(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st, was host to the session Mini Oral session 2: GU tumours, renal & urothelial. Dr. Sarah Scagliarini was the invited discussant for mini-oral abstracts 2593MO, 2594MO, and 2613MO.
Dr. Scagliarini began her presentation by noting that she would be discussing biomarkers in renal cell carcinoma (RCC), focusing specifically on three key abstracts. She highlighted that this discussion is particularly timely, coming just days after the 2025 Nobel Prize in Physiology or Medicine was awarded to Mary E. Brunkow, Fred Ramsdell, and Shimon Sakaguchi for their groundbreaking discoveries in peripheral immune tolerance. She emphasized the importance of addressing three fundamental questions in this context: What biomarkers should be used? Why are they relevant? And when and in which patients should they be applied?
There is a pressing need for biomarkers in RCC, raising the key question: What exactly is a biomarker? She defined it as a measurable indicator of a biological context in RCC but noted several challenges that complicate its use, including intratumoral heterogeneity, dynamic evolution under drug pressure, and the distinct immune biology of RCC, which lacks clear oncogenic or tumor microenvironment targets. Therefore, she concluded that relying on a single biomarker is insufficient, underscoring the necessity for incorporating translational endpoints into clinical trials to better understand and guide therapy.
Dr. Scagliarini outlined the critical role of biomarkers in kidney cancer, emphasizing their relevance across the entire disease spectrum. In small renal masses, they could help guide decisions between observation, surgery, or local therapy. After surgery, biomarkers may inform whether patients should undergo surveillance or receive adjuvant therapy. In metastatic disease, they can support prognostic assessment, predict therapy response, guide selection among various combination regimens, and even enable treatment de-escalation strategies. Ultimately, she noted, the goal of biomarker development in RCC can be summarized in two words: therapy personalization.
