(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress, held in Berlin, Germany, was host to a renal and urothelial carcinoma proffered paper session. Dr. Rana McKay discussed perioperative immunotherapy strategies in RCC following the previous presentations of the RAMPRT and NESCIO trials.
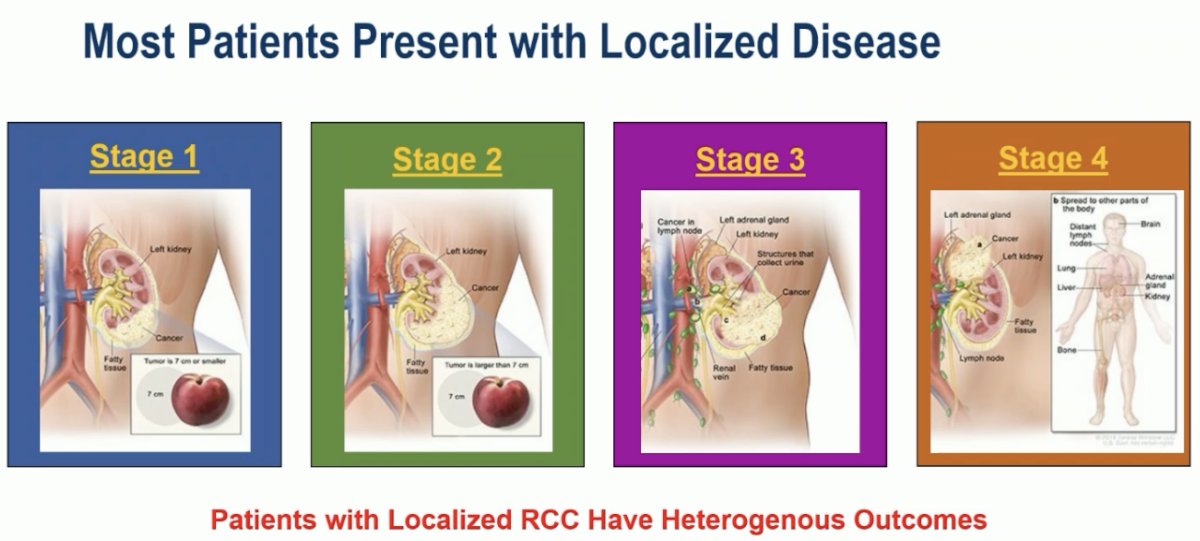
Most kidney cancer patients present with localized disease; however, these patients have heterogeneous disease outcomes.
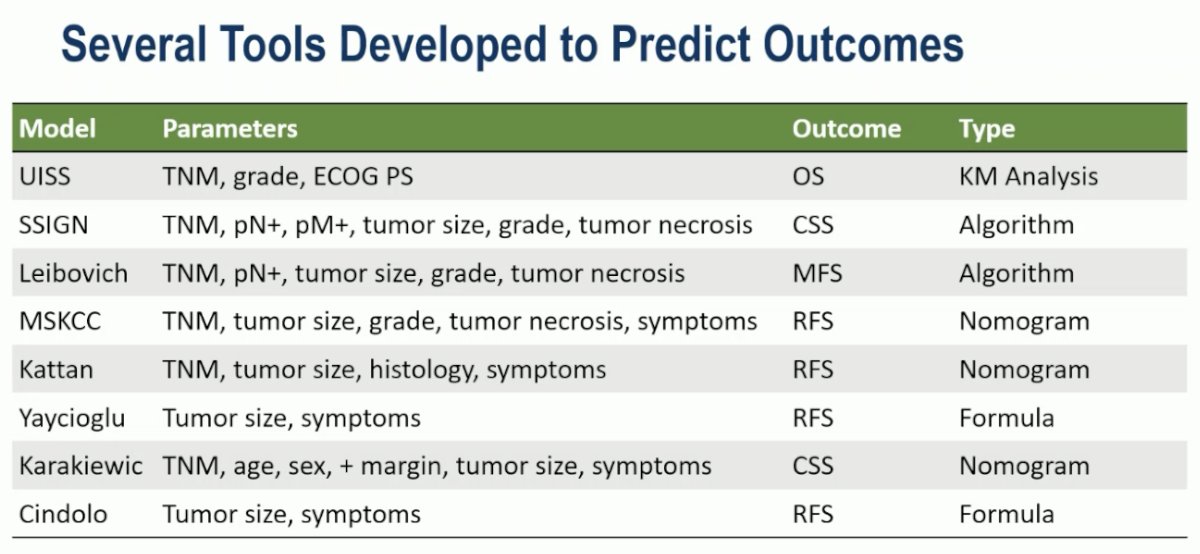
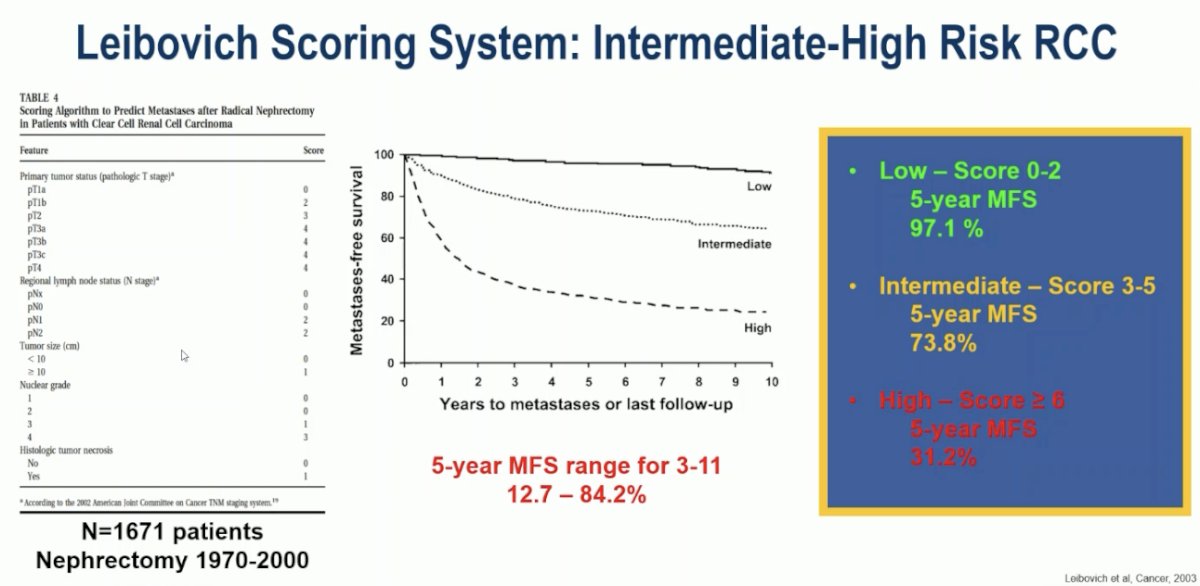
Several tools have been developed to accurately predict outcomes, including the Leibovich Scoring System that incorporates pathologic stage, regional nodal status, tumor size, nuclear grade, and presence/absence of histologic tumor necrosis:
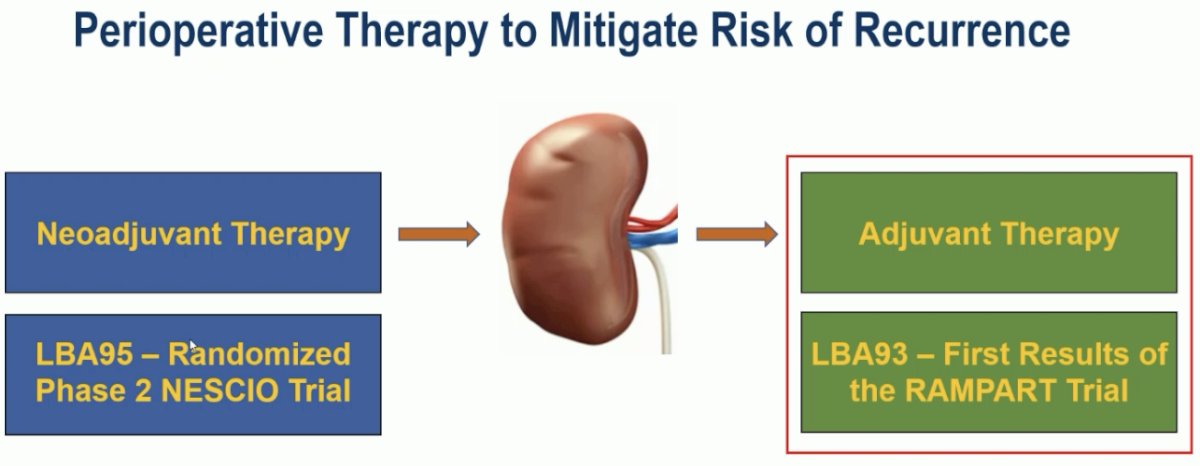
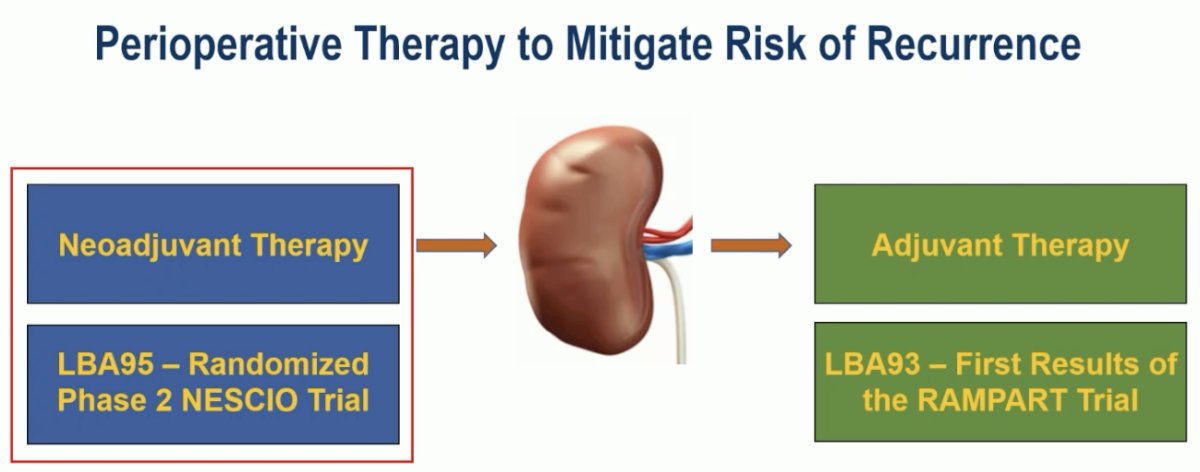
Perioperative therapy has been proposed to mitigate the risk of disease recurrence.
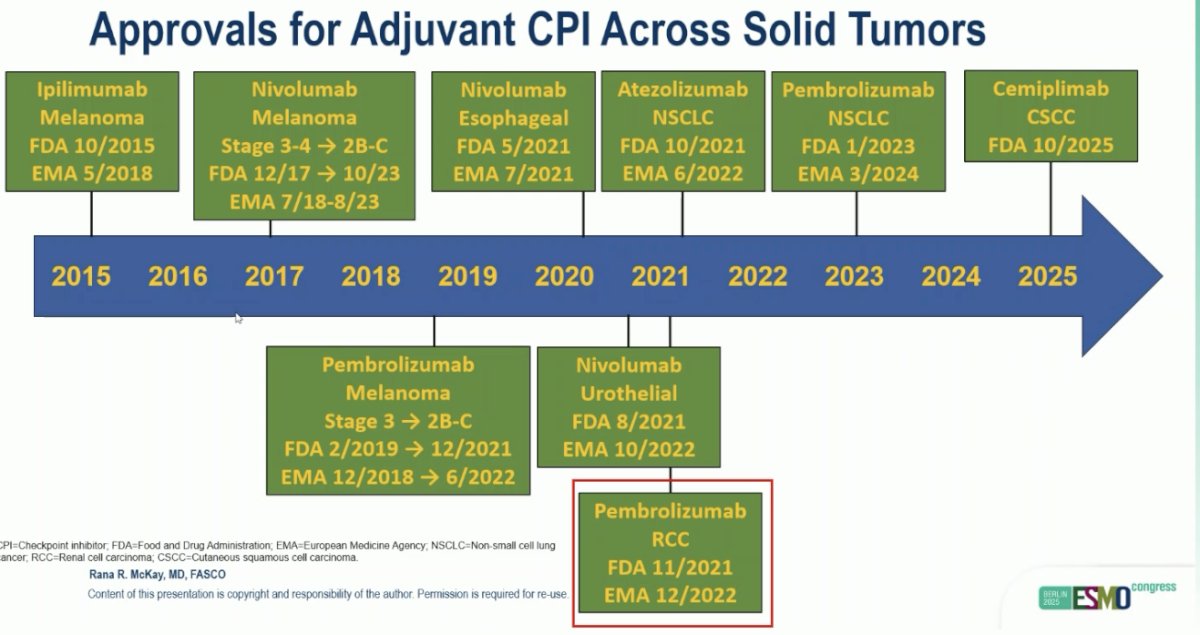
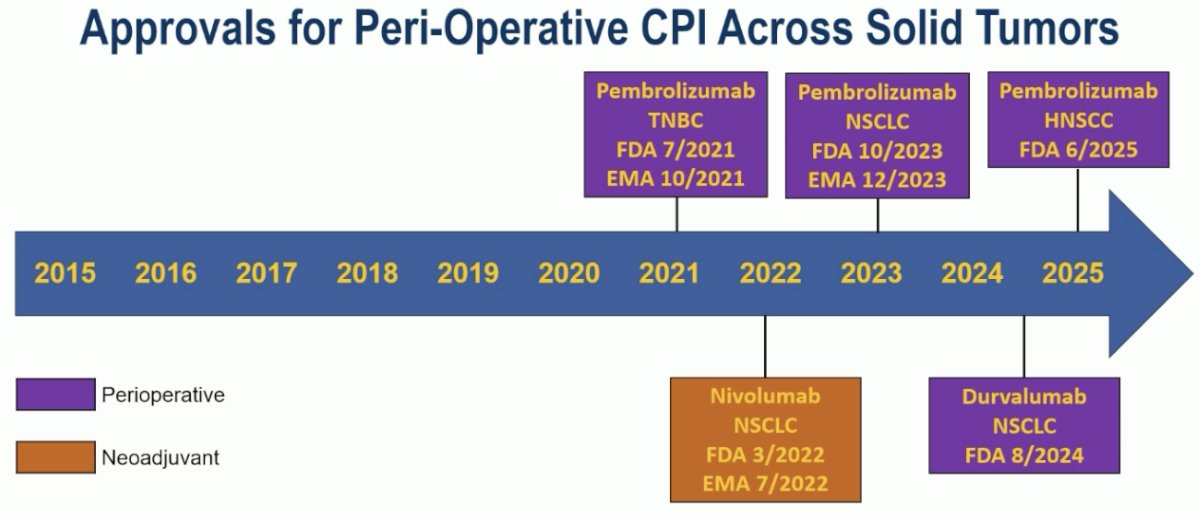
Is there an existing paradigm for the use of adjuvant immune checkpoint inhibitors (ICIs) across other solid malignancies? Summarized below is a historical timeline of all approvals for adjuvant ICIs across solid tumors, including pembrolizumab for RCC, based on the results of the KEYNOTE-564 trial.1
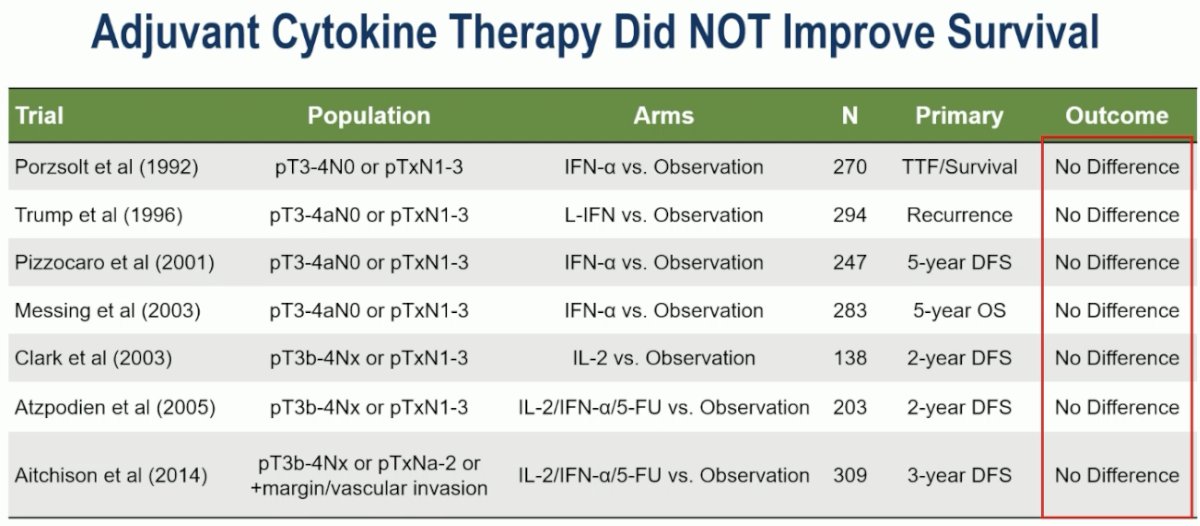
