(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress, held in Berlin, Germany, between October 17th and 21st, 2025, was host to a renal and urothelial carcinoma proffered paper session. Dr. Scott Haake presented OPTIC RCC, a phase II trial utilizing a novel RNAseq-based biomarker to evaluate the efficacy of cabozantinib plus nivolumab in cluster ½ metastatic clear cell renal cell carcinoma (ccRCC).
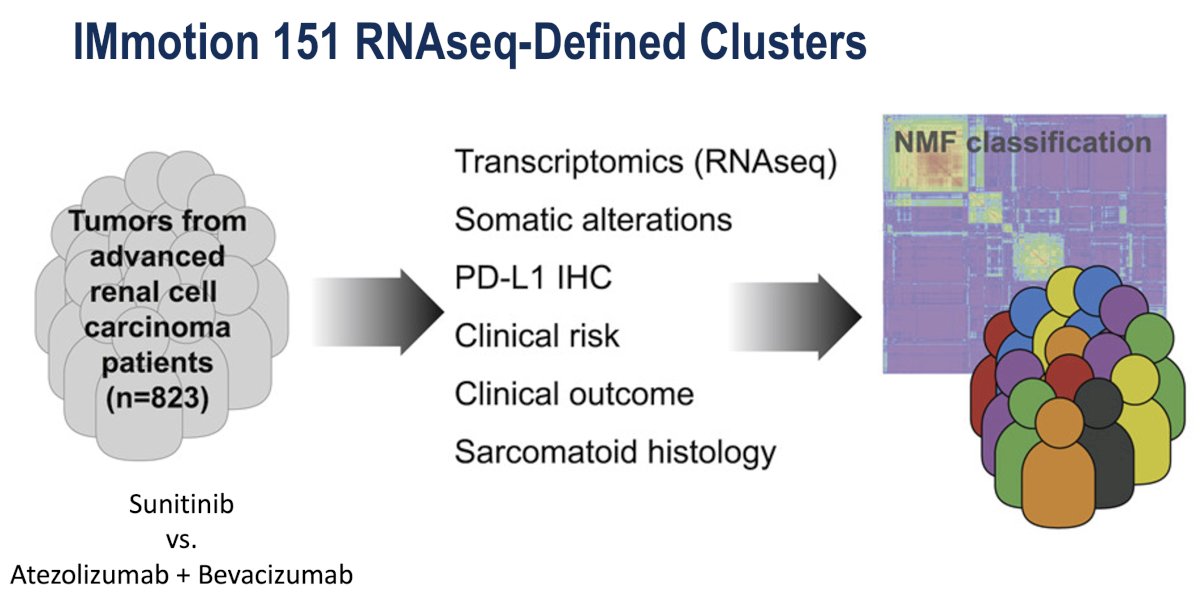
The origins of the OPTIC RCC study can be traced back to the IMmotion 151 study, a randomized phase III clinical trial comparing sunitinib to the combination of atezolizumab plus bevacizumab in previously untreated kidney cancer.1
Extensive translational and genomic characterization was performed on tumors from this study. In this report, Dr. Haake focused on the gene expression analyses. Unsupervised clustering was performed using the gene expression data, grouping similar tumors into "clusters".
