Dr. Decruyenaere highlighted that this retrospective multicenter cohort study, conducted across 18 Belgian institutions, evaluated patients with mRCC who had been treated with immune checkpoint inhibitors (ICPI) for at least 21 months without toxicity. The study compared two groups: those who continued ICPI therapy (n=80) versus those who elected to discontinue treatment between 21–25 months (n=15). Both unadjusted and adjusted statistical analyses were performed to address immortal time and confounding bias, applying artificial censoring and inverse probability weighting based on 11 prespecified variables, including age, sex, ECOG status, IMDC risk, metastatic pattern, histology, sarcomatoid features, ICPI type, and best RECIST response.
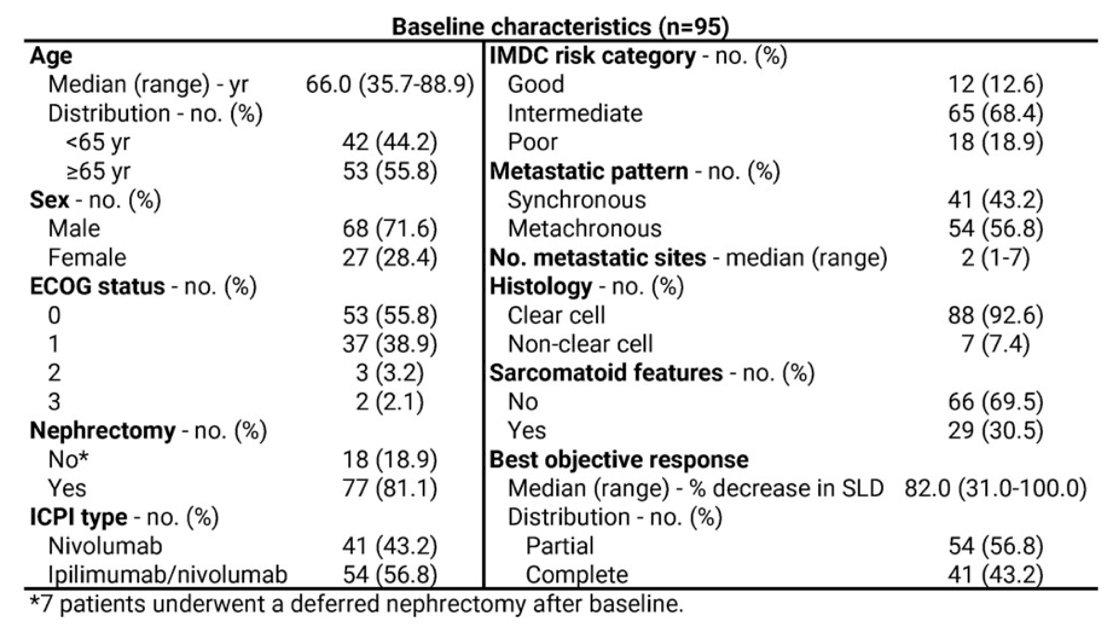
Baseline characteristics for the 95 included patients are summarized in the table. The median age was 66 years, with 56% aged ≥65 and 72% being male. Most patients had ECOG 0–1 (95%) and prior nephrectomy (81%). The majority were classified as intermediate IMDC risk (68%) and had clear-cell histology (93%), with 30% exhibiting sarcomatoid features. The median number of metastatic sites was 2, and 57% had metachronous disease. Regarding treatment, 57% received ipilimumab/nivolumab and 43% nivolumab monotherapy. The best objective response achieved was partial in 57% and complete in 43% of patients, with a median tumor size reduction of 82%.