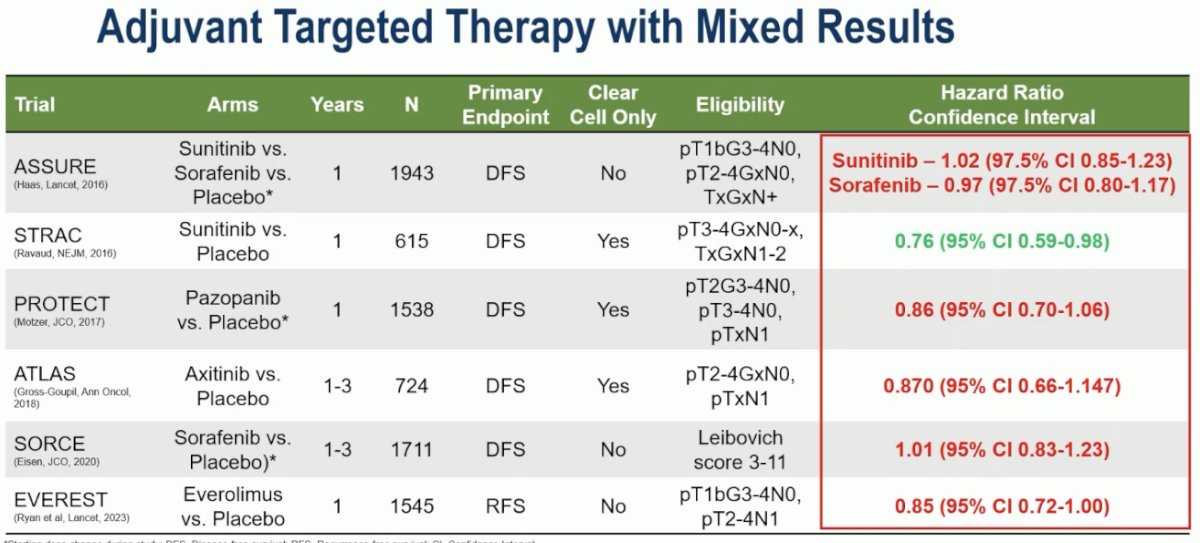
Focusing on the RCC disease space, Dr. McKay noted that trials of adjuvant cytokine therapy did not improve survival, and only the STRAC trial in the VEGFR-TKI era demonstrated a survival benefit.2
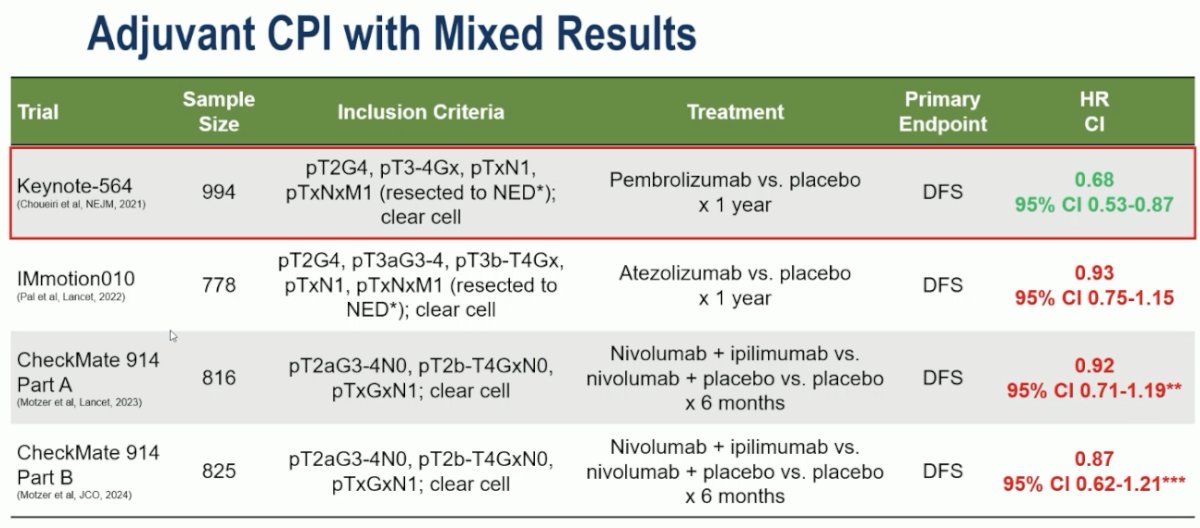
In the immunotherapy era, published trials to date have demonstrated inconsistent results, with only the KEYNOTE-564 trial demonstrating survival benefits.
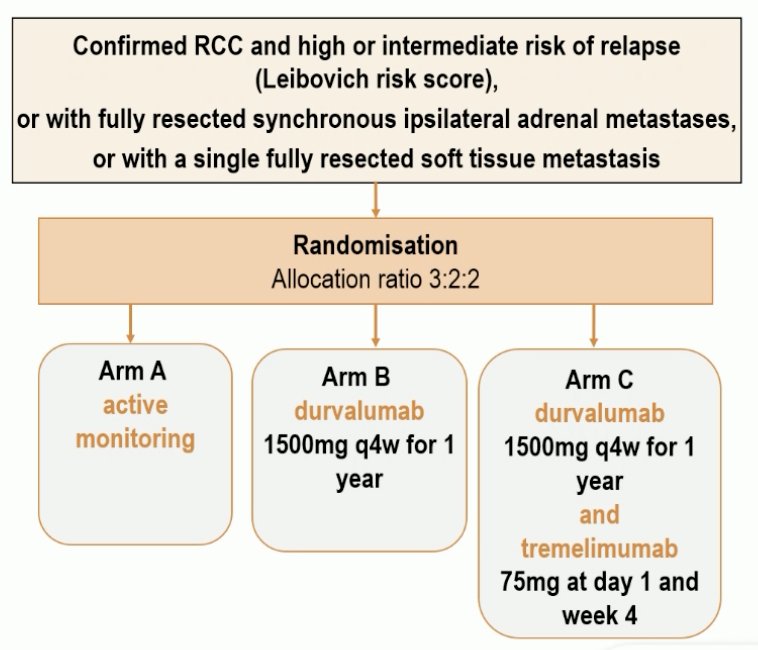
RAMPART employed an open label, multi-arm, multi-stage platform design. Eligible RCC patients at high or intermediate risk of relapse (Leibovich Score), including patients with a fully resected single metastatic disease site (i.e., M1 NED), were randomized in a 3:2:2 ratio to:
- Arm A: Active monitoring
- Arm B: Durvalumab monotherapy x 1 year
- Arm C: Durvalumab x1 year + tremelimumab (Day 1 & Week 4)
- Only 23% of patients completed all 13 durvalumab infusions (median: 8 infusions)
16% of patients had non-ccRCC. 45% and 50% of patients were at intermediate and high risks of recurrence, respectively. 5% of enrolled patients were M1 NED.
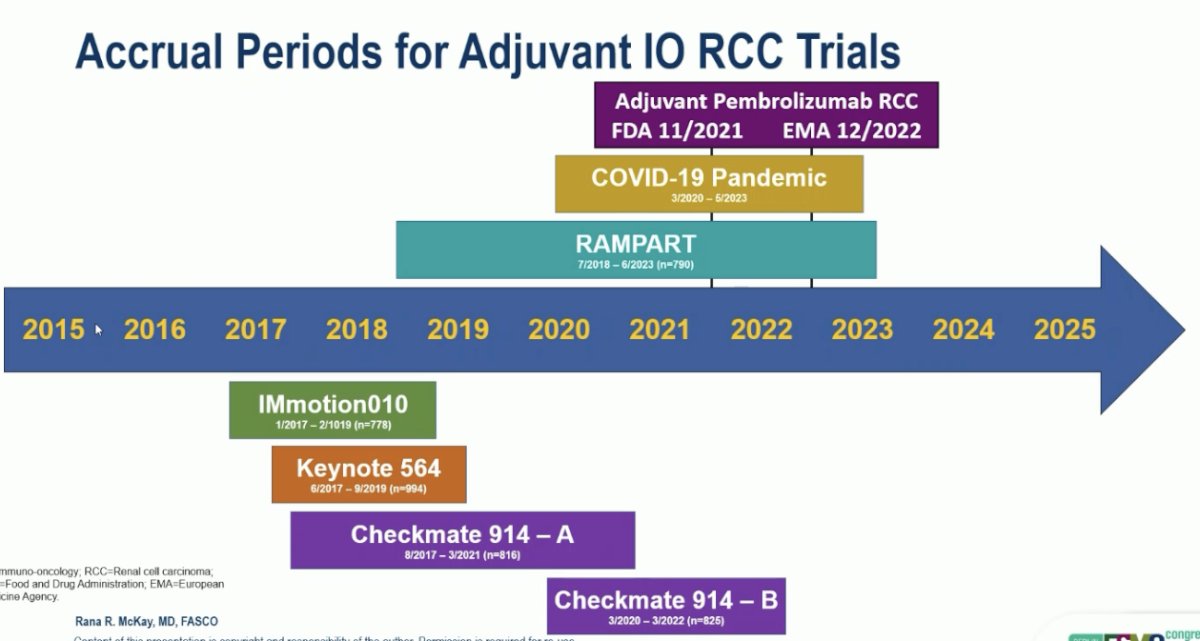
Dr. McKay noted that enrolment for this trial occurred much later compared to other analogous trials in this space – both the COVID-19 pandemic and the approval of pembrolizumab in this setting both significantly hampered accrual into this trial.