Dr. Scagliarini transitioned to the metastatic RCC setting, posing the question of when biomarkers should be integrated into clinical practice. She noted that the field is currently awaiting results from ongoing trials testing new triplet regimens, adaptive and sequential approaches, and pragmatic designs exploring novel strategies. She referenced four key phase III studies with long-term follow-up: KEYNOTE-426 (5 years), CLEAR/KEYNOTE-581 (4 years), CheckMate 9ER (5 years), and CheckMate 214, with the latter demonstrating a remarkable 9-year survival in a metastatic population.1-4 These data, she noted, highlight the evolving landscape of mRCC therapy and the potential role of biomarkers in refining future treatment strategies.

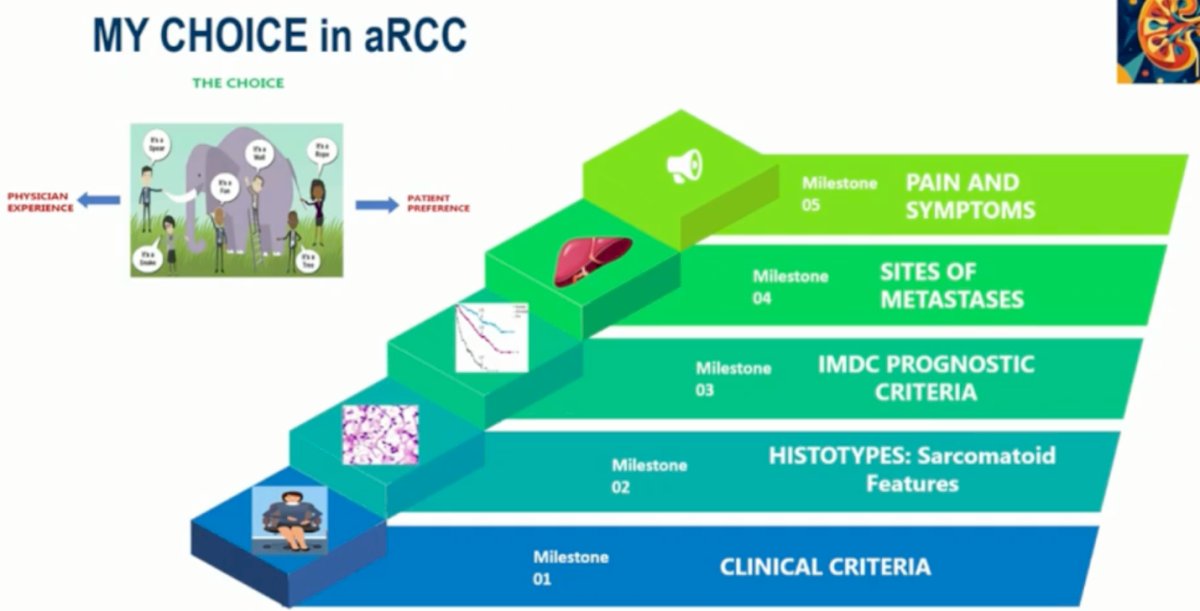
In her clinical practice, Dr. Scagliarini emphasized that treatment choice in advanced RCC is a balance between physician experience and patient preference. She illustrated her decision-making framework through five key milestones: starting with clinical criteria, followed by histologic subtype and sarcomatoid features, IMDC prognostic classification, sites of metastases, and finally, patient pain and symptom burden. She underscored that while data-guided therapy, personalization anchored in both objective disease characteristics and patient-centered factors, remains at the heart of clinical decision-making in RCC.
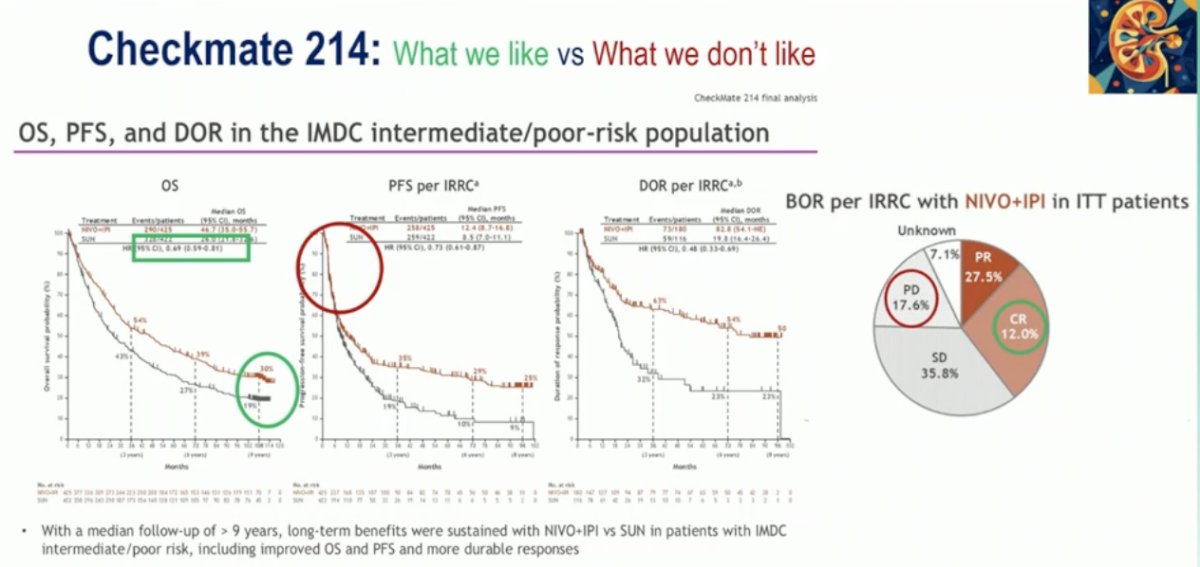
Revisiting the CheckMate 214 trial, Dr. Scagliarini highlighted both the strengths and limitations of the long-term data. With a median follow-up of over nine years, nivolumab plus ipilimumab continues to show sustained overall and progression-free survival benefits over sunitinib in patients with IMDC intermediate or poor-risk disease, along with more durable responses. She pointed out that the complete response rate reached 12%, and partial responses were observed in nearly 28% of patients.4 However, she also noted that about one in six patients still experienced primary progression, emphasizing that while dual ICI remains a cornerstone for this population, predictive biomarkers are urgently needed to better identify who truly benefits from this approach.