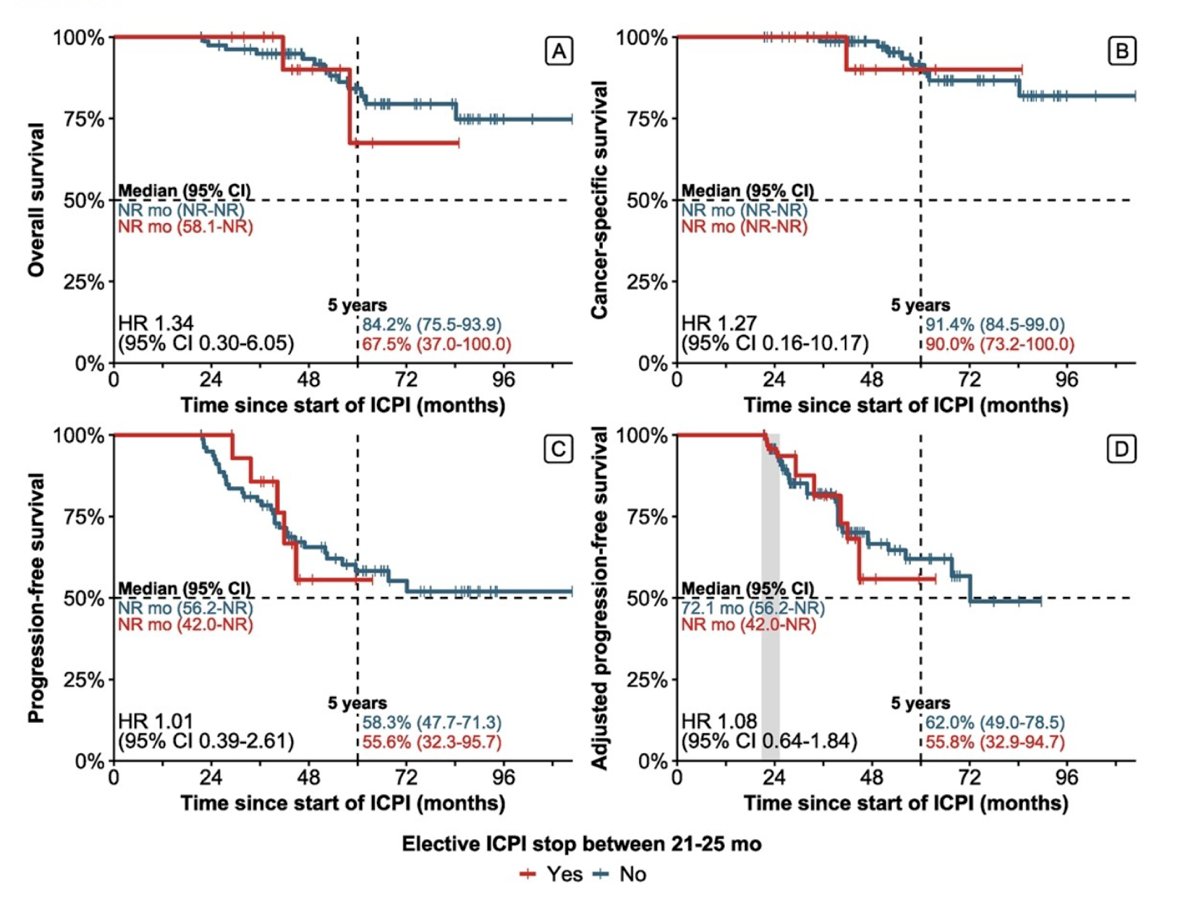
Median OS, CSS, and PFS were not reached in either group. At 5 years, OS was 84.2% for patients who continued ICPI versus 67.5% for those who stopped, while CSS was 91.4% versus 90.0%, respectively. Median PFS was 72.1 months for ICPI continuation and 42.0 months for elective discontinuation, with similar adjusted PFS outcomes (HR 1.08, 95% CI 0.64–1.84). The 5-year PFS rate difference was only 6.2%, translating to a number needed to harm of 17, suggesting that elective discontinuation after approximately 2 years did not substantially compromise long-term outcomes.
Among patients who elected to discontinue ICPI, the median stopping time was 29 months (95% CI 26.5–35.6), with 65% stopping between 24 and 36 months. Elective discontinuation at approximately 24 months resulted in a median reduction of 26.4 months (95% CI 23.1–29.6) of ICPI exposure per patient—representing a substantial decrease in treatment duration and potential toxicity burden, without compromising long-term efficacy outcomes.

