patient-reported outcomes (PROs) from AMPLITUDE, a randomized placebo-controlled phase 3 trial of niraparib (NIRA) and abiraterone acetate (AA) plus prednisone (P) in metastatic hormone-sensitive prostate cancer (mHSPC) with homologous recombination repair mutations.
Dr. Rathkopf began by presenting the AMPLITUDE trial, a randomized, double-blind, placebo-controlled phase III study evaluating niraparib in combination with abiraterone acetate (AA) and prednisone plus androgen deprivation therapy (ADT) in men with metastatic hormone-sensitive prostate cancer (mHSPC) harboring homologous recombination repair mutations (HRRm).1 The AMPLTIUDE study design is shown below.
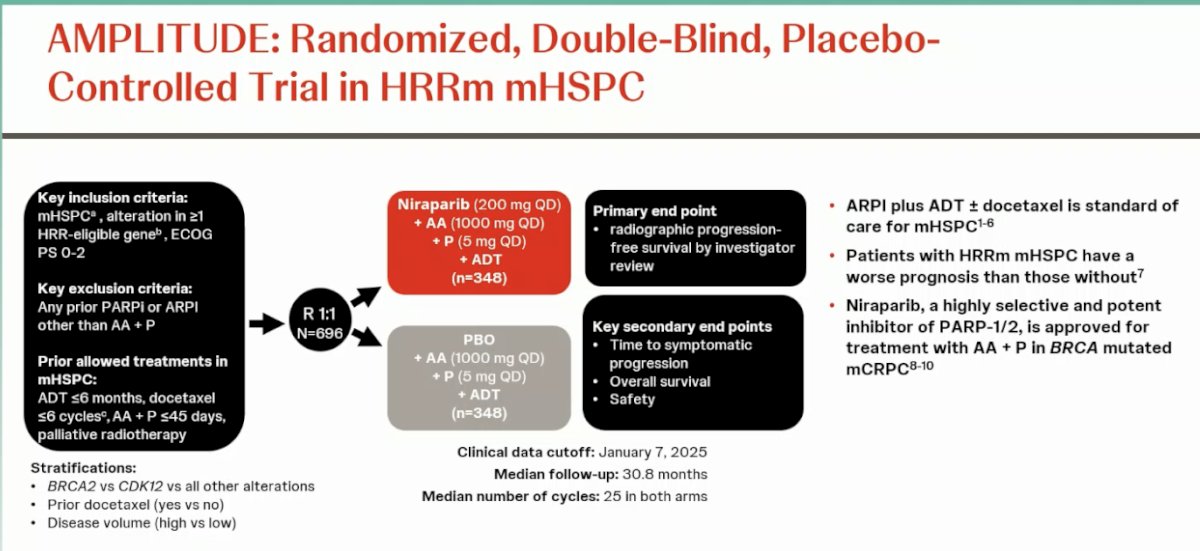
ARPI plus ADT ± docetaxel remains the standard of care for mHSPC, yet patients with HRRm experience worse outcomes compared to those without. Niraparib, a potent and selective PARP-1/2 inhibitor, is already approved for use in combination with AA + P in BRCA-mutated mCRPC, forming the rationale for its investigation in the hormone-sensitive setting.2