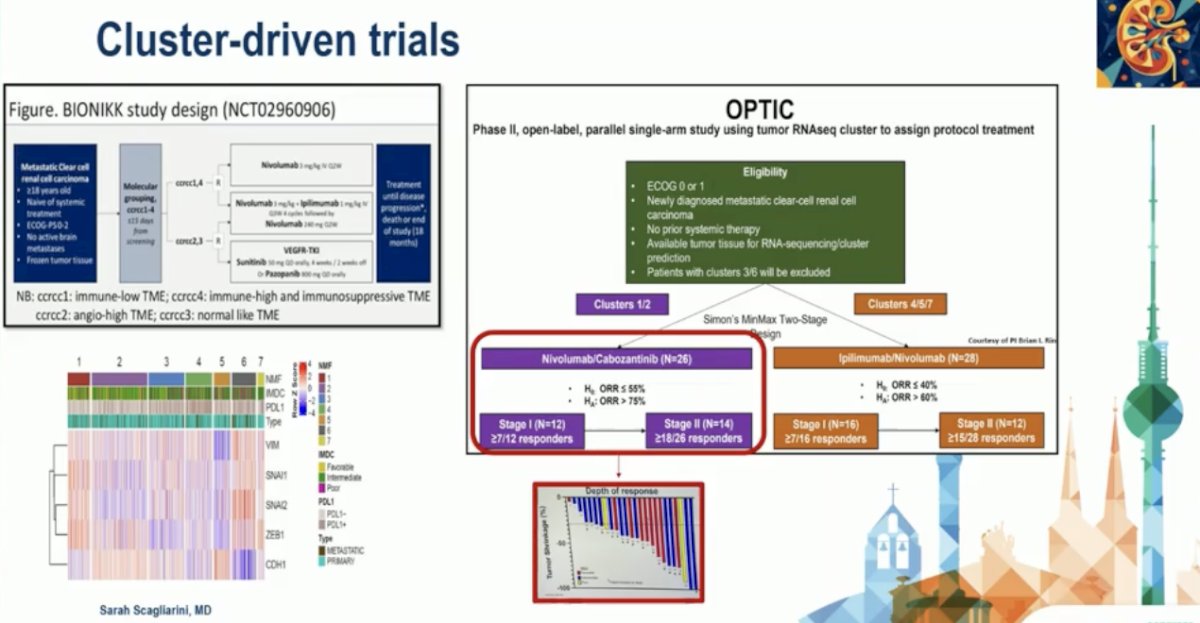
Dr. Scagliarini emphasized that a paradigm shift is underway in RCC with the rise of cluster-driven trials, designed to personalize therapy based on the tumor’s molecular and immune landscape. She highlighted the BIONIK and OPTIC studies as prime examples of this approach. In the BIONIK study, patients are stratified into molecular subgroups reflecting distinct tumor microenvironments: immune-low, immune-high/immunosuppressive, and angiogenic clusters to guide treatment with nivolumab, ipilimumab, or sunitinib accordingly. Similarly, the OPTIC trial uses RNA sequencing to assign patients to specific treatment clusters, such as nivolumab–cabozantinib or ipilimumab–nivolumab combinations, depending on their molecular profile. The OPTIC and BIONIK trials' design is outlined below.
