(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to the session Mini oral session: GU tumours, prostate, penile and testis. Dr. Peter J. Godolphin discussed Effects of prostate radiotherapy (RT) on synchronous, metastatic, hormone-sensitive prostate cancer (mHSPC): STOPCAP meta-analysis of individual participant data (IPD).
The analysis presented by Dr. Godolphin was based on the STOPCAP meta-analysis of individual participant data, which pooled results from all eligible randomized trials evaluating the addition of prostate radiotherapy (RT) to standard of care (SoC) in men with de novo metastatic prostate cancer disease confirmed by conventional CT and/or bone scans. The primary aim of this analysis was to assess the effect of adding prostate radiotherapy (RT) to standard of care (SOC) in men with de novo metastatic prostate cancer. Secondary aims evaluated whether the treatment effect varied according to patient characteristics or concomitant docetaxel use.
Dr. Godolphin outlined that the primary outcome of this analysis was overall survival (OS), while progression-free survival (PFS) served as the main outcome for subgroup analyses. Additional endpoints, such as failure-free survival (FFS) and time to symptomatic local event requiring intervention, were not presented in this report.
A two-stage fixed-effects meta-analysis of hazard ratios (HRs) was conducted, adjusting for age, PSA, performance status, Gleason score, and planned docetaxel use. The analysis also accounted for changes in trial design in key contributing studies, including STAMPEDE and PEACE-1.1-3
The analysis included data from four key randomized trials: HORRAD, STAMPEDE, and two PEACE-1 cohorts (RT with and without abiraterone).1-3 Across studies, follow-up ranged from 5 to 9 years, with baseline survival between 3.2 and 5.3 years. The proportion of patients planned for docetaxel varied widely from 0% in HORRAD to over 60% in the PEACE-1 cohorts. HORRAD data, representing 76% of its original participants, could not be included in the volume-based subgroup analyses because visceral metastases were not recorded.

Dr. Godolphin presented the overall effects of prostate RT on OS, showing a pooled hazard ratio of 0.92 (95% CI 0.84–1.00; p=0.058). While not reaching conventional statistical significance, the trend favored prostate RT. No significant heterogeneity was observed across studies (p=0.664), suggesting consistent findings between HORRAD, STAMPEDE, and the PEACE-1 cohorts.

Similarly, the pooled analysis for progression-free survival demonstrated a significant benefit with prostate RT, with a hazard ratio of 0.88 (95% CI 0.81–0.95; p=0.002). The effect was consistent across all included studies (heterogeneity p=0.506), supporting the robustness of the finding.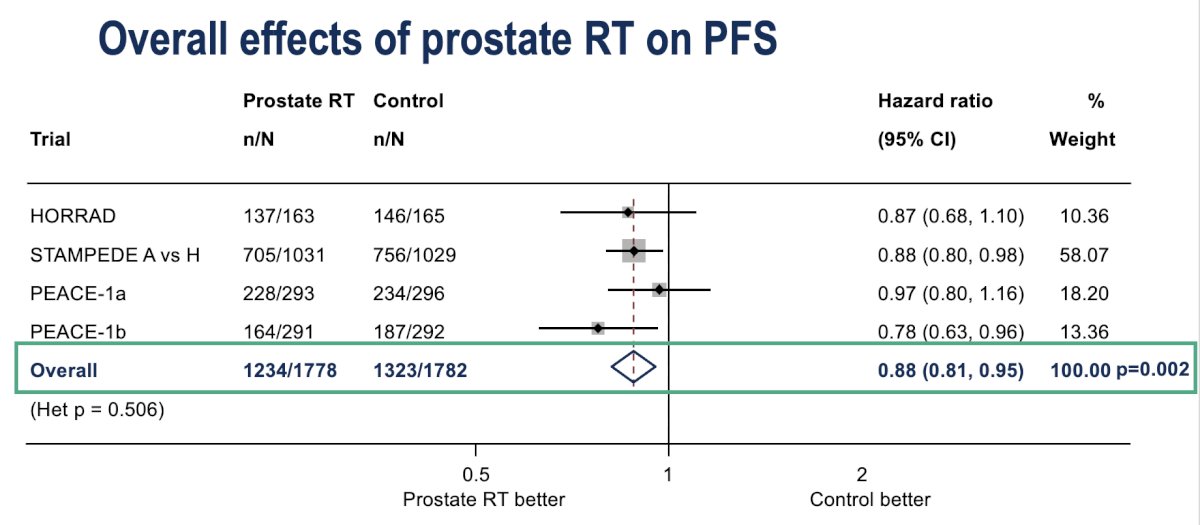
Moreover, when stratified by metastatic burden, prostate RT significantly improved progression-free survival in patients with fewer than five bone metastases (HR 0.79; 95% CI 0.69–0.89), but not in those with five or more (HR 0.97; 95% CI 0.88–1.08). The interaction p-value was 0.010, confirming a greater benefit in patients with low-volume disease. Similar trends were observed for overall survival (interaction HR 1.18; 95% CI 0.98–1.42; p=0.08).

