(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to the session Mini oral session: GU tumours, prostate, penile and testis. Dr. Yüksel Ürün was the Invited Discussant of LBA91, 2420MO, and LBA92 mHSPC in 2025: More, Less, or Smarter?
Dr. Ürün opened by emphasizing the rapidly evolving landscape of mHSPC, noting that androgen deprivation therapy (ADT) alone is no longer acceptable for patients able to tolerate intensified treatment. Over the past decade, the field has transitioned from ADT monotherapy to doublet and triplet combinations, resulting in improved survival outcomes, albeit with increased toxicity, higher costs, and growing inequities in access. He highlighted that contemporary management now balances molecular intensification with clinical pragmatism, underscoring that “we can treat wisely as well as effectively.”
As treatment intensification continues to evolve in mHSPC, prostate cancer can no longer be viewed as a single disease. Clinicians are now layering multiple modalities such as ADT, ARPI, docetaxel, PARPi, radioligand therapy, and radiotherapy, raising the critical question of how to combine these wisely. The key, he noted, is finding the right balance for each patient, enough treatment to maximize benefit without compounding toxicity.
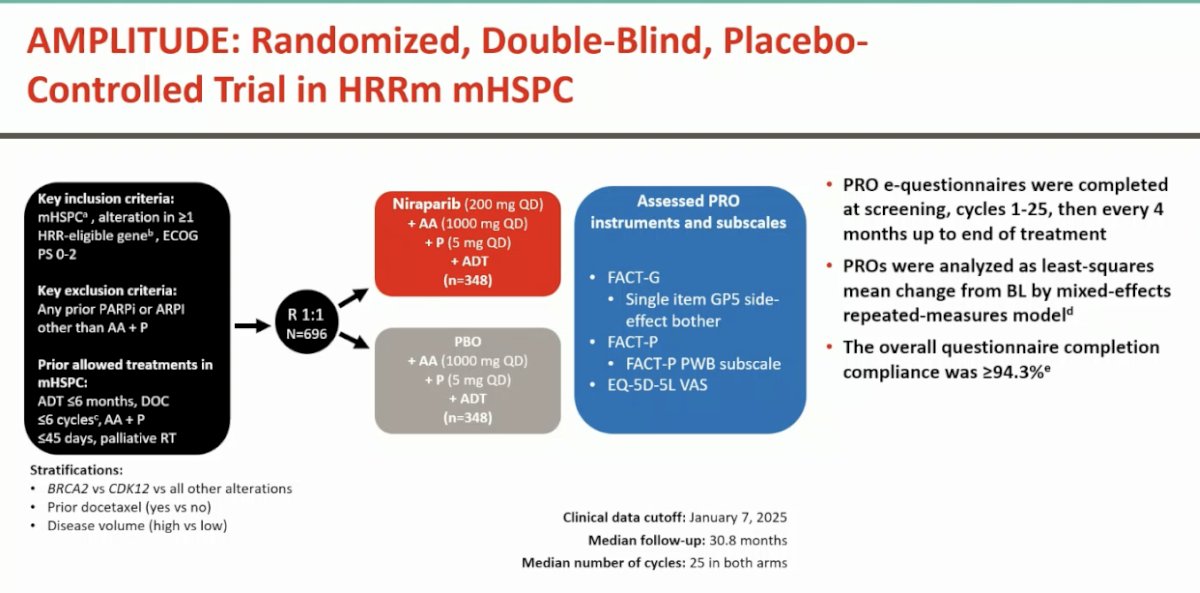
LBA91 - Patient reported outcomes (PROs) from AMPLITUDE, a randomized placebo-controlled phase 3 trial of niraparib (NIRA) and abiraterone acetate (AA) plus prednisone (P) in metastatic hormone-sensitive prostate cancer (mHSPC) with homologous recombination repair mutations (HRRm)The AMPLITUDE trial was a randomized, double-blind, placebo-controlled phase III study that enrolled 696 patients with mHSPC harboring homologous recombination repair mutations. Participants were assigned 1:1 to receive niraparib plus abiraterone acetate and prednisone with ADT, or placebo plus abiraterone acetate and prednisone with ADT. (1)
Patient-reported outcomes were collected electronically at baseline, throughout 25 treatment cycles, and then every four months until the end of therapy. Questionnaires included FACT-G, FACT-P (with its physical well-being subscale), EQ-5D-5L VAS, and a single-item GP5 side-effect bother score, with over 94% completion compliance making it a patient-friendly, comprehensive assessment of treatment tolerability and quality of life.