The AMPLITUDE study, recently published, investigated niraparib in combination with abiraterone acetate and prednisone versus placebo with abiraterone acetate and prednisone in patients with homologous recombination repair–mutated metastatic hormone-sensitive prostate cancer and successfully met its primary endpoint of radiographic progression-free survival. Treatment with niraparib significantly reduced the risk of radiographic progression or death by 37% (HR 0.63; p=0.0001) and halved the time to symptomatic progression (HR 0.50; p<0.0001). The safety profile was consistent with previous studies, with no new safety signals observed.1
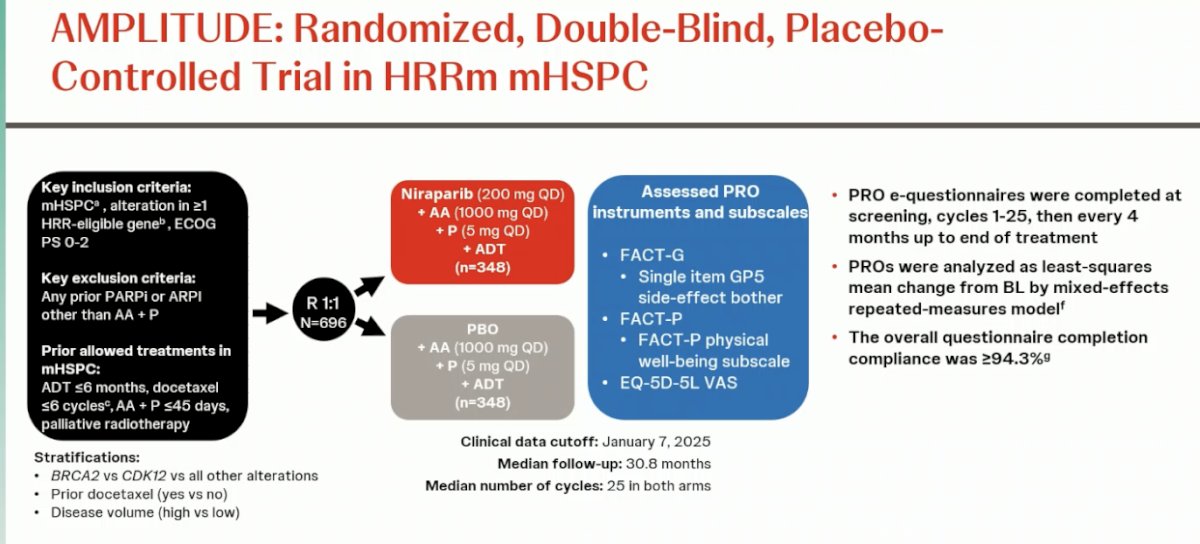
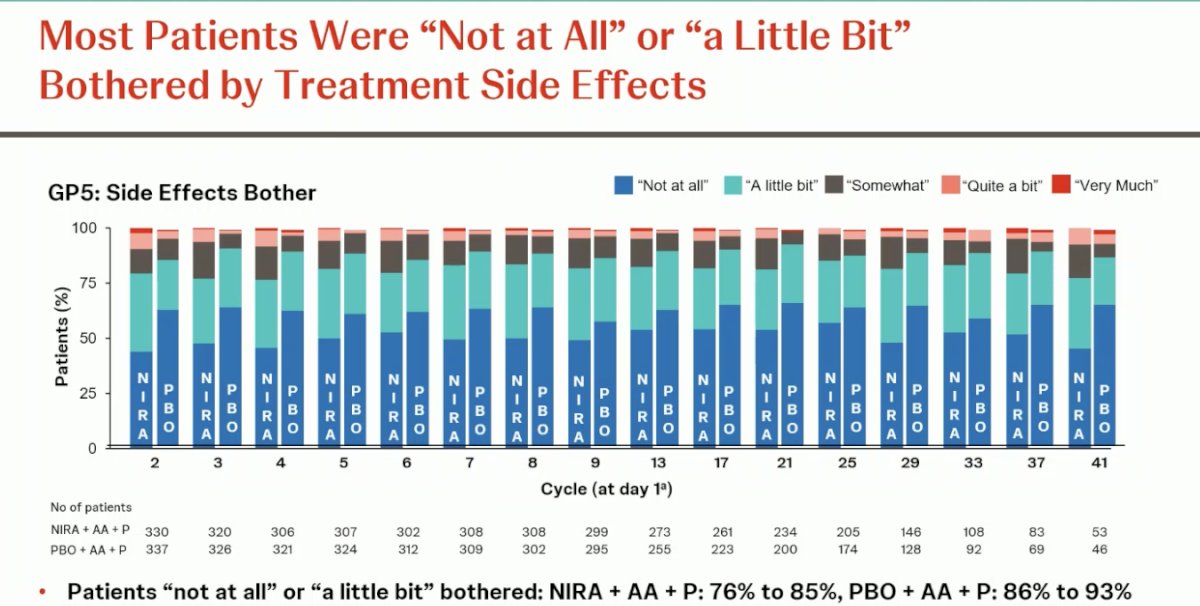
For patient-reported outcomes, instruments used in the AMPLITUDE trial included the Functional Assessment of Cancer Therapy–General (FACT-G), the single-item GP5 side-effect bother question, the Functional Assessment of Cancer Therapy–Prostate (FACT-P), its physical well-being subscale, and the EQ-5D-5L visual analog scale. Electronic questionnaires were completed at screening, during cycles 1–25, and every 4 months thereafter until treatment completion. Outcomes were analyzed using a mixed-effects repeated-measures model, with least-squares mean change from baseline. Overall questionnaire completion compliance was 94.3%.