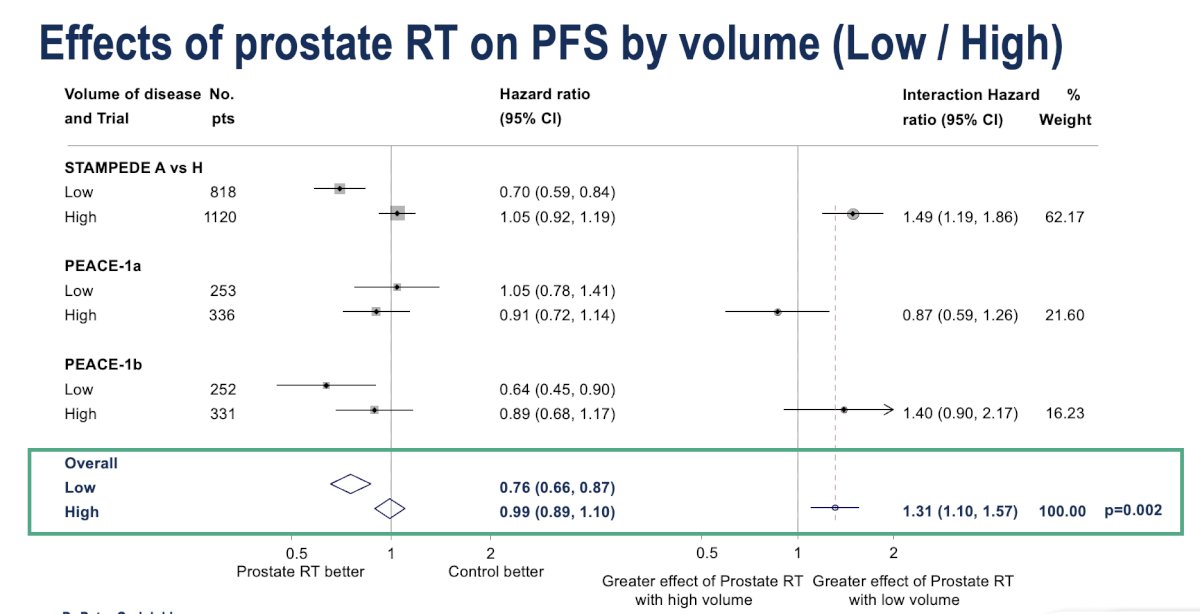
Furthermore, when analyzed by disease volume (excluding HORRAD from this analysis), prostate RT significantly improved progression-free survival in patients with low-volume disease (HR 0.76; 95% CI 0.66–0.87), whereas no benefit was seen in those with high-volume disease (HR 0.99; 95% CI 0.89–1.10). The interaction p-value was 0.002, confirming a greater effect in low-volume cases. Similar trends were observed for overall survival (interaction HR 1.31; 95% CI 1.07–1.60; p=0.009).