The AMPLITUDE trial demonstrated a significant improvement in radiographic progression-free survival (HR 0.63, p = 0.0001) with niraparib plus abiraterone acetate and prednisone compared to standard therapy. Quality of life was largely maintained following a transient decline during the early treatment cycles, and the safety profile was consistent with prior experience.
Together, these results suggest that biomarker-selected intensification can deliver meaningful clinical benefit without compromising tolerability a key priority as treatment combinations expand. However, important questions remain as PARP inhibition moves earlier in the disease course: will the benefit extend beyond BRCA mutations to other HRR alterations, and how will patients and payers perceive this shift as precision oncology or as an unnecessary escalation of therapy?
2420MO - Effects of prostate radiotherapy (RT) on synchronous, metastatic, hormone-sensitive prostate cancer (mHSPC): STOPCAP meta-analysis of individual participant data (IPD)
Dr. Ürün then reviewed the STOPCAP meta-analysis of individual participant data evaluating the impact of prostate radiotherapy (RT) in synchronous mHSPC. (2-4) The pooled analysis demonstrated an overall survival improvement that approached statistical significance, with an 8% relative reduction in mortality risk (HR 0.92, p = 0.058). However, only 30% of included patients were from PEACE-1, and he emphasized that only the PEACE-1 cohort remains directly relevant to contemporary practice, given the incorporation of modern systemic intensification with ADT and ARPIs.

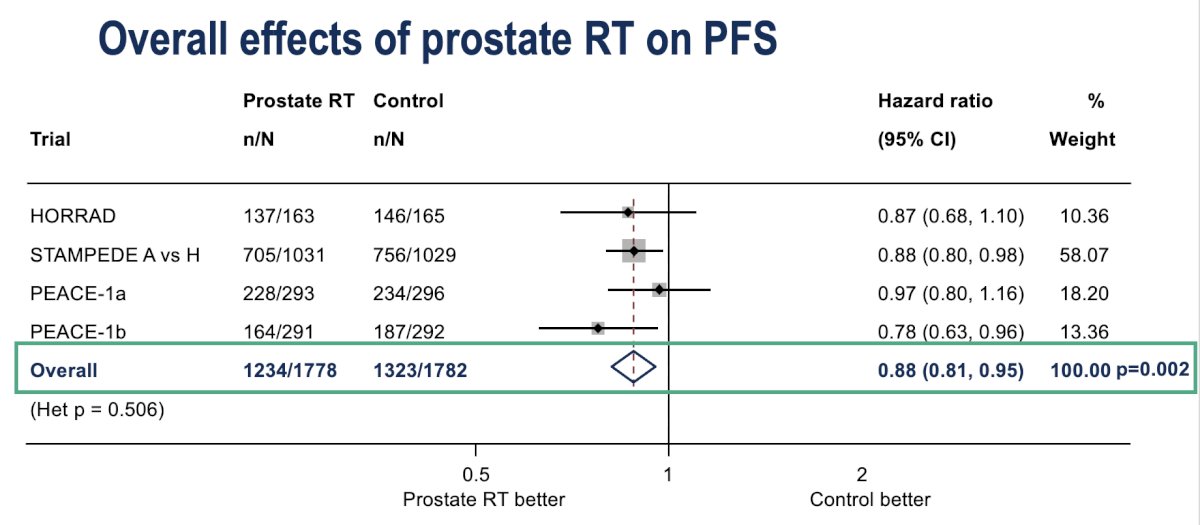
Prostate radiotherapy was associated with a statistically significant 12% reduction in the risk of progression or death (HR 0.88, p = 0.002) across trials in the STOPCAP meta-analysis. While this benefit in progression-free survival reinforces the biological rationale for local control in synchronous mHSPC, he emphasized that the clinical context has evolved, and the relevance of these findings must now be interpreted in the era of intensified systemic therapy, particularly as seen in PEACE-1.
