(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to a renal and urothelial carcinoma proffered paper session. Dr. Femke Brugers presented the randomized phase II NESCIO trial, which evaluated neoadjuvant immunotherapy in locally advanced clear cell renal cell carcinoma (ccRCC) at risk for recurrence or distant metastases.
Patients with locally advanced ccRCC are at high risk of developing disease recurrence or distant metastases following surgical resection.1 Adjuvant pembrolizumab improved disease-free (DFS) and overall survival (OS) in the phase III KEYNOTE-564 trial and is an approved standard of care option in this setting.2,3 Neoadjuvant immunotherapy has demonstrated promising efficacy with improved event-free survival in other cancer types.4-7 In ccRCC, the clinical benefit of neoadjuvant immunotherapy remains unclear and requires further systematic evaluation.
NESCIO is an investigator-initiated, randomized, non-comparative, open-label, two-stage, phase II trial, with the study design illustrated below. The main inclusion criteria are as follows:
- Histologically confirmed resectable ccRCC
- No history of distant metastases
- Intermediate- to high-risk disease:
- cT1b-cT2a grade 4 cN0M0
- cT2b grade 3-4 cN0M0
- cT3-4 any grade cN0M0
- cTany cN1 (fully resectable) cM0
- No prior immunotherapy and not on immunosuppressants
Eligible patients underwent 1:1:1 randomization to 2 neoadjuvant doses of:
- Arm A: Nivolumab (anti-PD-1) 360 mg Q3W
- Arm B: Ipilimumab (anti-CTLA-4) 1 mg/kg + nivolumab 3 mg/kg Q3W
- Arm C: Relatlimab (anti-LAG-3) 360 mg + nivolumab 360 mg Q3W
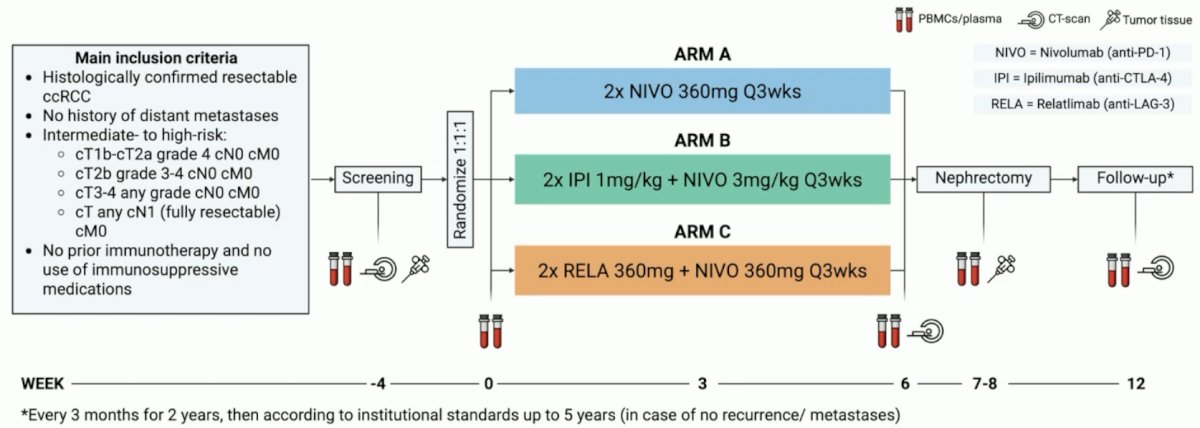
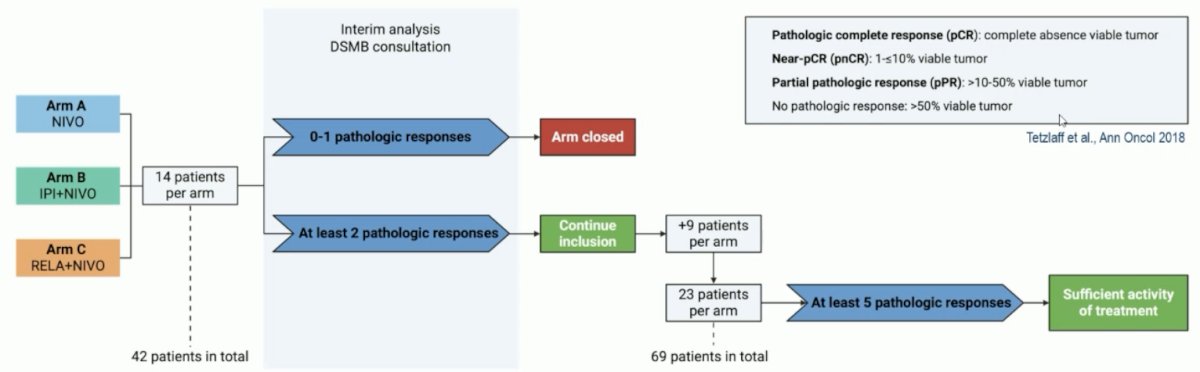
The primary endpoint was the pathologic response rate, defined as the proportion of patients demonstrating a complete, near complete, or partial pathologic response. A Simon’s two-stage design was used to detect a 30% partial or higher pathological response rate (≤50% viable tumor) with an alpha of 0.10 and a power of 85%.
During the 1st stage 14 patients per arm were included and evaluated for pathologic responses. If ≥2 responses were observed, then enrolment into the study arm was continued.
The secondary endpoints were:
- Safety, as measured by:
- The frequency of immune-related adverse events leading to a surgical delay of >2 weeks
- Surgical morbidity according to the Clavien Dindo classification
- Objective response rate (ORR): Defined as the proportion of patients demonstrating a complete or partial response, according to RECIST 1.1 at week 6
- Event-free survival (EFS), recurrence-free survival (RFS), rate of distant metastases, and local recurrences at 2 and 5 years after randomization or surgery, respectively
- Exploratory endpoints: in-depth translational research analyses
The baseline characteristics of the 1st 14 included patients in each arm are summarized below. Of note, 1 patient in the nivolumab arm was not evaluable for the primary endpoint of pathologic response, and, as such, an additional patient was included, leading to 15 patients in that arm. Dr. Burgers highlighted the following study characteristics:
- Excellent performance status: 79–93%
- cT3a: 71–93%
- cN1: 20–29%
- M1NED: 7% of patients in the nivolumab & nivolumab + ipilimumab arms
- Biopsy grade 1-2 disease: 80% of patients in the cohort
- Baseline tumor diameter: 10–12.3 cm

In the 1st stage, the primary endpoint of ≥2 pathologic responses was met for Arms B and C (2 responses each). The primary endpoint was not met for arm A of nivolumab monotherapy.

All patients received both treatment cycles. Surgery was delayed >2 weeks secondary to immune-related toxicity in 1 patient (nephritis secondary to nivolumab). There were two deaths:
- One before surgery, not treatment or disease related (nivolumab arm)
- One after surgery due to an adverse event, not treatment related (ipilimumab + nivolumab)
Grade ≥3 immune-related adverse events (e.g., nephritis, hepatitis, colitis, pneumonitis) were observed in 7%, 43%, and 14% of patients in Arms A, B, and C, respectively. Grade ≥3 surgery-related adverse events (e.g., hemorrhage, wound infection, dehiscence) were observed in 36% and 29% of patients in Arms B and C, respectively (none in Arm A). Grade ≥3 surgical complications according to the Clavien-Dindo classification were observed in 14% of patients in Arms B and C (none in Arm A).

The majority of patients (40/42) had radiologically stable disease at week 6. One patient in Arm B had a partial response, and one patient in Arm A had progressive disease.