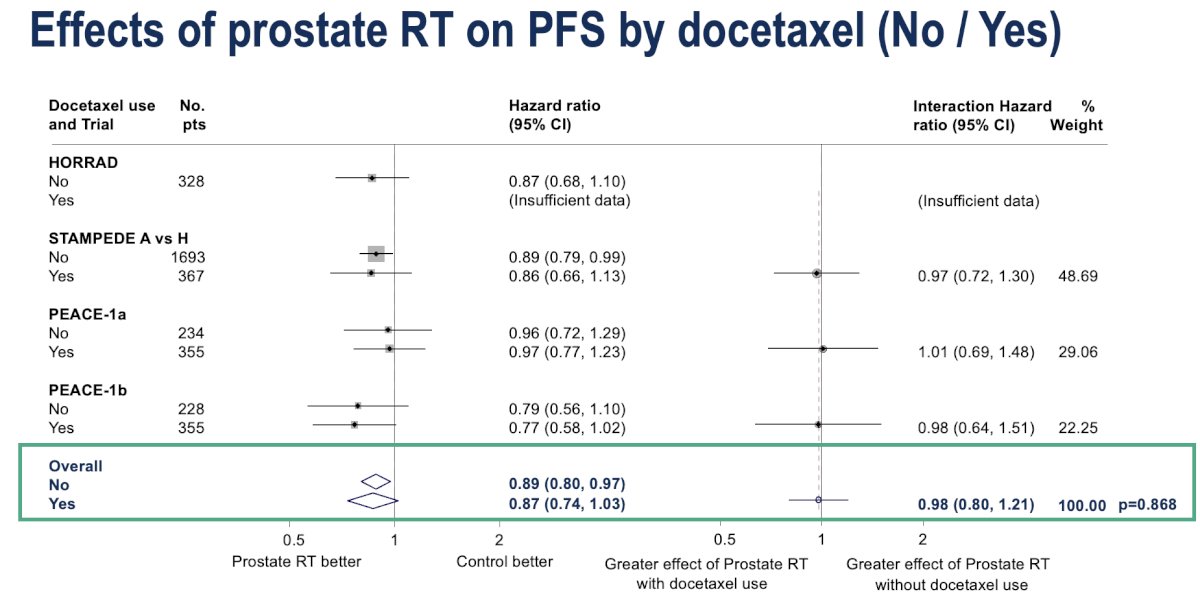
Lastly, the benefit of prostate RT on progression-free survival was consistent regardless of concurrent docetaxel use. The pooled HR was 0.89 (95% CI 0.80–0.97) for patients not receiving docetaxel and 0.87 (95% CI 0.74–1.03) for those who did, with no significant interaction between groups (interaction HR 0.98; 95% CI 0.80–1.21; p=0.868).
Dr. Godolphin highlighted that the effect of prostate RT on progression-free survival did not vary by age, BMI, performance status, nodal involvement, tumor stage, or Gleason score. He also noted that upcoming analyses will include the full HORRAD dataset, updated follow-up from PEACE-1, and evaluation of RT effects on symptomatic local events requiring intervention.
Dr. Godolphin concluded his presentation with the following summary of current results:
- This is the first individual patient data meta-analysis of prostate RT trials in mHSPC.
- Across all patients, prostate RT provided a modest benefit in overall and progression-free survival.
- The survival benefit was confined to patients with fewer than five bone metastases, with an approximate 5% absolute improvement in 5-year survival.
- A similar benefit was observed in those with low-volume disease, corresponding to an ~8% absolute improvement in 5-year survival.
- No difference in treatment effect was seen according to planned docetaxel use.
Presented by: Peter J. Godolphin, MSc, PhD, Senior Research Fellow, University College London, MRC Clinical Trials Unit at UCL, London, United Kingdom
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
Reference:
- Boevé LMS, Hulshof MCCM, Verhagen PCMS, Twisk JWR, Witjes WPJ, de Vries P, Jeroen A van Moorselaar R, Vis AN, van Andel G. Prostate Cancer-related Events in Patients with Synchronous Metastatic Hormone-sensitive Prostate Cancer Treated with Androgen Deprivation Therapy with and Without Concurrent Radiation Therapy to the Prostate; Data from the HORRAD Trial. Eur Urol. 2025 Mar;87(3):357-363. doi: 10.1016/j.eururo.2024.08.035. Epub 2024 Sep 20. PMID: 39304427.
- Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Gravis G, Calabro F, Berdah JF, Hasbini A, Silva M, Thiery-Vuillemin A, Latorzeff I, Mourey L, Laguerre B, Abadie-Lacourtoisie S, Martin E, El Kouri C, Escande A, Rosello A, Magne N, Schlurmann F, Priou F, Chand-Fouche ME, Freixa SV, Jamaluddin M, Rieger I, Bossi A; PEACE-1 investigators. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707. doi: 10.1016/S0140-6736(22)00367-1. Epub 2022 Apr 8. PMID: 35405085.
- Parker CC, James ND, Brawley CD, Clarke NW, Hoyle AP, Ali A, Ritchie AWS, Attard G, Chowdhury S, Cross W, Dearnaley DP, Gillessen S, Gilson C, Jones RJ, Langley RE, Malik ZI, Mason MD, Matheson D, Millman R, Russell JM, Thalmann GN, Amos CL, Alonzi R, Bahl A, Birtle A, Din O, Douis H, Eswar C, Gale J, Gannon MR, Jonnada S, Khaksar S, Lester JF, O'Sullivan JM, Parikh OA, Pedley ID, Pudney DM, Sheehan DJ, Srihari NN, Tran ATH, Parmar MKB, Sydes MR; Systemic Therapy for Advanced or Metastatic Prostate cancer: Evaluation of Drug Efficacy (STAMPEDE) investigators. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018 Dec 1;392(10162):2353-2366. doi: 10.1016/S0140-6736(18)32486-3. Epub 2018 Oct 21. PMID: 30355464; PMCID: PMC6269599.