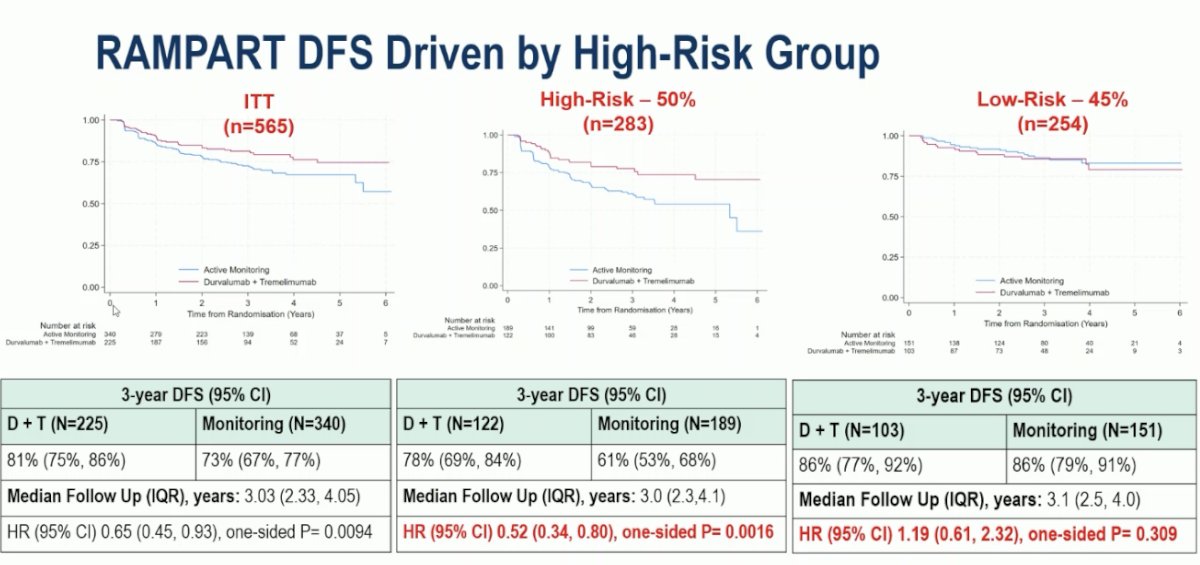
In the intent-to-treat (ITT) population, at a median follow-up of three years, the combination of durvalumab + tremelimumab significantly prolonged DFS, compared to active monitoring (3-year DFS: 81% vs 73%; HR: 0.65, 95% CI: 0.45–0.93, p<0.01). The benefit appeared to be limited to patients at high risk of disease recurrence (high-risk: HR=0.52, p=0.0016; intermediate-risk: HR=1.19, p=0.31):
While RAMPART was a positive study, Dr. McKay noted that many questions remain unanswered:
- What is the impact on overall survival?
- What about access to and receipt of subsequent treatments?
- What are the outcomes across clear cell and non-clear cell histologies?
- What are the rates of irreversible significant toxicity?
- What are the outcomes of Arm B (nivolumab) versus Arm C (active monitoring)?
- Can we identify patients who do not require treatment?
Next, Dr. McKay discussed the NESCIO trial:
Over the past 5 years, there have been 5 approvals of perioperative or neoadjuvant IO therapy across solid tumors.
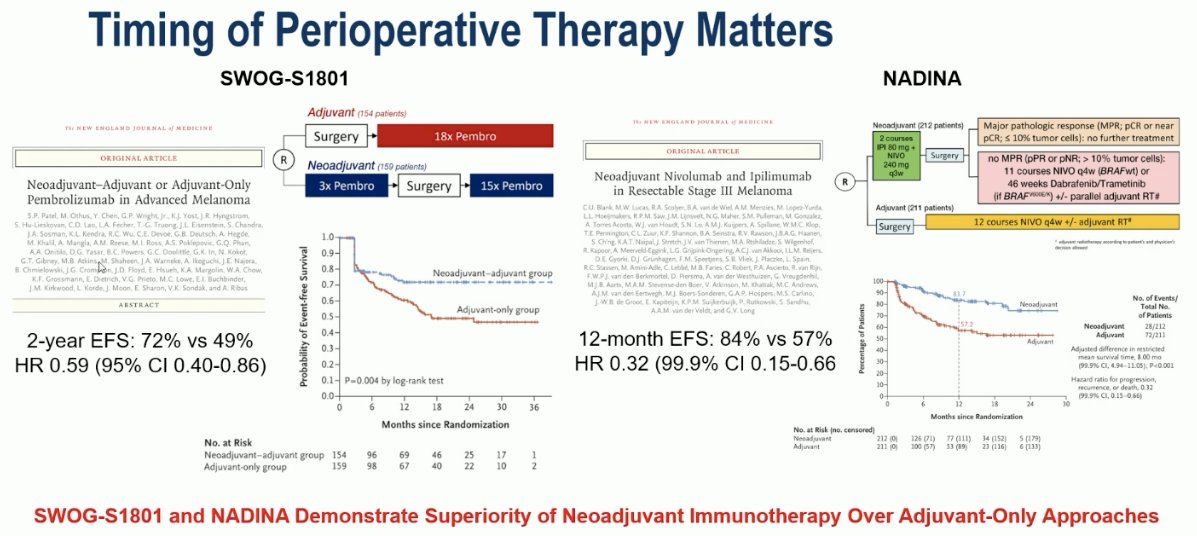
The timing of perioperative therapy (neoadjuvant versus adjuvant) remains a critical one, with both SWOG-S1801 and NADINA in the melanoma disease space demonstrating the superiority of neoadjuvant immunotherapy over adjuvant-only approaches.