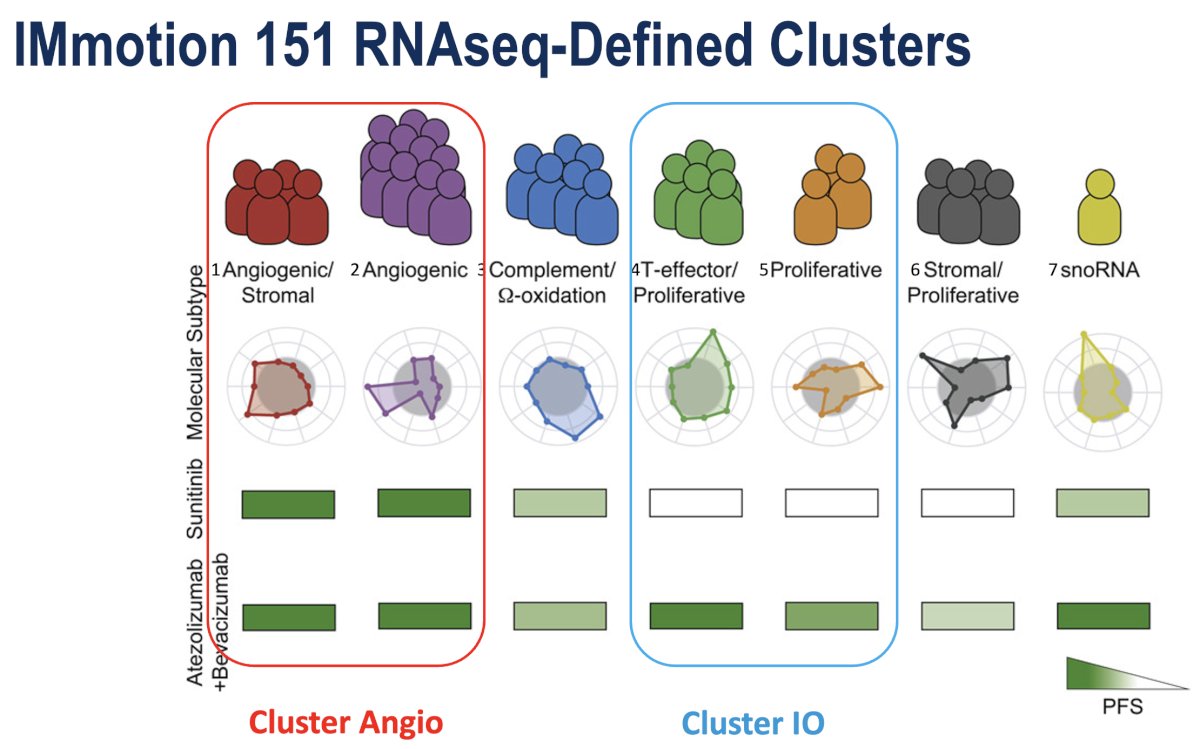
Shown below are the 7 clusters. Two of these clusters exhibited a strong angiogenic gene expression signature. Patients in these two clusters had favorable progression-free survivals (PFS) to both the control arm and the experimental arm, likely because both arms contained a potent anti-angiogenic therapy. These tumors are referenced as "cluster 1/2 or cluster angio".
Two of these clusters demonstrated superior response to the immune checkpoint inhibitor-containing experimental arm (relative to the control arm of sunitinib). These will be referred to as "cluster 4/5 or cluster IO".
Clusters 3 and 6 patients did not respond well to either arm, and cluster 7 was very small. Thus, these clusters were excluded moving forward.
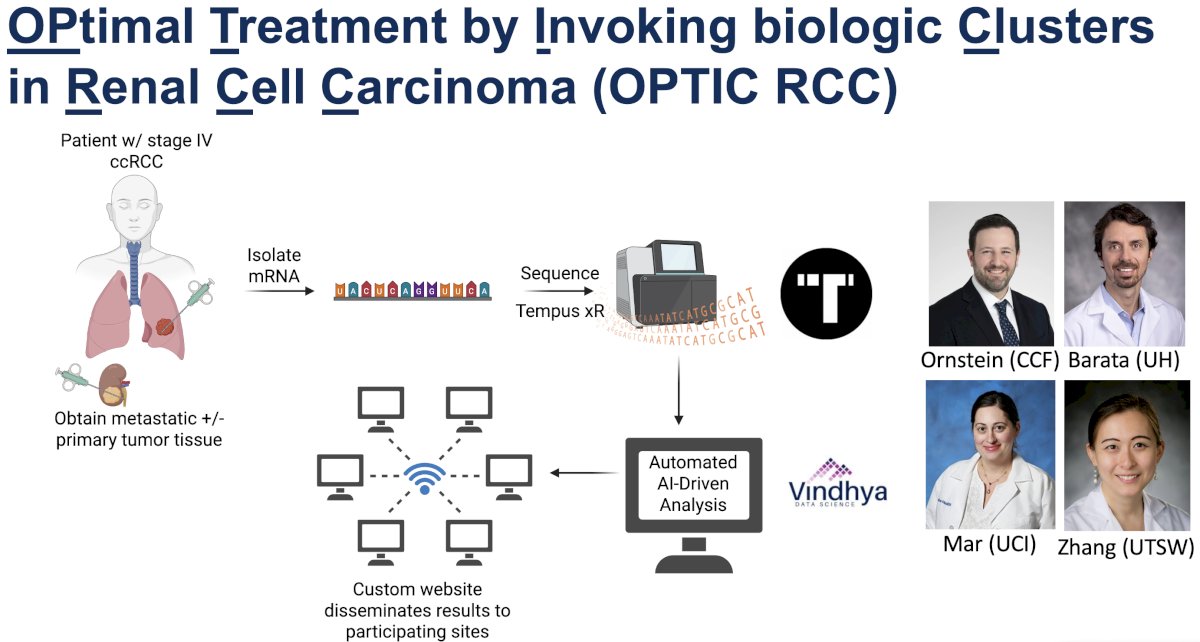
Based on these groups of clusters, the study investigators designed the OPtimal Treatment by Invoking biologic Clusters in Renal Cell Carcinoma (OPTIC) RCC study. The goal was to take these ”tumor clusters” or “gene expression signatures” that retrospectively correlated with drug response and prospectively evaluate their ability to enrich for drug response.
The key eligibility criteria were as follows:
- Metastatic ccRCC without prior systemic therapy in any setting
- Available tumor tissue for RENA sequencing/cluster prediction
- ECOG 0 or 1
Tumors were allocated to treatment arms based on cluster assignment:
- Cluster 1/2 patients were treated with cabozantinib plus nivolumab, a regimen with a potent anti-angiogenic drug (cabozantinib) as well as the anti-PD1 ICI nivolumab.
- The initial results of this arm were presented by Dr. Haake today.
- The primary endpoint is ORR.
- The study investigators hypothesized that this regimen would improve ORR by 20% (55% to 75%) relative to the historical control from CheckMate-9ER.2
- Cluster 4/5 was treated with the dual ICI regimen of ipilimumab plus nivolumab. This arm remains open to accrual.
- Clusters 3, 6, and 7 were excluded from the study.
Additional secondary endpoints are as follows:
- Progression-free survival (PFS)
- Depth of response >80% at 6 months
- Immune-related adverse events

Patients with stage IV ccRCC were required to have tissue from the metastatic site. mRNA was isolated, and RNA sequencing was performed by Tempus. Vindhya Data Science developed a cloud-based, automated, AI-driven data analysis algorithm that would process the data in real time without the need for an "on-call" bioinformatician. VDS also designed a custom website to disseminate the clustering results to participating sites in real time.