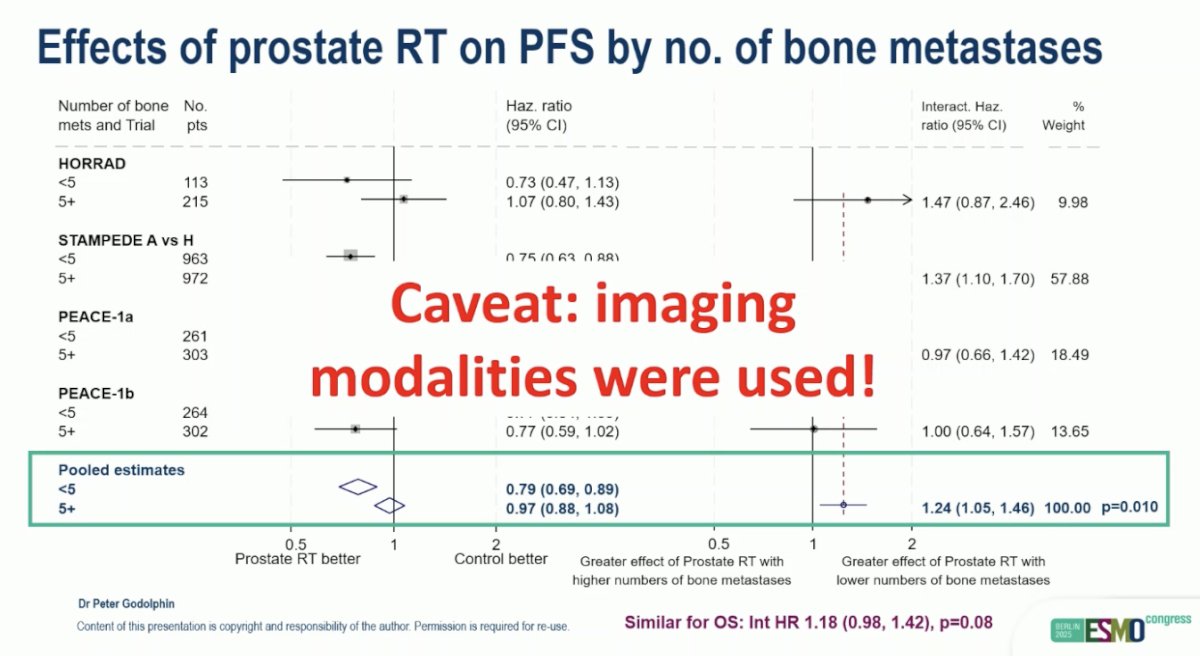
Furthermore, Dr. Ürün presented the subgroup analysis of prostate radiotherapy by number of bone metastases, showing a clear benefit in patients with fewer than five lesions (HR 0.79, p < 0.01), while no significant effect was observed in those with higher disease burden (HR 0.97). He emphasized, however, that these results must be interpreted with caution given the imaging modalities used in these trials primarily bone scans and CT scans which differ from current PSMA PET–based staging. Nonetheless, he noted that current clinical guidelines continue to recommend conventional imaging for treatment decision-making in mHSPC.
Dr. Ürün concluded by highlighting these demonstrated that prostate radiotherapy did not improve overall survival but did significantly prolong radiographic progression-free survival. Moreover in findings from the PEACE-1 trial, showed, it reduced the incidence of severe genitourinary events and delayed the onset of castration resistance, with these benefits observed irrespective of metastatic burden.
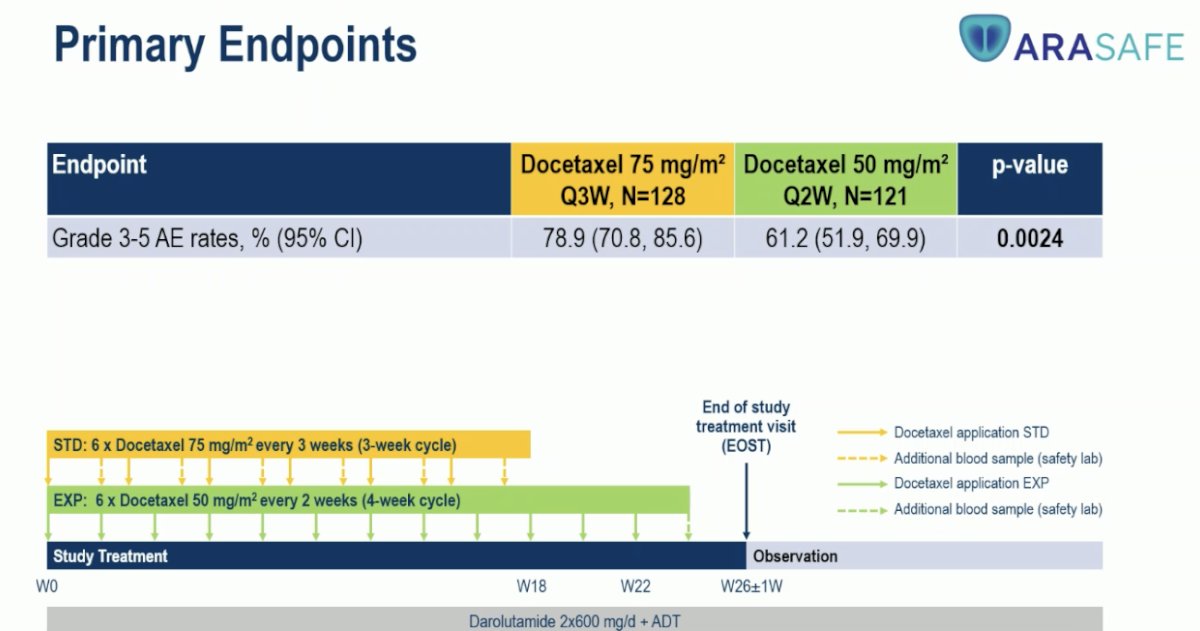