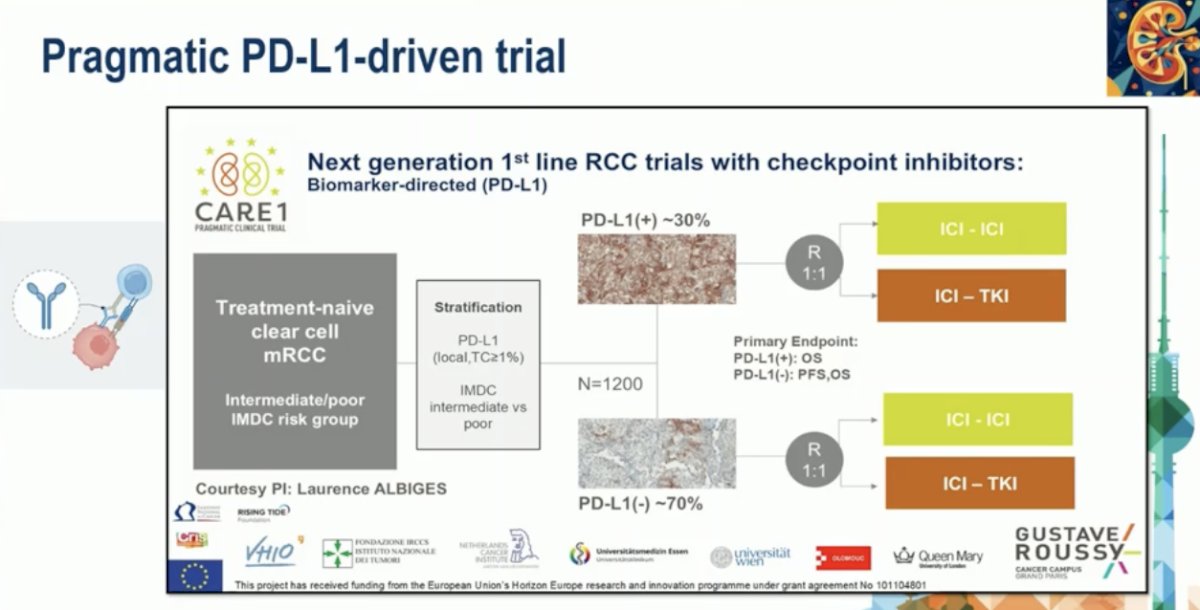
Furthermore, Dr. Scagliarini highlighted the emergence of pragmatic PD-L1–driven trials, such as the CARE1 study, which represents the next generation of biomarker-directed first-line RCC research. This trial enrolls treatment-naïve patients with clear cell mRCC in the intermediate or poor IMDC risk groups and stratifies them based on PD-L1 expression (approximately 30% PD-L1 positive vs 70% PD-L1 negative). Patients are then randomized 1:1 to receive either ICI–ICI or ICI–TKI combinations. The primary endpoint for PD-L1(+) tumors is overall survival, while for PD-L1(–) tumors, both PFS and OS are evaluated. This approach aims to answer a key clinical question: can PD-L1 expression long debated in RCC, finally serve as a reliable biomarker to guide treatment selection between dual immunotherapy and immunotherapy–TKI combinations in real-world settings?
The study presented by Dr. McKay and discussed by Dr. Scagliarini analyzed de-identified DNA- and RNA-sequencing data from patients with RCC who received first-line immunotherapy, using the Tempus multimodal database. Patients were stratified into quartiles according to LAG-3 RNA expression levels.
The analysis revealed that increased LAG-3 RNA expression was associated with a higher objective response rate and lower rates of progressive disease (p=0.034), suggesting a potential predictive role for LAG-3 in immunotherapy response. However, no significant association was observed between LAG-3 expression and overall survival.