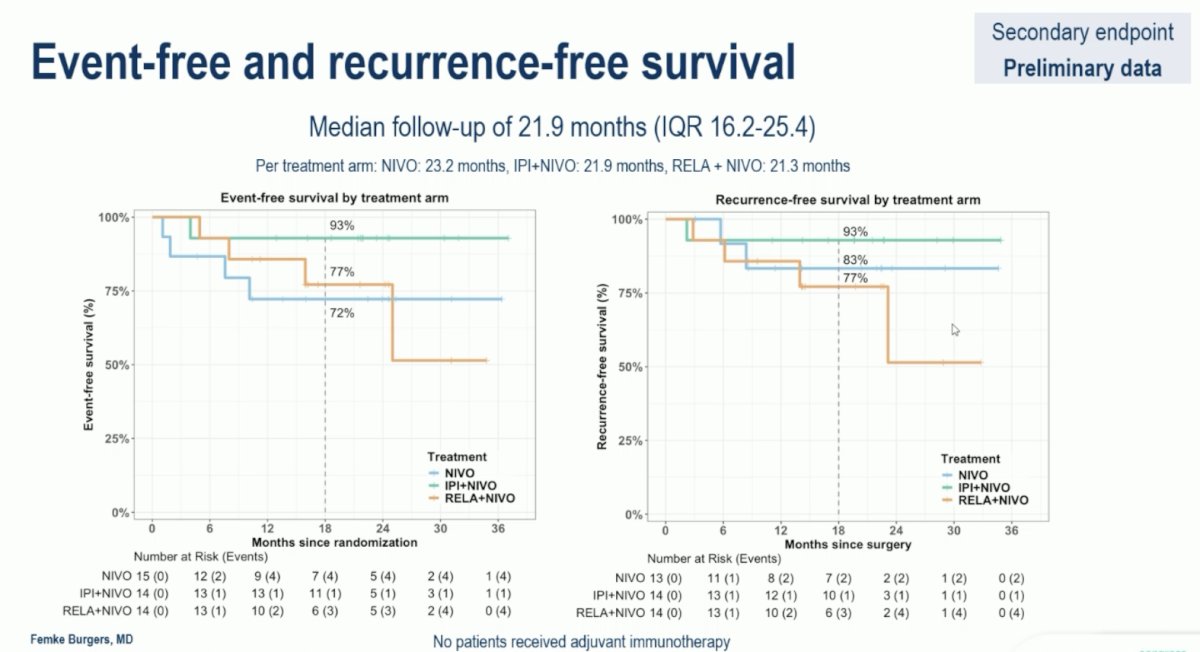
At a median follow-up of 22 months, the EFS and RFS rates by treatment arm were as follows:
- EFS at 18 months
- Arm B (Ipi + Nivo): 93%
- Arm C (Rela + Nivo): 77%
- Arm A (Nivo): 72%
- RFS at 18 months
- Arm B: 93%
- Arm A: 83%
- Arm C: 77%
To date, all 4 patients with a pathologic response have remained free of disease recurrence:
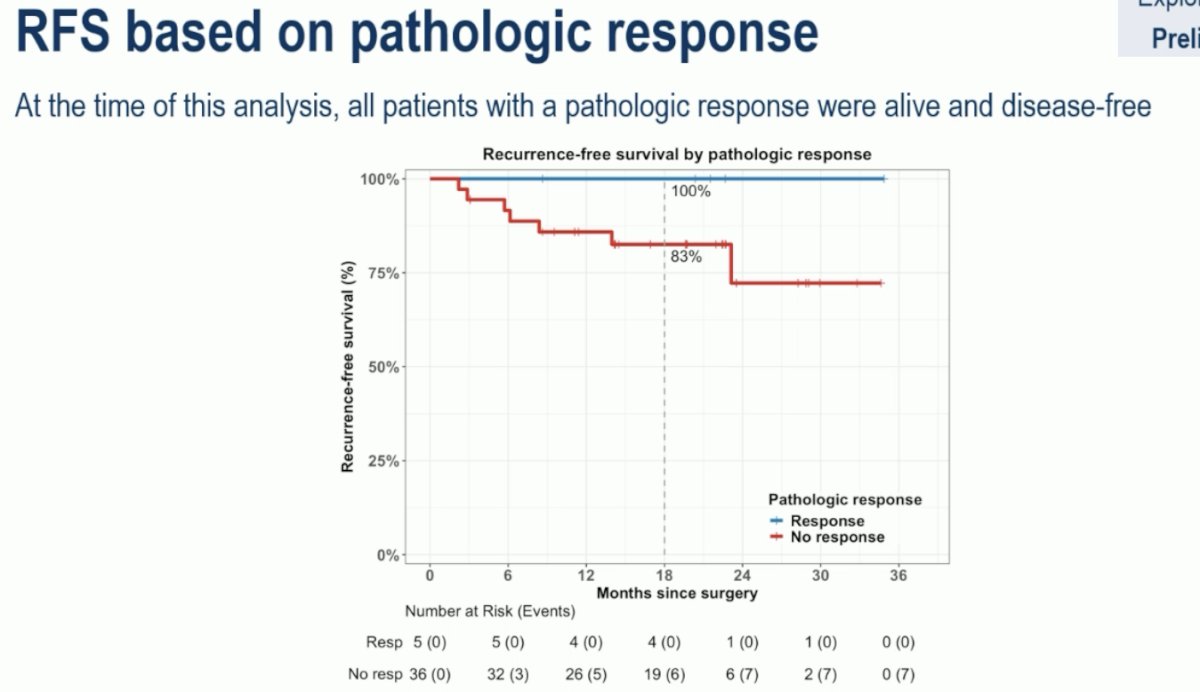
Dr. Burgers concluded as follows:
- (Ultra)short neoadjuvant ICI therapy for six weeks resulted in remarkable pathologic responses in a limited number of patients with intermediate- to high-risk ccRCC.
- In Stage 1, the primary endpoint of ≥2 pathologic responses was met in the IPI+NIVO (2 near-pCR) and RELA+NIVO (1 pPR and 1 pCR) treatment arms.
- Neoadjuvant ICI therapy showed acceptable safety profiles, with minimal impact on surgical timing.
- Preliminary survival results suggest favorable EFS and RFS, especially in the IPI+NIVO arm and in patients with a pathologic response.
Presented by: Femke Brugers, MD, Division of Medical Oncology, Netherlands Cancer Institute (NKI), Amsterdam, the Netherlands.
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: Phase II NESCIO Trial of Neoadjuvant Immunotherapy in Renal Cell Carcinoma - Femke Burgers
References:
- Marconi L, de Bruijn R, van Werkhoven E, et al. Adjuvant therapy in renal cell carcinoma: A systematic review and pooled analysis. Clin Genitourin Cancer. 2021; 19(6):518–527.
- Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021; 384(9):829–841.
- Choueiri TK, Powles T, Escudier B, et al. Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. N Engl J Med. 2024; 390(3):231–243.
- Blank CU, Rozeman EA, Versluis JM, et al. Neoadjuvant nivolumab and ipilimumab in resectable stage III melanoma. N Engl J Med. 2024; 390(5):411–423.
- Vos HJ, van der Leest P, Velds A, et al. Tumor microenvironment heterogeneity in renal cell carcinoma revealed by spatial transcriptomics. Nat Commun. 2021; 12(1):6532.
- van Dijk D, Sharma R, Nainys J, et al. Recovering gene interactions from single-cell data using data diffusion. Nat Med. 2020; 26(4):526–532.
- Chalabi M, Versluis JM, Rozeman EA, et al. Neoadjuvant immunotherapy leads to pathological responses in early-stage colon cancer. N Engl J Med. 2024; 390(6):519–530.