LBA92 - 3-Weekly Docetaxel 75 mg/m2 vs 2-Weekly Docetaxel 50 mg/m2 in Combination with Darolutamide + ADT in Patients with mHSPC – Results from the Randomised Phase 3 ARASAFE TrialLastly, Dr. Ürün discussed the ARASAFE trial, a randomized, open-label, multicenter phase 3 study evaluating darolutamide plus ADT with two different docetaxel dosing schedules in patients with mHSPC: the standard regimen of 75 mg/m² every 3 weeks versus an experimental biweekly schedule of 50 mg/m² every 2 weeks. The primary endpoints were grade 3–5 adverse events and grade 3–4 neutropenia or death, with secondary endpoints including overall survival, time to CRPC, and quality of life. He noted that hospital visits were more frequent in the experimental arm due to the biweekly dosing; and the total cumulative docetaxel dose was substantially higher compared to the standard arm.
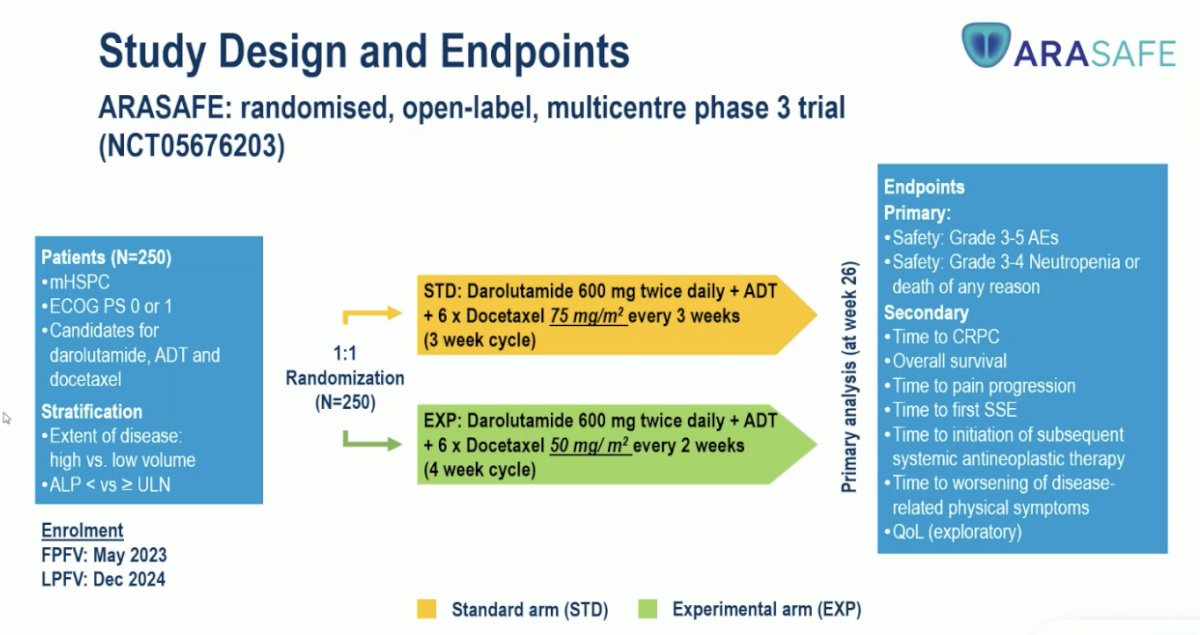
He highlighted that the ARASAFE trial met its primary endpoint, showing a statistically significant reduction in grade 3–5 adverse events with the biweekly docetaxel 50 mg/m² regimen compared to the standard 75 mg/m² every 3 weeks (61.2% vs 78.9%, p=0.0024). This translated into a clear safety advantage for the experimental arm while maintaining treatment intensity.