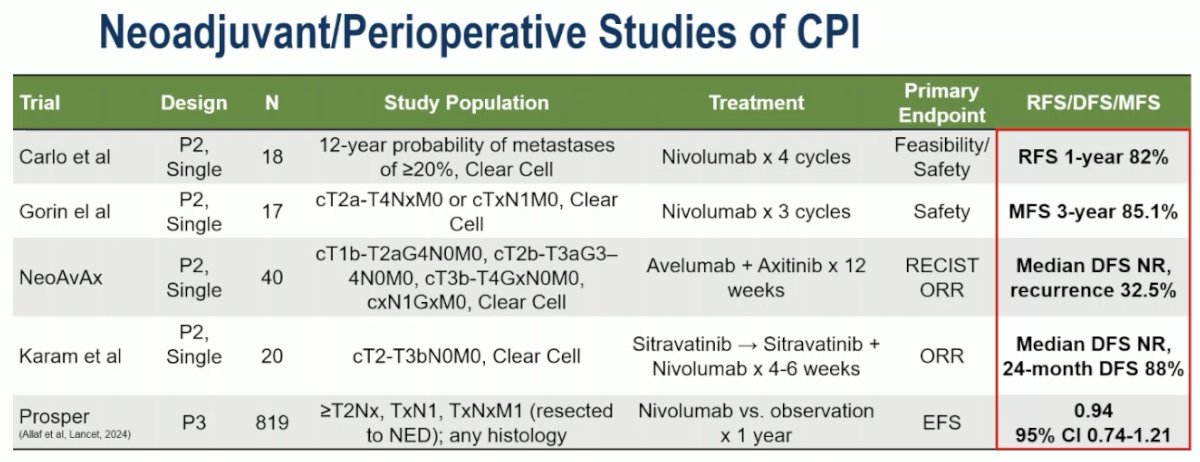
In the RCC disease space, the evidence for neoadjuvant therapy remains limited to small, single arm phase II studies with heterogenous populations and varying endpoints, making definitive conclusions difficult to attain.
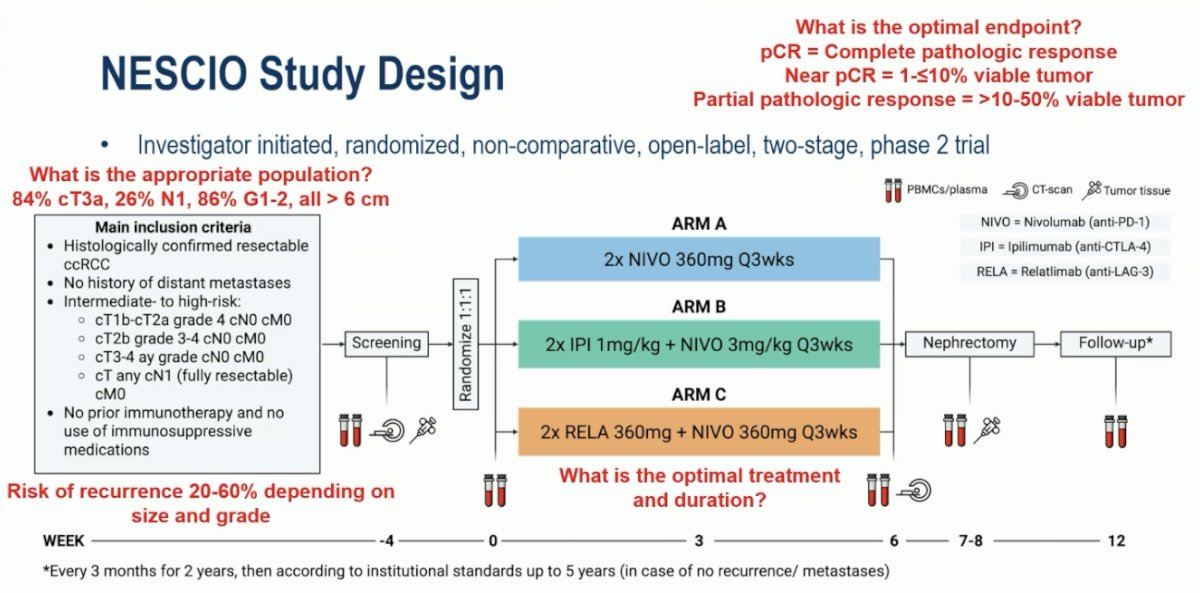
NESCIO is an investigator-initiated, randomized, non-comparative, open-label, two-stage, phase II trial that included patients with resectable ccRCC and intermediate- to high-risk disease. Eligible patients underwent 1:1:1 randomization to 2 neoadjuvant doses of:
- Arm A: Nivolumab
- Arm B: Ipilimumab + nivolumab
- Arm C: Relatlimab (RAG-3 inhibitor) + nivolumab
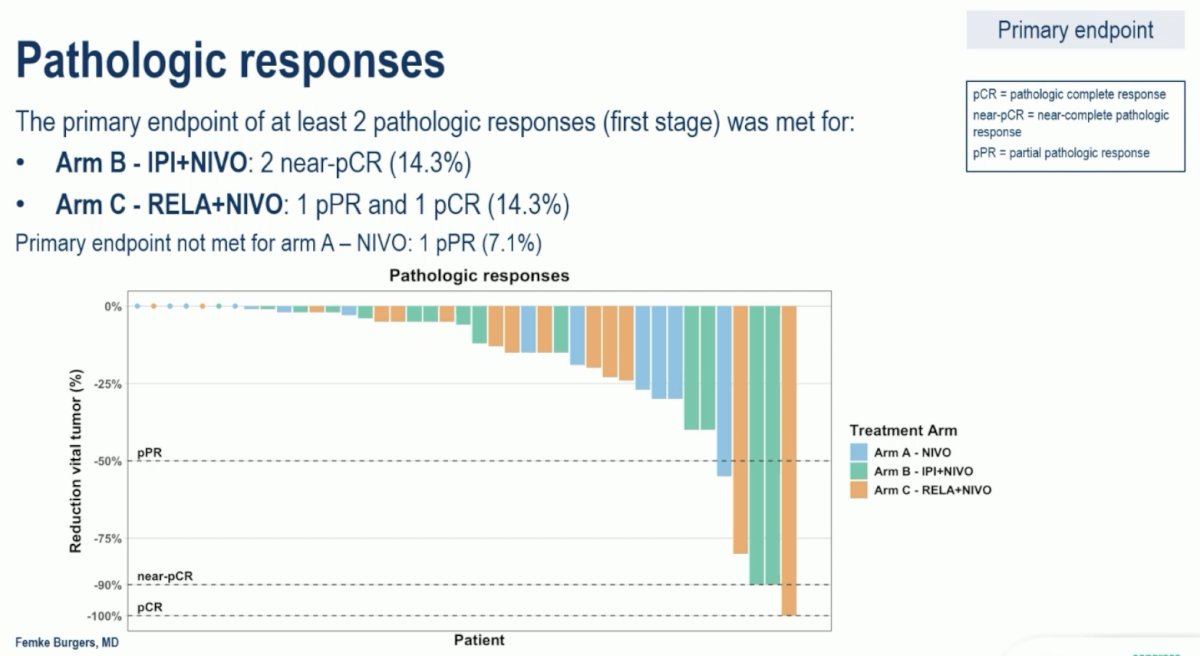
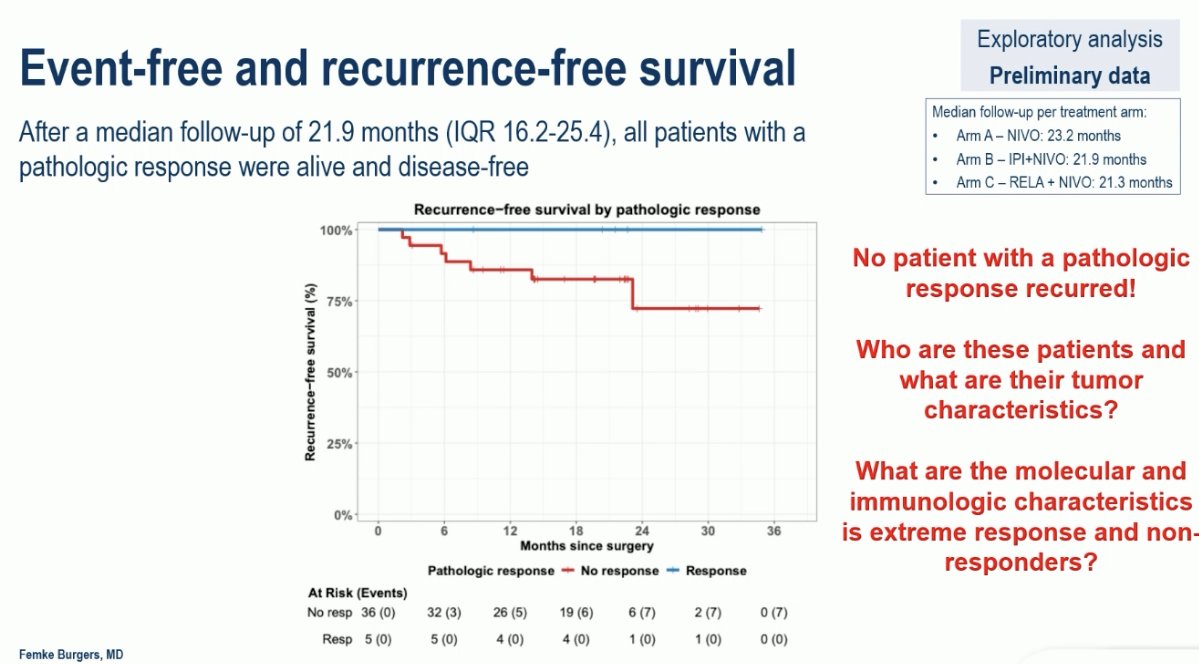
In the 1st stage, the primary endpoint of ≥2 pathologic responses was met for Arms B and C (2 responses each). The primary endpoint was not met for arm A of nivolumab monotherapy.
Dr. McKay raised the following questions regarding the NESCIO trial:
- Was this the appropriate patient population to evaluate this clinical question? 86% of patients had Grade 1-2 disease, and the risk of recurrence in this cohort ranged between 20% and 60% – a wide range.
- What is the optimal treatment and duration? Are 2 doses enough? Should it be 6 or 8?
- What is the optimal endpoint? Is it any pathologic response or complete/near-complete responses only?
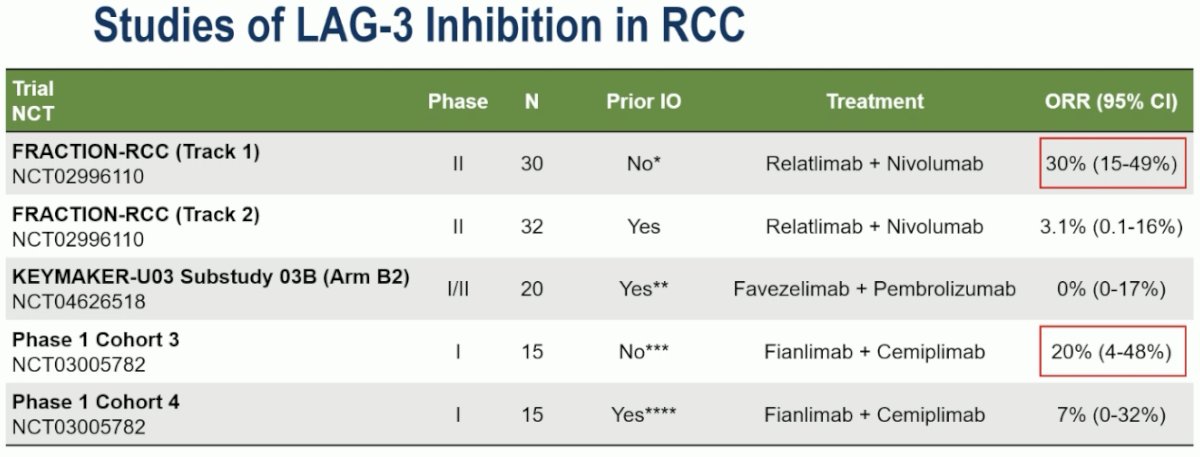
Several studies have evaluated LAG-3 blockade in advanced RCC. In the IO-naïve setting, LAG-3 blockade has been associated with ORRs in the 20-30% range but has no demonstrated activity in the post-IO setting.
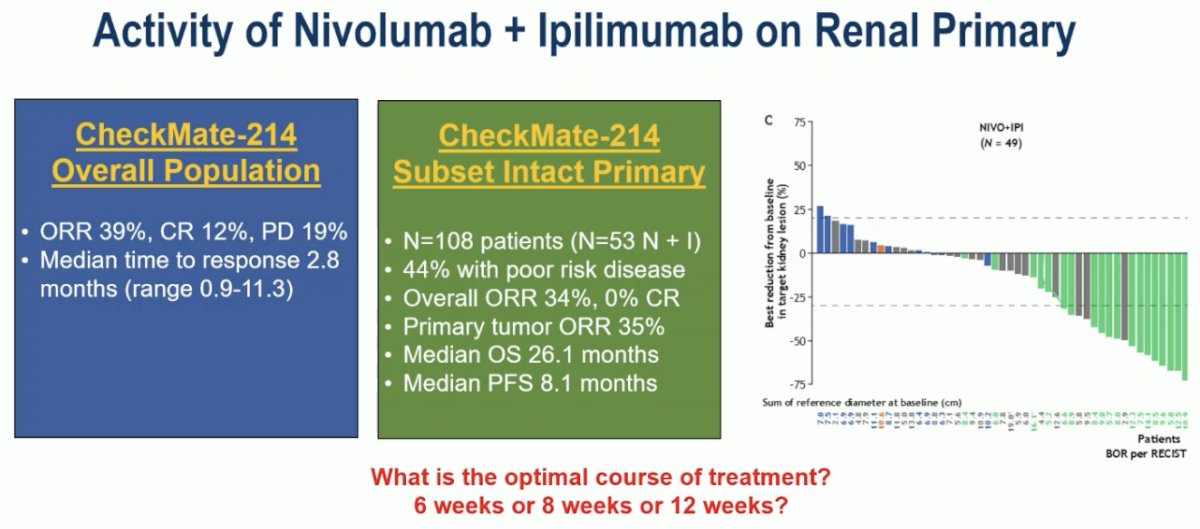
With regards to ipilimumab + nivolumab in the 1st line metastatic RCC setting, Dr. McKay noted that the ORR in the CheckMate-214 trial was 39%, with a median time to response of 2.8 months.5 Specifically, among patients with an intact primary, the ORR in the primary tumor was 35%. Dr. McKay argued that this suggests the need for longer neoadjuvant treatment courses to achieve meaningful responses.