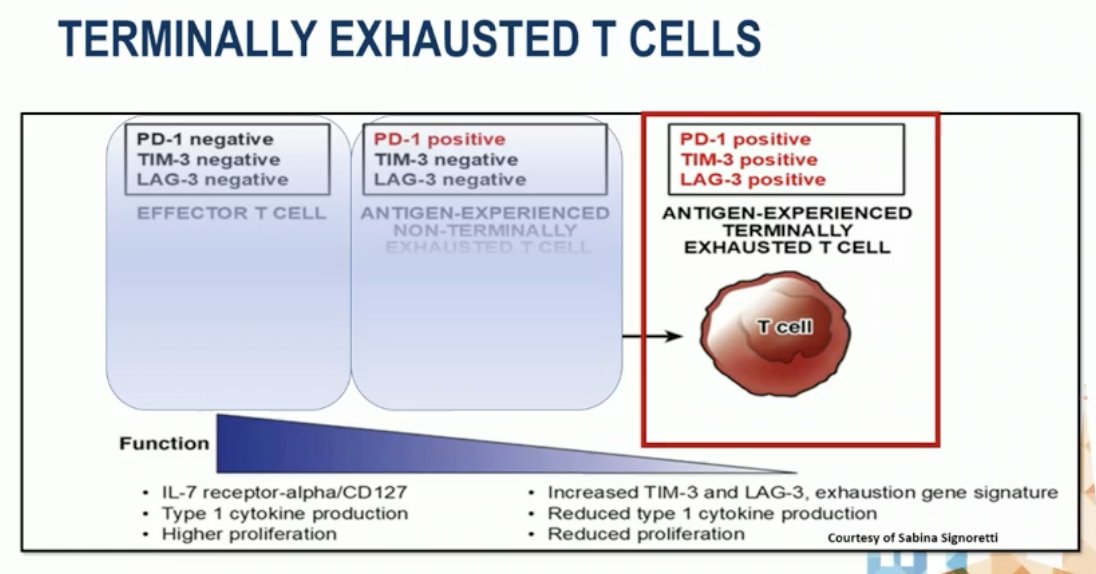
Dr. Scagliarini emphasized that this represents a clear example of T-cell exhaustion. In this state, antigen-experienced T cells express high levels of inhibitory receptors such as PD-1, TIM-3, and LAG-3. These “terminally exhausted” T cells show reduced IL-7 receptor (CD127) expression, diminished type 1 cytokine production, and impaired proliferative capacity.
She explained that this phenotype reflects chronic antigen exposure, leading to functional decline despite the presence of immune activation markers—underscoring the challenge of reversing exhaustion in the tumor microenvironment and the potential role of LAG-3 blockade to restore T-cell function in RCC, as shown in the figure below.
This abstract is important because tumors with high LAG-3 expression demonstrate a complex immune landscape showing strong effector cell infiltration (including CD8+ T cells, NK cells, and M1 macrophages) while simultaneously activating immunosuppressive mechanisms (such as M2 macrophages and Tregs), suggesting an adaptive resistance phenotype.
She described this as an elegant and original piece of work in RCC, highlighting that it underscores a key therapeutic implication: single-agent checkpoint inhibition may be insufficient due to overlapping suppressive pathways. Instead, multi-targeted combination strategies including LAG-3, PD-1/PD-L1, and other checkpoint inhibitors may be required to restore T-cell function and achieve meaningful, durable antitumor responses.
2613MO - Identifying Biomarkers of Response to First-Line Nivolumab plus Ipilimumab Therapy in Patients with Metastatic Clear Cell Renal Cell Carcinoma (mccRCC) enrolled in the COSMIC 313 trialDr. Scagliarini then introduced the abstract presented by Dr. Berkay Simsek, which focused on identifying biomarkers of response to first-line nivolumab plus ipilimumab therapy in patients with metastatic clear cell RCC enrolled in the COSMIC-313 trial. (5) The COSMIC-313 study design is shown below.
