(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma trials in progress session and a presentation by Dr. Guillaume Grisay discussing EORTC GUCG 2418 STARBUST and strategies for treatment adaptation following re-evaluation of the bladder after using primary neoadjuvant systemic therapies. The standard treatment for patients with muscle invasive bladder cancer consists of neoadjuvant systemic therapy followed by radical cystectomy or trimodal therapy. Currently, patients are not routinely reassessed after neoadjuvant systemic therapy and proceed directly to local treatment, leading to a missed opportunity for patients with complete or near complete response to benefit from bladder sparing strategies. On the other hand, for the non-responders, it is a missed opportunity to early systemic escalation. Unfortunately, several studies have shown an insufficient concordance between the clinical and pathological staging of muscle invasive bladder cancer, unraveling the inadequacy of the current methods for clinical stating post-neoadjuvant chemotherapy.
The platform will involve multiple steps. First, STARBUST-1 is a single arm phase II trial that aims to create an effective multimodal signature that can predict effectively predictive pathological complete response to neoadjuvant systemic therapy. Second, STARBURST-2 will be developed as a risk-adapted strategies trial based on the response to neoadjuvant chemotherapy. This strategy will consist of omitting the local treatment in responders substituting it with intravesical or systemic treatment and, in non-responders, replacing it with immediate systemic escalation.
STARBUST-1 is a single arm prospective phase II trial in which patients with newly diagnosed muscle invasive bladder cancer (pT2-pT4aN0-1M0) will be included. All patients will be treated with standard of care neoadjuvant systemic therapy followed by radical cystectomy. All patients will be assessed before neoadjuvant systemic therapy with a cystoscopy, urine cytology, bladder mpMRI using the NacVi-RADS score, as well as blood and urine liquid biopsy. After completion of neoadjuvant systemic therapy, each patient will undergo a cystoscopy (± biopsy), standard of care clinical and radiological workup (CT ± FDG-PET), a mpMRI, and blood/urine collection:
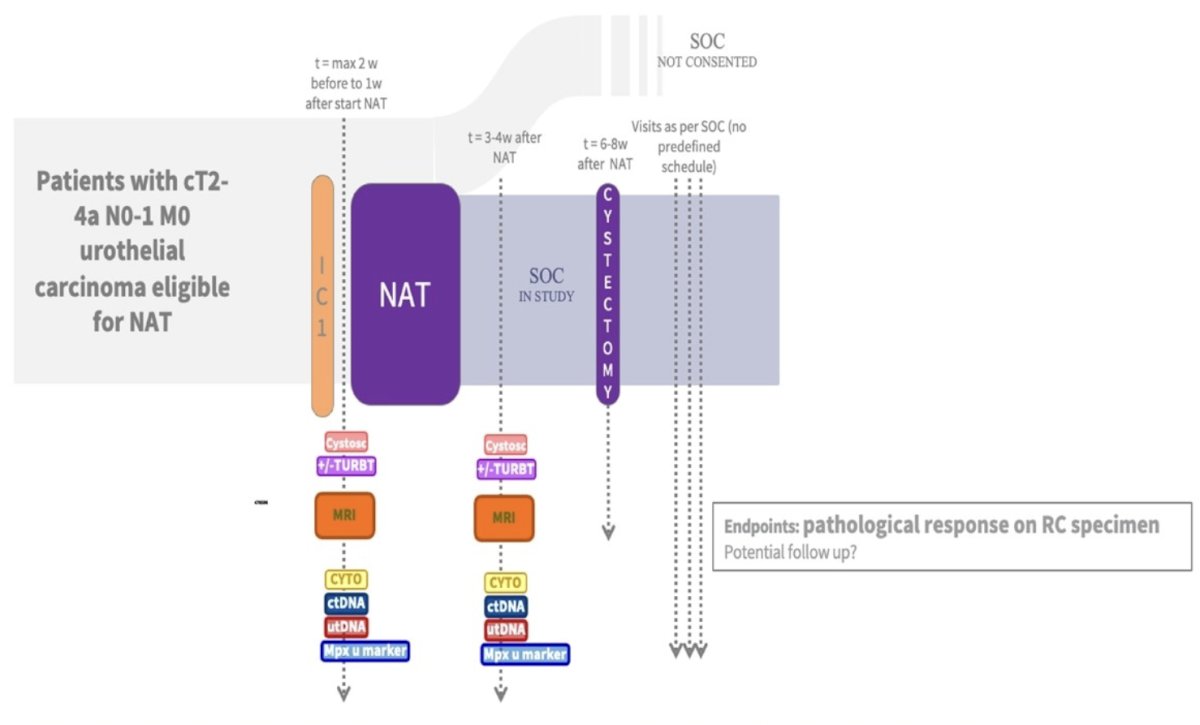
The primary endpoint is to prospectively validate (i) the accuracy of the NacVI-RADS to predict the pathological complete response defined as the absence of residual disease on the cystectomy specimen (ypT0), (ii) the accuracy of the NacVI-RADS score to predict the pathological near complete response defined as the absence of muscle invasive disease on cystectomy specimen (ypT0/Ta/T1), and (iii) to predict the absence of muscle invasive disease (ypT≥2 versus ypT0/Ta/T1) assessed by negative predictive value, positive predictive value, and receiver operating curves. Kappa score agreement between the MRI staging and radical cystectomy pathological staging will also be addressed.
Secondary endpoints include the assessment of new biomarkers including blood circulating tumor DNA and urine tumor DNA, urines multiplex biomarkers, pathomics, radiomics and molecular alterations that could predict the pathological response. The investigators will also assess the added discriminative ability of a multimodal clinic-radiological-genetic score that include cystoscopy, MRI and liquid biopsies over standard of care clinic-radiological evaluation.
Clinical trial identification: NCT02834884
Presented by: Guillaume Grisay, MD, PhD, Centres Hospitaliers Universitaires, Woluwe-Saint-Lambert, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025