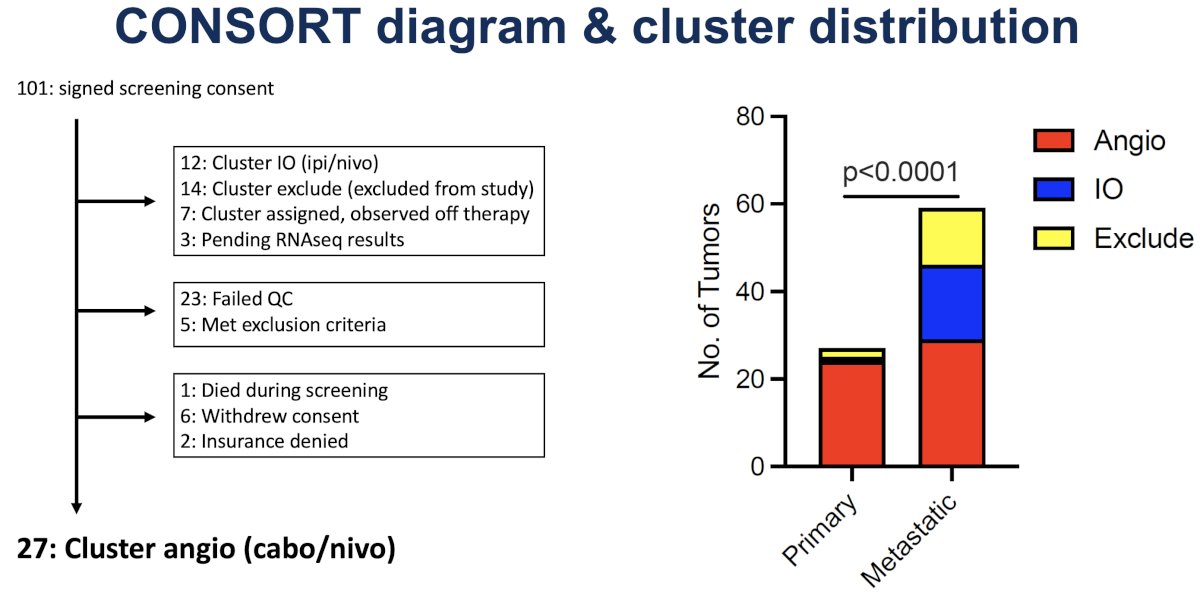
The CONSROT diagram and cluster distribution are illustrated below. 101 patients signed the screening consent. Twelve patients were assigned to cluster IO and thus treated on the ipi/nivo arm. Fourteen patients were assigned to cluster exclusion and were thus excluded from the study. Of note, some patients with cluster assignment have not started therapy yet.
Roughly 20% of patients failed quality control during tumor RNA sequencing, typically due to an inadequate tumor sample.
From these 101 patients, 27 patients are eligible, signed the consent, and went on the study. Interestingly, the study investigators observed significant discordance between primary and metastatic tissue cluster assignments. The primary tumors were biased towards the angiogenic signature, whereas the metastatic tumors displayed far more cluster diversity. Thus, after 17 patients were enrolled onto the cluster angio arm, the investigators transitioned to requiring metastatic tissue for cluster assignment so that OPTIC RCC would target the metastatic tumor biology.