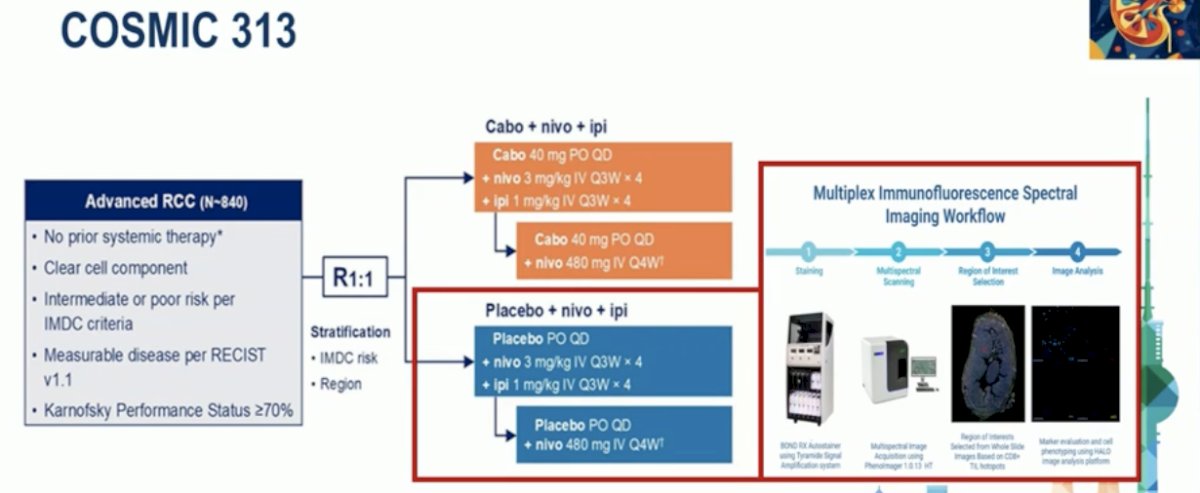
She noted that prior studies have shown that CD8+ T cells expressing PD-1 but not TIM-3 or LAG-3 are associated with improved outcomes to anti–PD-1 monotherapy in metastatic RCC. Building on this, the COSMIC-313 analysis aimed to assess whether the presence of CD8+PD-1+TIM-3–LAG-3 tumor-infiltrating lymphocytes (TILs) correlates with better clinical outcomes in patients treated with the nivolumab–ipilimumab combination, providing further insight into immune cell phenotypes predictive of therapeutic response.
Dr. Scagliarini emphasized that this abstract matters because a high density of CD8+PD-1+TIM-3–LAG-3– tumor-infiltrating lymphocytes (TILs) was associated with improved overall response rate (60.4% vs 37.9%, p=0.005) and longer progression-free survival (not reached vs 9.3 months, p=0.001) in patients receiving first-line nivolumab plus ipilimumab.
She described it as “a pebble in the pond,” highlighting that this finding could represent an early step toward identifying a predictive biomarker of response to dual immune checkpoint blockade. She concluded by questioning whether further validation through randomized studies should be prioritized to confirm its predictive value and potential correlation with overall survival.
2594MO - Association of circulating kidney injury molecule-1 (KIM-1) levels with clinical outcomes in advanced renal cell carcinoma (aRCC): Retrospective analysis of COSMIC-313Lastly, Dr. Scagliarini introduced the abstract presented by Dr. Wenxin Xu, which evaluated circulating kidney injury molecule-1 (KIM-1) levels and their association with clinical outcomes in advanced renal cell carcinoma, using data from the COSMIC-313 trial.
