(UroToday.com) The 2025 ESMO annual meeting featured a kidney cancer mini oral session and a presentation by Dr. Sara Coca Membribes discussing the final efficacy data and biomarker analysis from the clear cell cohort of CALYPSO. Ipilimumab + nivolumab is standard of care in metastatic clear cell RCC (intermediate and poor risk); however, there is currently no data comparing PD-1/PD-L1 monotherapy with or without CTLA-4 inhibition in this setting.
MET inhibition in clear cell RCC is supported by agents such as cabozantinib, which targets both VEGFR and MET. Savolitinib (a selective MET inhibitor) has established activity in papillary RCC.
The predictive role of PD-L1 biomarker expression remains unclear in RCC, and tumor cell staining and combined positive score (CPS) have been explored as biomarkers, with exploratory data favoring tumor cell staining. Additionally, KIM-1 is a promising biomarker in RCC, reflecting disease burden and treatment response.
CALYPSO is a phase II trial evaluating durvalumab, savolitinib, and tremelimumab in previously treated advanced RCC. In this study, these agents were evaluated alone or in combination. Dr. Membribes and colleagues previously reported the interim analysis of response rates and progression-free survival at ASCO 2022. This analysis, presented at ESMO 2025, reported the final overall survival analysis in the clear cell RCC cohort.
This was a multinational, open-label, randomized phase II study in patients with advanced RCC previously treated with VEGF-targeted therapy but naïve to immune checkpoint and MET inhibitors. Patients were randomized to durvalumab, savolitinib, durvalumab + tremelimumab, or durvalumab + savolitinib:
The primary endpoint was confirmed response rate with a threshold of ≥50% for further evaluation, which was not achieved. DNA alterations were assessed using Foundation One. KIM1, RNA-based analysis, and PD-L1 in tumor cells, immune cells, and combined with durvalumab and durvalumab + savolitinib/durvalumab + tremelimumab are ongoing.
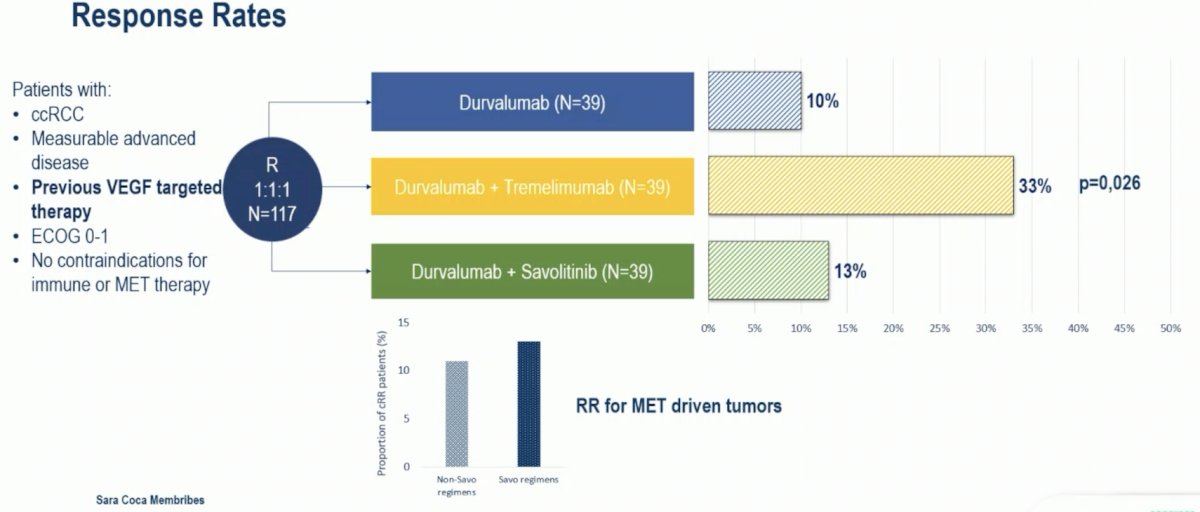
From 2017 to 2021, 138 patients were randomized to durvalumab (n = 39), savolitinib (n = 21), durvalumab + tremelimumab (n = 39), and durvalumab + savolitinib (n = 39). The median age was 62 years (range: 28-85). The confirmed response rates at the interim analysis presented at ASCO 2022 for durvalumab were 10%, durvalumab + tremelimumab was 28%, and durvalumab + savolitinib were 13% (savolitinib was 5%, closed early):

The median duration of response with durvalumab was 9.8 months, for durvalumab + tremelimumab was 19.4 months, and for durvalumab + savolitinib was 13.3 months. With a minimum follow-up of 40 months, the response rate for durvalumab was 10%, for durvalumab + tremelimumab was 33% and for durvalumab + savolitinib was 13%:
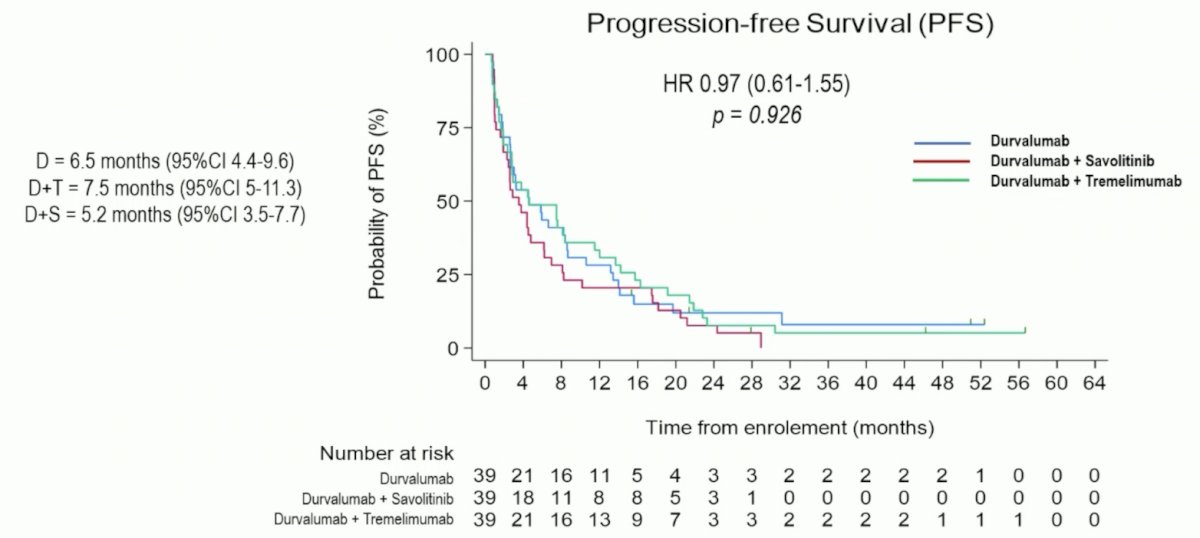
The final progression-free survival analysis showed no difference between the three groups (HR 0.97, 95% CI 0.61-1.55):
The median overall survival for durvalumab was 25.8 months, for durvalumab + tremelimumab was 24.2 months, and for durvalumab + savolitinib was 16.3 months (HR 0.88, 95% CI 0.51-1.51):
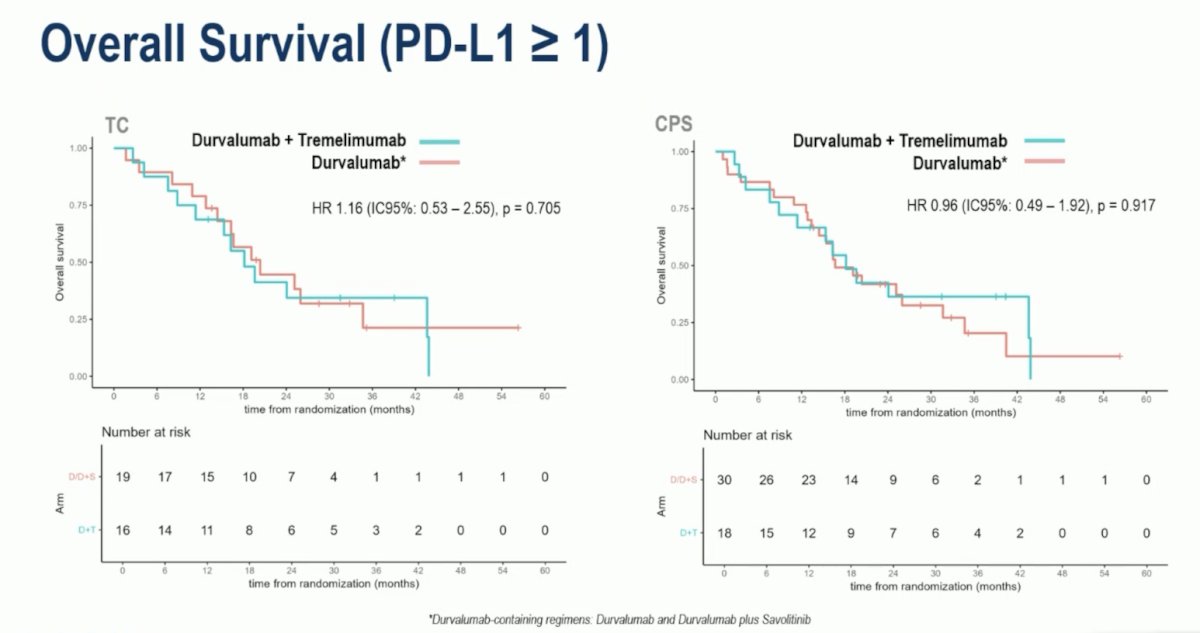