With regards to the choice of the primary study outcome, the NESCIO criteria mirrored those of the INMC pathologic response criteria in melanoma.
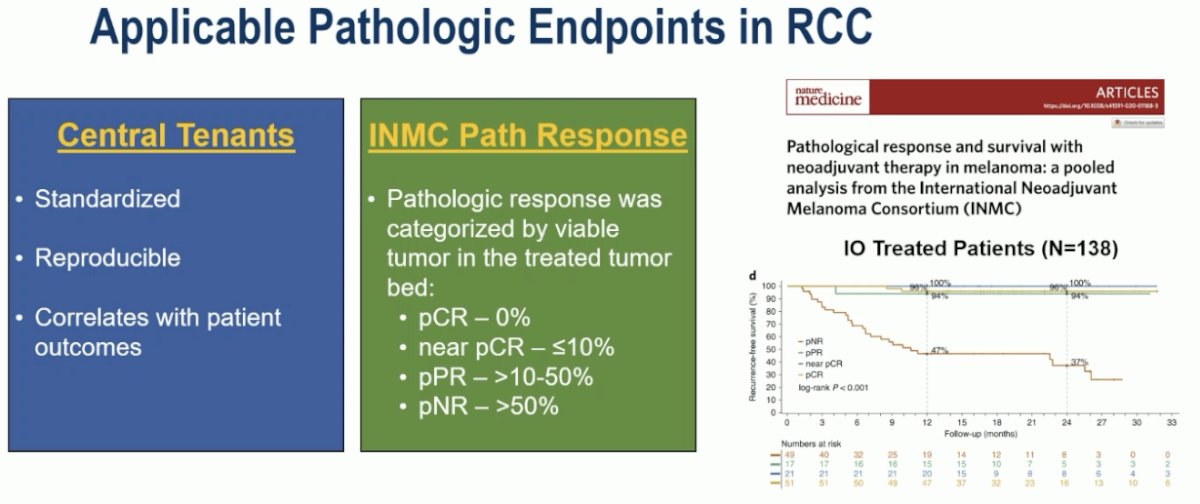
The choice of this primary endpoint is further supported by the results of this trial, whereby none of the 4 patients who experienced a pathologic response in the primary tumor experienced disease recurrence.
There is a clear need to standardize how we design trials of neoadjuvant therapy in RCC with several ‘call to action’ papers recently published.
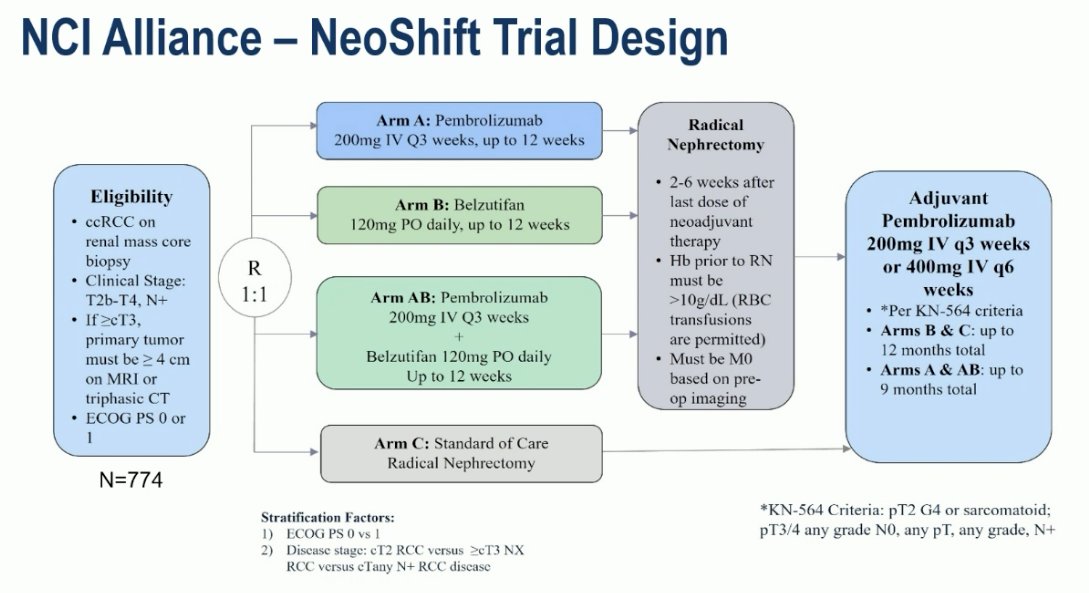
The NeoShift trial is evaluating neoadjuvant and adjuvant pembrolizumab, with or without belzutifan, in locally advanced ccRCC.
Dr. McKay concluded with the following take home messages:

Presented by: Rana McKay, MD, Professor, Department of Medicine, University of California, San Diego, CA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Choueiri TK, Tomczak P, Park SH, et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med. 2021; 385(8):683-694.
- Ravaud A, Motzer RJ, Pandha HS, et al. Adjuvant sunitinib in high-risk renal-cell carcinoma after nephrectomy. N Engl J Med. 2016; 375(23):2246–2254.
- Patel SP, Othus M, Chen Y, et al. Neoadjuvant–Adjuvant or Adjuvant-Only Pembrolizumab in Advanced Melanoma. N Engl J Med. 2023; 388(9):813-823.
- Blank CU, Mandala M, Ferrucci PF, et al. Neoadjuvant Nivolumab and Ipilimumab in Resectable Stage III Melanoma. N Engl J Med. 2024; 391(18):1675-1686.
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carinoma. N Engl J Med. 2018; 378(14):1277-1290.