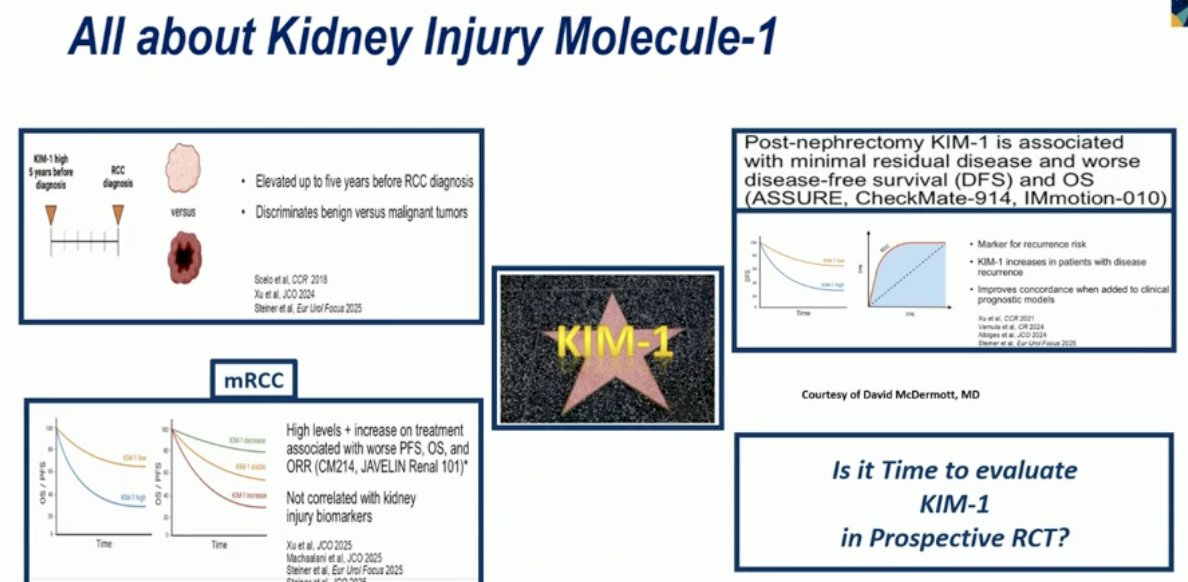
She explained that KIM-1 is a transmembrane protein overexpressed in clear cell RCC and serves as a circulating biomarker for early detection, risk stratification, and disease recurrence. The study explored the relationship between baseline KIM-1 levels and key clinical variables, including tumor response, progression-free survival (PFS), and overall survival (OS) to determine its prognostic and potentially predictive value in patients treated with first-line nivolumab plus ipilimumab.
Moreover, KIM-1 remains one of the most well-recognized and promising biomarkers in RCC. Elevated KIM-1 levels can be detected up to five years before RCC diagnosis and can help discriminate between benign and malignant renal tumors. Post-nephrectomy, higher KIM-1 levels have been linked with minimal residual disease and worse DFS and OS, as shown in studies such as ASSURE, CheckMate-914, and IMmotion-010, as illustrated below.
In metastatic RCC, high or rising KIM-1 levels during treatment have been associated with worse PFS, OS, and ORR, as observed in COSMIC-313, CheckMate 214, and JAVELIN Renal 101. A key question remains: “Is it time to evaluate KIM-1 in a prospective randomized clinical trial?” highlighting COSMIC-313 as a critical step toward that goal.
Dr. Scagliarini concluded that in COSMIC-313, patients with poor-risk disease, larger tumor burden, and no prior nephrectomy had significantly higher baseline KIM-1 levels, which were associated with worse OS. A correlation between KIM-1 dynamics and treatment response was observed at Week 7 in the cabozantinib–nivolumab–ipilimumab arm and at both Weeks 4 and 7 in the nivolumab–ipilimumab arm. The association with OS was seen only for nivolumab–ipilimumab. Overall, the prognostic value of KIM-1 was reaffirmed; however, as in prior studies, its predictive correlation with treatment response appears less robust in patients receiving TKIs.
Dr. Scagliarini concluded her presentation by emphasizing that “it’s not noise, it’s process,” highlighting that the future of renal cell carcinoma research lies in the integration of multiple biomarkers. She underscored the importance of new pragmatic, biomarker-driven trials that move beyond single-variable approaches to refine patient selection, optimize therapeutic strategies, and personalize treatment in RCC.