The mean baseline FACT-G score was similar between groups, approximately 80 in both arms. An initial reduction in health-related quality of life was observed during the first four cycles, likely related to common adverse events such as hypertension and anemia. Over time, FACT-G scores were maintained and remained comparable between the niraparib and placebo groups, with only slight separation of the curves toward the end of treatment.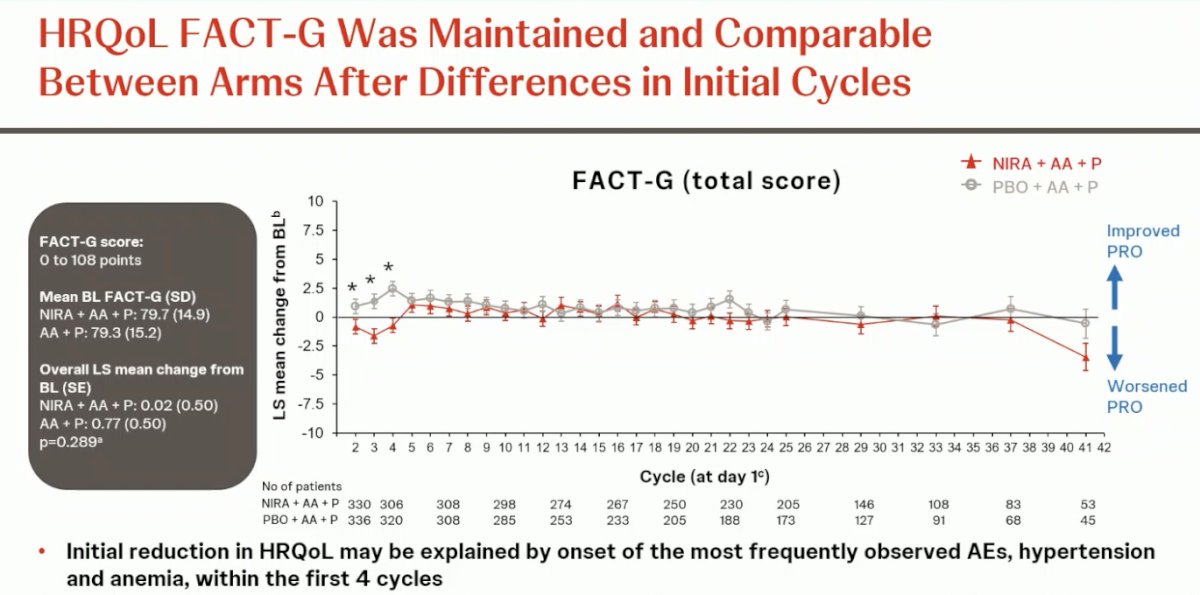
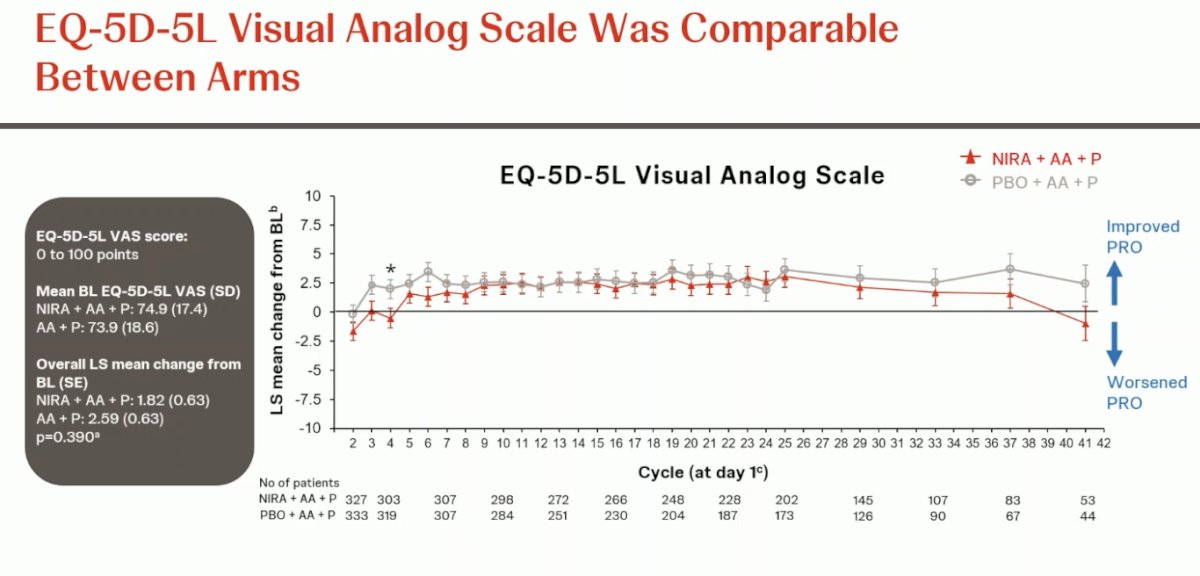
Scores on the EQ-5D-5L visual analog scale were comparable between treatment arms. A transient difference was observed during the first cycle, likely related to early treatment effects, but scores quickly aligned and remained stable thereafter. Overall, quality-of-life outcomes were maintained across both groups without clinically meaningful deterioration.
Dr. Rathkopf concluded her presentation with the following key takeaways:
- Niraparib added to AA + P significantly prolonged time to radiographic progression or death compared with AA + P alone in patients with HRR-mutated mHSPC.
- Health-related quality of life remained stable overall, with only a mild and transient decline early in treatment.
- The initial reduction in HRQoL likely reflected manageable adverse events during early cycles, which improved with supportive care and dose adjustments.