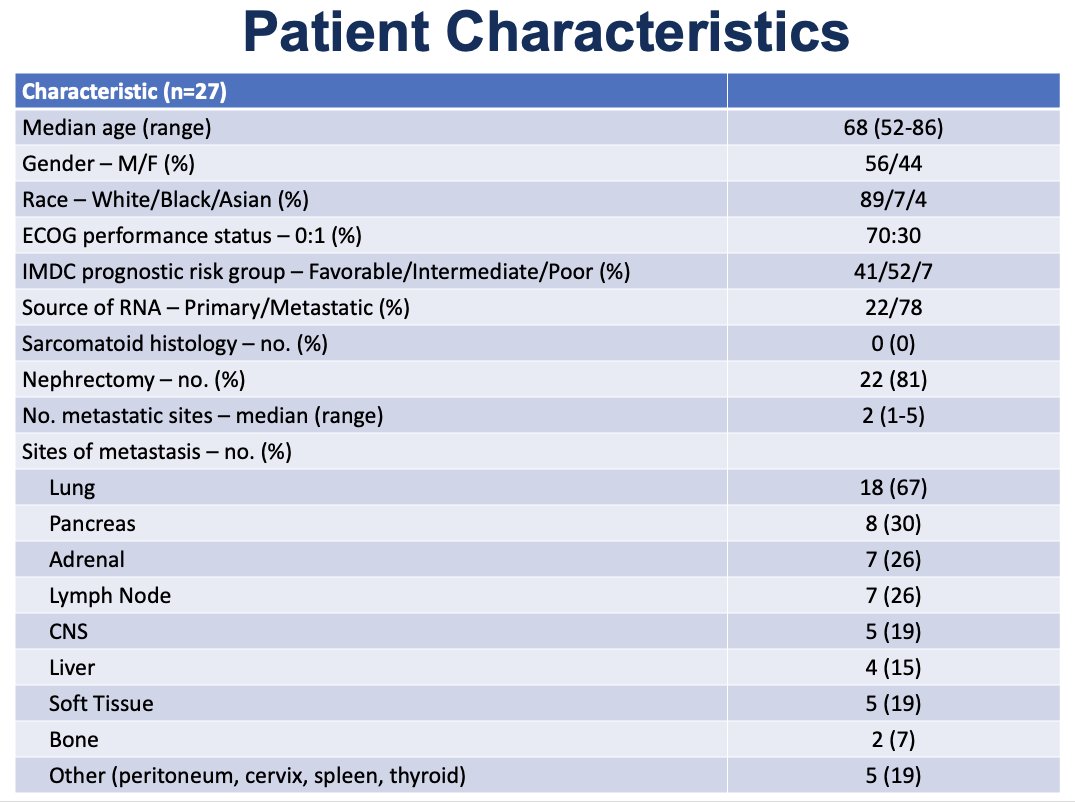
Summarized below are the baseline patient characteristics for the 27 patients enrolled in the cabozantinib/nivolumab arm. Dr. Haake noted that, overall, the patient characteristics were as expected for a cohort of patients with stage IV ccRCC.
IMDC risk classification was as follows:
- Favorable: 41%
- Intermediate: 52%
- Poor: 7%
None of the tumors harbored a sarcomatoid component. The sites of metastases were typical of advanced kidney cancer. However, higher proportions of pancreatic and adrenal metastases were observed relative to other front-line trials, which is expected based on our knowledge of angiogenic tumors.
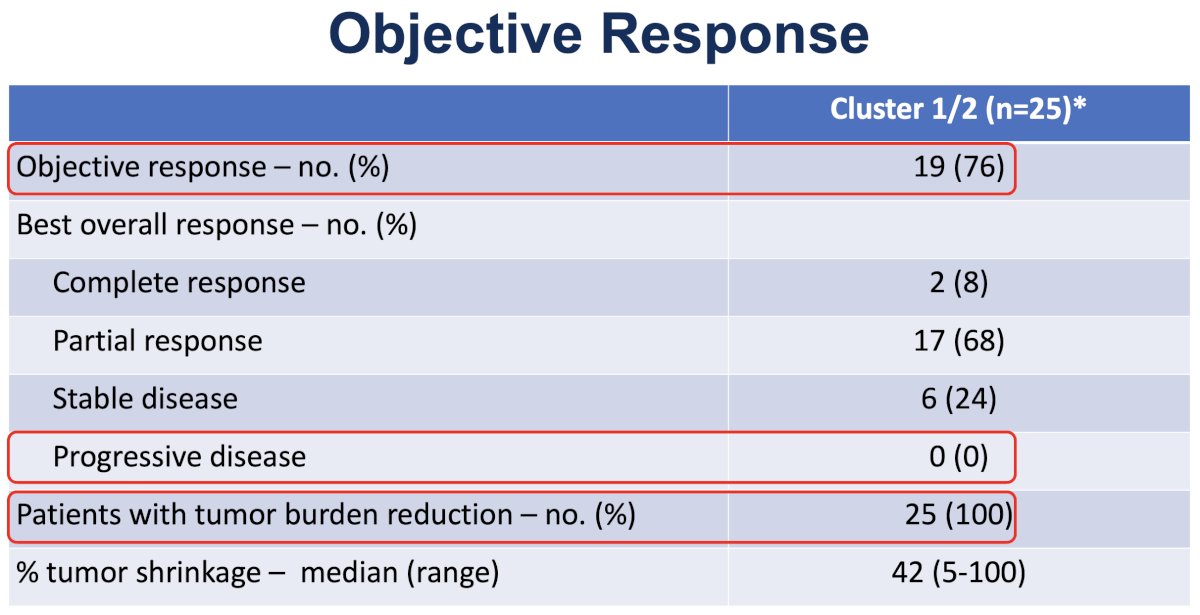
Of the 27 patients, 25 had post-baseline scans available. The ORR was 76% (primary endpoint met):
- CR: 8%
- PR: 68%
- SD: 24%
- PD: 0%
All patients exhibited some reduction in tumor burden. The median follow-up is relatively short at ~11 months. 17 of 27 patients remain on study.