Presented by: Sarah Scagliarini, MD, Medical Oncologist at AORN Cardarelli in Naples
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
References:
- Plimack ER, Powles T, Stus V, Gafanov R, Nosov D, Waddell T, Alekseev B, Pouliot F, Melichar B, Soulières D, Borchiellini D, McDermott RS, Vynnychenko I, Chang YH, Tamada S, Atkins MB, Li C, Perini R, Molife LR, Bedke J, Rini BI. Pembrolizumab Plus Axitinib Versus Sunitinib as First-line Treatment of Advanced Renal Cell Carcinoma: 43-month Follow-up of the Phase 3 KEYNOTE-426 Study. Eur Urol. 2023 Nov;84(5):449-454. doi: 10.1016/j.eururo.2023.06.006. Epub 2023 Jul 25. Erratum in: Eur Urol. 2023 Nov;84(5):e123-e124. doi: 10.1016/j.eururo.2023.08.010. Erratum in: Eur Urol. 2024 Feb;85(2):e58-e59. doi: 10.1016/j.eururo.2023.11.016. PMID: 37500340.
- Motzer R, Alekseev B, Rha SY, Porta C, Eto M, Powles T, Grünwald V, Hutson TE, Kopyltsov E, Méndez-Vidal MJ, Kozlov V, Alyasova A, Hong SH, Kapoor A, Alonso Gordoa T, Merchan JR, Winquist E, Maroto P, Goh JC, Kim M, Gurney H, Patel V, Peer A, Procopio G, Takagi T, Melichar B, Rolland F, De Giorgi U, Wong S, Bedke J, Schmidinger M, Dutcus CE, Smith AD, Dutta L, Mody K, Perini RF, Xing D, Choueiri TK; CLEAR Trial Investigators. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. 2021 Apr 8;384(14):1289-1300. doi: 10.1056/NEJMoa2035716. Epub 2021 Feb 13. PMID: 33616314.
- Motzer RJ, Escudier B, Burotto M, Powles T, Apolo AB, Bourlon MT, Shah AY, Porta C, Suárez C, Barrios CH, Richardet M, Gurney H, Kessler ER, Tomita Y, Bedke J, Scheffold C, Askelson M, Panzica J, Zhang J, van Kooten Losio M, Choueiri TK. Final analysis of nivolumab plus cabozantinib for advanced renal cell carcinoma from the randomized phase III CheckMate 9ER trial. Ann Oncol. 2025 Sep 23:S0923-7534(25)04714-3. doi: 10.1016/j.annonc.2025.09.006. Epub ahead of print. PMID: 40998092; PMCID: PMC12522107.
- Tannir NM, Albigès L, McDermott DF, Burotto M, Choueiri TK, Hammers HJ, Barthélémy P, Plimack ER, Porta C, George S, Donskov F, Atkins MB, Gurney H, Kollmannsberger CK, Grimm MO, Barrios C, Tomita Y, Castellano D, Grünwald V, Rini BI, Jiang R, Desilva H, Fedorov V, Lee CW, Motzer RJ. Nivolumab plus ipilimumab versus sunitinib for first-line treatment of advanced renal cell carcinoma: extended 8-year follow-up results of efficacy and safety from the phase III CheckMate 214 trial. Ann Oncol. 2024 Nov;35(11):1026-1038. doi: 10.1016/j.annonc.2024.07.727. Epub 2024 Aug 2. PMID: 39098455; PMCID: PMC11907766.
- Choueiri TK, Powles T, Albiges L, Burotto M, Szczylik C, Zurawski B, Yanez Ruiz E, Maruzzo M, Suarez Zaizar A, Fein LE, Schutz FA, Heng DYC, Wang F, Mataveli F, Chang YL, van Kooten Losio M, Suarez C, Motzer RJ; COSMIC-313 Investigators. Cabozantinib plus Nivolumab and Ipilimumab in Renal-Cell Carcinoma. N Engl J Med. 2023 May 11;388(19):1767-1778. doi: 10.1056/NEJMoa2212851. PMID: 37163623; PMCID: PMC10257898.