- Adding niraparib to AA + P preserves patients’ quality of life while providing meaningful clinical benefit, with a safety profile in line with previous data for this regimen.
Presented by: Dana E. Rathkopf, MD, Medical Oncologist, Associate Chair, Junior Faculty Development, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between September 17th and 21st.
Related content: Analysis of Patient-Reported Quality of Life from the AMPLITUDE Trial - Eleni Efstathiou
References:
- Di Lorenzo G, Montorsi F, Buonerba C. Re: Gerhardt Attard, Neeraj Agarwal, Julie Graff, et al. Niraparib plus Abiraterone Acetate and Prednisone for HRR-mutated Metastatic Castration-sensitive Prostate Cancer: Results from the AMPLITUDE Phase 3 Trial. J Clin Oncol 2025;43(17 Suppl):LBA5006. Eur Urol Oncol. 2025 Aug;8(4):1215-1216. doi: 10.1016/j.euo.2025.06.006. Epub 2025 Jun 25. PMID: 40571549.
- Rathkopf DE, Roubaud G, Chi KN, Efstathiou E, Attard G, Olmos D, Small EJ, Saad M, Castro E, Kim W, Wu D, Bertzos K, Dibaj S, Zhang J, Francis P, Smith MR. Patient-reported Outcomes for Patients with Metastatic Castration-resistant Prostate Cancer and BRCA1/2 Gene Alterations: Final Analysis from the Randomized Phase 3 MAGNITUDE Trial. Eur Urol. 2025 Oct;88(4):359-369. doi: 10.1016/j.eururo.2024.09.003. Epub 2024 Sep 23. PMID: 39317633.