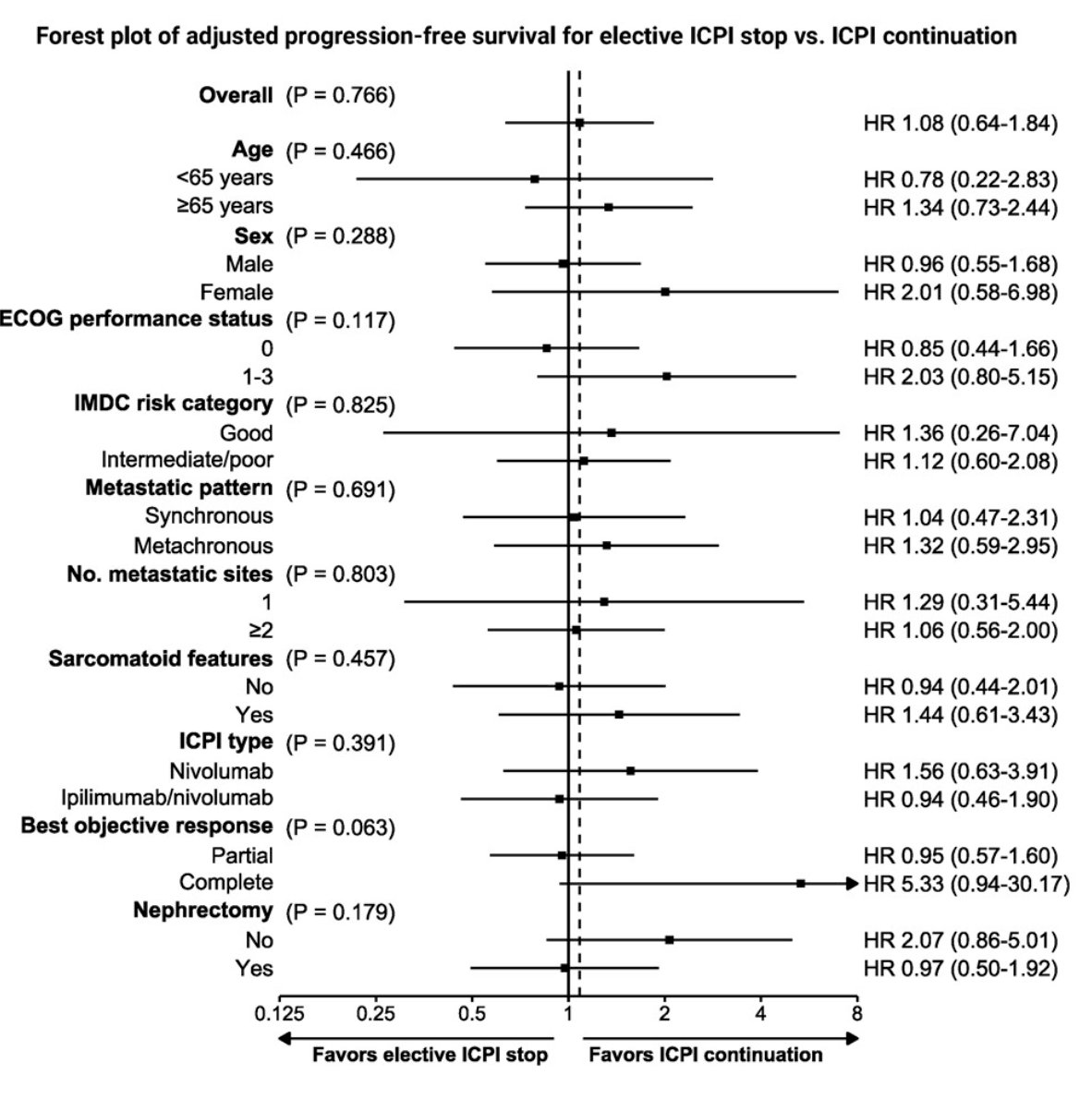
Lastly, subgroup analyses showed no significant differences in adjusted PFS between patients who stopped ICPI electively and those who continued treatment across all clinical variables, including age, ECOG status, IMDC risk group, number of metastatic sites, or sarcomatoid features. The only trend observed was a potential benefit for ICPI continuation among patients achieving a complete response (HR 5.33, 95% CI 0.94–30.17; p=0.063), though this did not reach statistical significance. Overall, elective discontinuation at around 24 months appeared safe and feasible without compromising disease control in most subgroups.
Dr. Decruyenaere concluded that in patients with responding mRCC, elective discontinuation of immune checkpoint inhibitor therapy around 24 months does not appear to compromise survival outcomes compared to continued treatment. This approach offers a meaningful opportunity to reduce treatment exposure and potential toxicity without negatively impacting long-term efficacy.
Presented by: Alexander Decruyenaere, MD, Medical Oncologist at the Department of Medical Oncology Ghent University Hospital, Gent, Belgium
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025