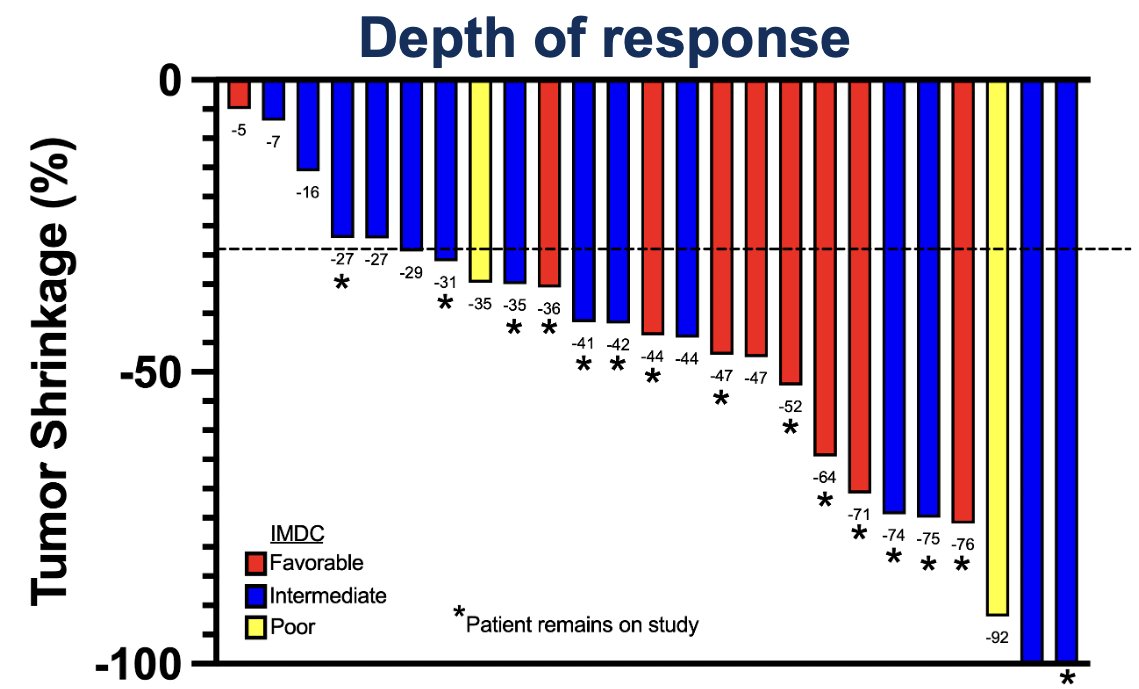
The waterfall plot demonstrating depth of response is illustrated below. Of the 6 patients with SD, 3 just missed the criteria for objective response, but were very close (27%, 27%, and 29%). 76% of patients met the RECIST criteria for objective response. Importantly, many of the best responses were observed in intermediate and poor risk disease (including both CRs).
With regards to operational logistics, Dr. Haake commented as follows: “In terms of operational logistics, we improved over time and then plateaued. We optimized the turnaround time for our sequencing and data analysis relatively early in the study. Thereafter, the rate-limiting step was typically acquisition of tissue (especially when biopsies and/or surgical samples were obtained at outside facilities and needed to be shipped to Vanderbilt before Tempus submission).”