Dr. Ürün reflected on whether the ARASAFE trial is addressing the right clinical question, emphasizing that in current practice, ADT plus docetaxel alone has largely been replaced by more effective triplet regimens. He questioned whether improving tolerability equates to improving treatment, reminding that “better tolerated toxicity” is not synonymous with “better therapy.” He also noted the paradox that, despite reduced toxicity, patients in the experimental arm received a higher total docetaxel dose, raising important considerations about the long-term effects on marrow health, neuropathy, and quality of life.
Precision in mHSPC extends beyond genomics it includes tolerance, disease volume, and even geography. Each trial represents a balance between efficacy and tolerability, and the future of care lies not only in adding more drugs but in better matching treatments to patients. Yet, the median patient in real-world practice is older, frailer, and often does not meet trial inclusion criteria. This raises several open questions for the field: should docetaxel schedules be tailored to patient frailty? Will radiotherapy retain relevance as triplet therapies become standard? How can patient-reported outcomes more meaningfully guide treatment decisions? Are we adequately accounting for the true burden of care including visits, monitoring, and anxiety when measuring efficacy? And finally, could adaptive, biomarker-driven de-escalation represent the next frontier in prostate cancer management?
Dr. Ürün concluded by emphasizing that ARASAFE highlights how “alternate dosing can be safer,” AMPLITUDE demonstrates that “more can be smarter,” and STOPCAP reminds us that “local may still matter.” Together, these findings illustrate a shift toward a more nuanced, individualized approach to mHSPC care, one that prioritizes both efficacy and tolerability. He also noted that ongoing studies such as CAPItello-281 and PSMAddition will continue to refine and expand this evolving treatment landscape.
Presented by: Yüksel Ürün, MD, Professor of medicine at the Ankara University School of Medicine, specializing in Medical Oncology. Ankara, Türkiye.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
Reference:
- Di Lorenzo G, Montorsi F, Buonerba C. Re: Gerhardt Attard, Neeraj Agarwal, Julie Graff, et al. Niraparib plus Abiraterone Acetate and Prednisone for HRR-mutated Metastatic Castration-sensitive Prostate Cancer: Results from the AMPLITUDE Phase 3 Trial. J Clin Oncol 2025;43(17 Suppl):LBA5006. Eur Urol Oncol. 2025 Aug;8(4):1215-1216. doi: 10.1016/j.euo.2025.06.006. Epub 2025 Jun 25. PMID: 40571549.
- Boevé LMS, Hulshof MCCM, Verhagen PCMS, Twisk JWR, Witjes WPJ, de Vries P, Jeroen A van Moorselaar R, Vis AN, van Andel G. Prostate Cancer-related Events in Patients with Synchronous Metastatic Hormone-sensitive Prostate Cancer Treated with Androgen Deprivation Therapy with and Without Concurrent Radiation Therapy to the Prostate; Data from the HORRAD Trial. Eur Urol. 2025 Mar;87(3):357-363. doi: 10.1016/j.eururo.2024.08.035. Epub 2024 Sep 20. PMID: 39304427.
- Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Gravis G, Calabro F, Berdah JF, Hasbini A, Silva M, Thiery-Vuillemin A, Latorzeff I, Mourey L, Laguerre B, Abadie-Lacourtoisie S, Martin E, El Kouri C, Escande A, Rosello A, Magne N, Schlurmann F, Priou F, Chand-Fouche ME, Freixa SV, Jamaluddin M, Rieger I, Bossi A; PEACE-1 investigators. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707. doi: 10.1016/S0140-6736(22)00367-1. Epub 2022 Apr 8. PMID: 35405085.
- Parker CC, James ND, Brawley CD, Clarke NW, Hoyle AP, Ali A, Ritchie AWS, Attard G, Chowdhury S, Cross W, Dearnaley DP, Gillessen S, Gilson C, Jones RJ, Langley RE, Malik ZI, Mason MD, Matheson D, Millman R, Russell JM, Thalmann GN, Amos CL, Alonzi R, Bahl A, Birtle A, Din O, Douis H, Eswar C, Gale J, Gannon MR, Jonnada S, Khaksar S, Lester JF, O'Sullivan JM, Parikh OA, Pedley ID, Pudney DM, Sheehan DJ, Srihari NN, Tran ATH, Parmar MKB, Sydes MR; Systemic Therapy for Advanced or Metastatic Prostate cancer: Evaluation of Drug Efficacy (STAMPEDE) investigators. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018 Dec 1;392(10162):2353-2366. doi: 10.1016/S0140-6736(18)32486-3. Epub 2018 Oct 21. PMID: 30355464; PMCID: PMC6269599.