Exploratory PD-L1 analysis for progression-free survival also showed no difference between durvalumab + tremelimumab versus durvalumab:

Similar findings were noted for overall survival comparing durvalumab + tremelimumab versus durvalumab:
Dr. Membribes noted that KIM-1 correlated with nephrectomy and IMDC score in clear cell RCC:
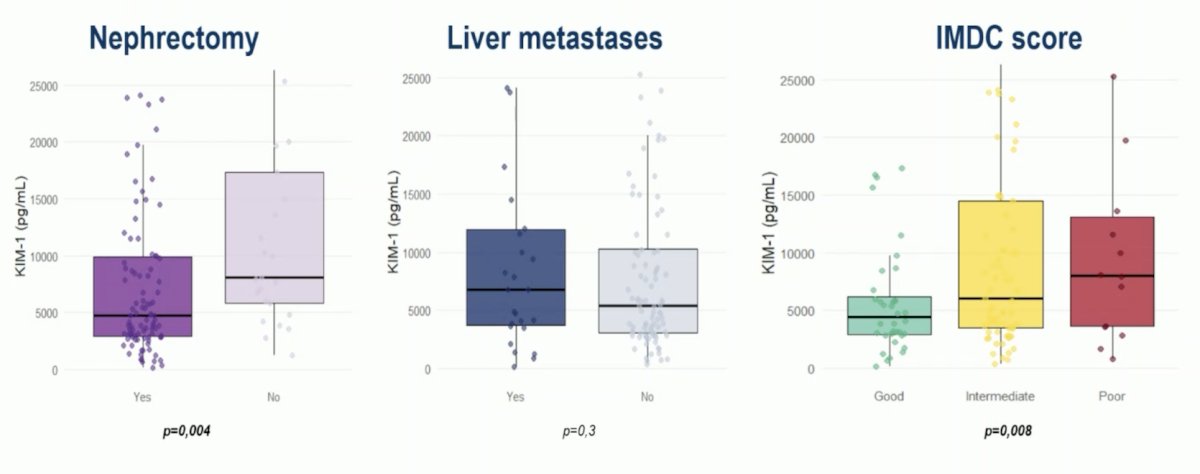
Also, a significant KIM-1 reduction was found with durvalumab + tremelimumab:

Dr. Membribes concluded her presentation discussing the final efficacy data and biomarker analysis from the clear cell cohort of CALYPSO with the following take-home points:
- In this final analysis, with a minimum follow-up of 40 months, durvalumab plus tremelimumab showed higher response rates and a greater reduction in KIM-1 levels
- The improvement in response did not translate into a clear benefit in progression-free survival or overall survival
- No clear enrichment of response was observed according to PD-L1 status (tumor cell staining or CPS)
- Study limitations include the sample size and the incomplete availability of PD-L1 tissue samples
- All patients had received prior VEGF therapy, which is no longer considered standard of care, limiting applicability to the first-line or adjuvant settings
- The comparison of durvalumab versus durvalumab + tremelimumab will be further evaluated in RAMPART, and the ongoing CARE1 trial is prospectively exploring the role of PD-L1 in treatment selection for metastatic clear cell RCC
- The results of this phase II trial may help inform these randomized phase III trials
Presented by: Sara Coca Membribes, Barts Cancer Institute, London, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.