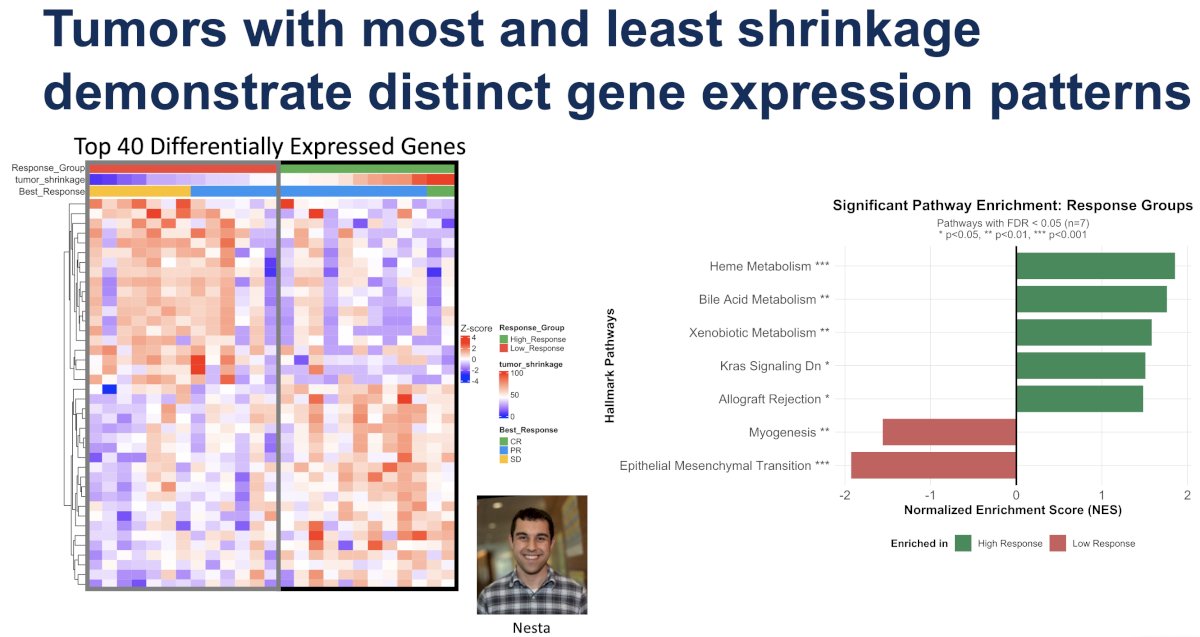
While all patients exhibited a reduction in tumor burden and all tumors exhibited strong angiogenic gene expression signatures, the study investigators compared gene expression patterns from tumors with the most and least shrinkage. Preliminary results demonstrated distinct gene expression patterns in tumors with the most versus least tumor shrinkage.
Looking at pathways that include these differentially expressed genes, Dr. Haake noted that several metabolic pathways were enriched in the tumors with the most shrinkage and increased epithelial-to-mesenchymal transition expression correlated with the least tumor shrinkage. These translational studies are preliminary and will be further refined.
Dr. Haake concluded as follows:
- Prospective investigation of tissue-based RNAseq biomarkers to guide therapy is operationally feasible in a front-line metastatic ccRCC population
- Primary and metastatic tumors can exhibit different gene expression signatures, requiring metastatic tumor biopsies for a biomarker-driven study
- Selection of patients exhibiting an angiogenic gene expression signature enriches for clinical outcome to cabozantinib + nivolumab
- A high objective response rate, reduction of tumor burden in all patients, and lack of primary progressive disease were observed
- Time-to-event endpoints, such as PFS and duration of response, will require additional follow-up
Presented by: Scott Haake, MD, PhD, Assistant Professor of Medicine, Division of Hematology Oncology, Vanderbilt University Medical Center, Nashville, TN
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Related content: Feasibility of Using an RNA-Seq Biomarker to Assign Therapy in the OPTIC RCC Trial - Pedro Barata
- Motzer RJ, Powles T, Atkins MB, et al. Final overall survival and molecular analysis in IMmotion151, a phase III trial comparing atezolizumab plus bevacizumab vs sunitinib in patients with previously untreated metastatic renal-cell carcinoma. JAMA Oncol. 2022; 8(2):275-280.
- Motzer RJ, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021; 384(9):829–841.