(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma trials in progress session and a presentation by Dr. Petros Grivas discussing INTerpath-011, a phase 2 study of intismeran autogene (V940/mRNA-4157) + BCG versus BCG alone for high-risk non muscle invasive bladder cancer. TURBT followed by intravesical BCG is the standard of care for patients with treatment-naive high-risk non muscle invasive bladder cancer.
However, many patients develop disease recurrence and novel therapies are needed to improve outcomes. Intismeran autogene is a personalized neoantigen therapy being evaluated in a number of solid tumors, including muscle-invasive bladder cancer, with the following mechanism of action:

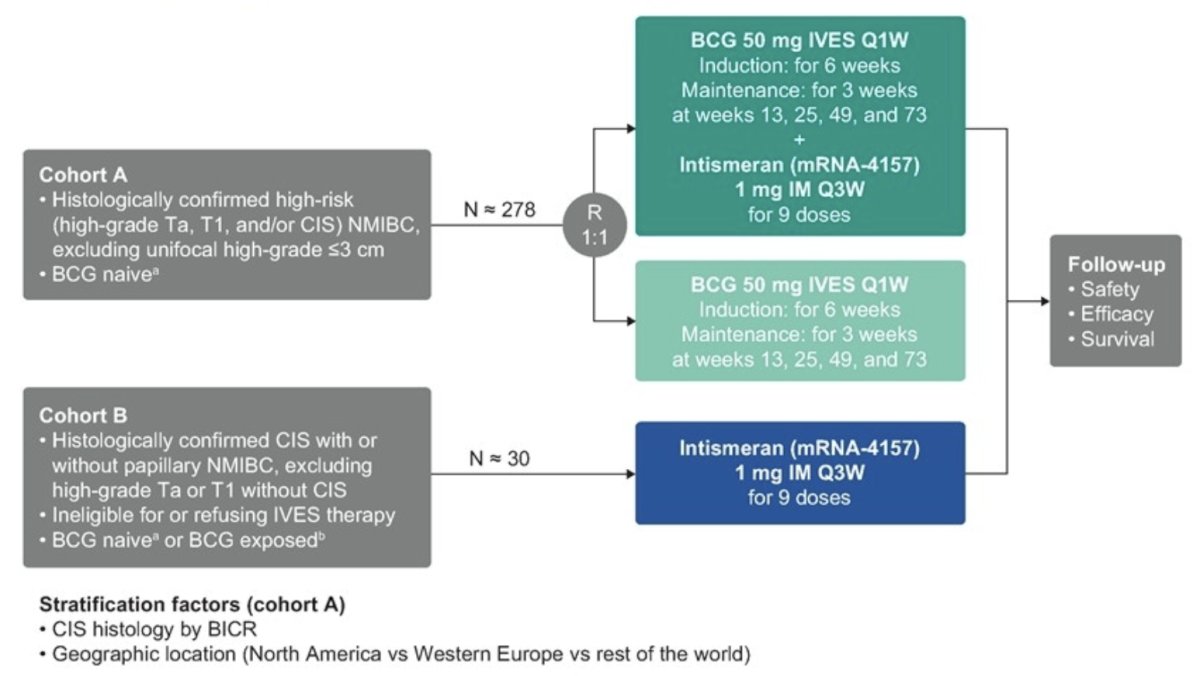
It is hypothesized that intismeran autogene will enhance the antitumor activity of BCG by boosting endogenous antitumor T-cell responses directed at the unique neoantigens of the tumor. INTerpath-011 (NCT06833073) is a randomized, multicohort, open-label, phase 2 study evaluating efficacy and safety of intismeran autogene + BCG versus BCG alone (cohort A) and intismeran autogene alone (cohort B; exploratory) in patients with high-risk non muscle invasive bladder cancer.
Eligible patients are adults with BCG-naive high-risk non muscle invasive bladder cancer (HG Ta, T1, and/or CIS; cohort A) or BCG-naive or BCG-exposed high-risk non muscle invasive bladder cancer (CIS ± papillary tumors [HG Ta or T1]) who are ineligible for or refusing intravesical therapy (cohort B). BCG naive is defined as either not receiving BCG or having received BCG >2 years before high-risk non muscle invasive bladder cancer recurrence. BCG exposed is defined as having not received adequate BCG dosing and high-risk non muscle invasive bladder cancer recurrence within 2 years of the last BCG dose. Patients must undergo TURBT ≤12 weeks before enrollment and provide tumor tissue and blood samples for NGS and intismeran autogene production and blood for ctDNA testing. In cohort A, ∼278 patients will be randomly assigned 1:1 to receive intravesical BCG (50 mg; induction: every week × 6 weeks; maintenance: every week × 3 weeks at weeks 13, 25, 49, and 73) with or without intismeran autogene 1 mg IM every 3 weeks × 9 doses. In cohort B, ∼30 patients will receive intismeran autogene 1 mg IM every 3 weeks × 9 doses:
Disease assessment (urine cytology by blinded independent central review and cystoscopy) will occur every 12 weeks (and ≥4 weeks after last BCG dose in cohort A) for the first 2 years and every 24 weeks for years 3–5. CT urogram or MR urogram will occur every 72 weeks for the first 2 years and every 104 weeks for years 3–5. The primary end points are event free survival (cohort A) and complete response rate (cohort B) by blinded independent central review. Secondary end points include recurrence free survival, disease free survival, overall survival, time to cystectomy, and safety (both cohorts). Enrollment is ongoing at the following sites:

Clinical trial identification: NCT06833073
Presented by: Petros Grivas, MD, PhD, Associate Professor, Department of Medicine, Division of Hematology Oncology, Clinical Director, Genitourinary Cancers Program, Fred Hutch Cancer Center, University of Washington Medicine, Seattle, WAWritten by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.