(UroToday.com) The 2025 ESMO annual meeting featured a Presidential Symposium session and a discussant presentation by Dr. Alexander W. Wyatt discussing “IMvigor011: A Phase 3 trial of ctDNA-guided adjuvant atezolizumab versus placebo in muscle invasive bladder cancer” presented by Dr. Thomas Powles. ctDNA is comprised of apoptosing cells that shed DNA fragments into the blood (ie. cell-free DNA (cfDNA)). Normal cfDNA is from the blood lineage, with an average of ~1,000 diploid genomes per 1 mL of blood plasma. ctDNA originates from cancer cells, and mutations in ctDNA are representative of matched tumor tissue. In 2008, the discovery was made that serial ctDNA can monitor tumor dynamics.1
Furthermore, cf/ctDNA ‘shedding’ is linked with proliferative, active populations, such has high placental cfDNA in maternal plasma during pregnancy. The key point from Dr. Wyatt is that detection of ctDNA molecules indicates the presence of live cancer cells.
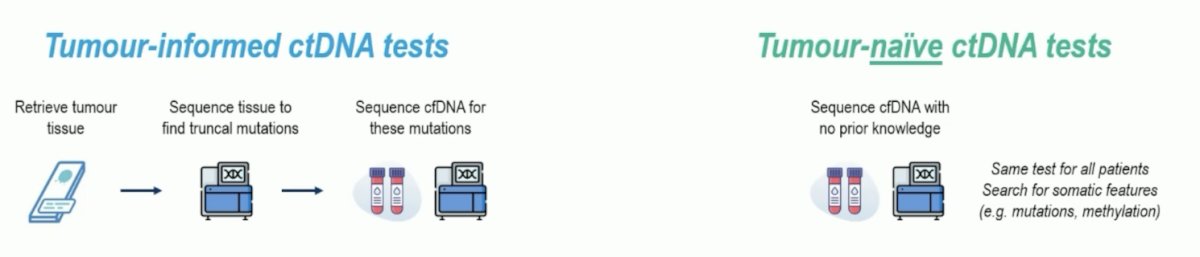
With regards to the technology of ctDNA detection, ctDNA is distinguished from normal cfDNA by cancer features (ie. mutations), and there are two broad classes of ctDNA detection tests: informed versus naïve:
- Tumor-informed ctDNA tests: the pros are that it is specific and already established, and the cons are that it takes time, is costly, and there are tissue failures
- Tumor-naïve ctDNA tests: the pros are that it is quick, easy for screening, with no tissue needed, and the cons are that has lower specificity
IMvigor011 used the Signatera tumor-informed ctDNA test in the trial: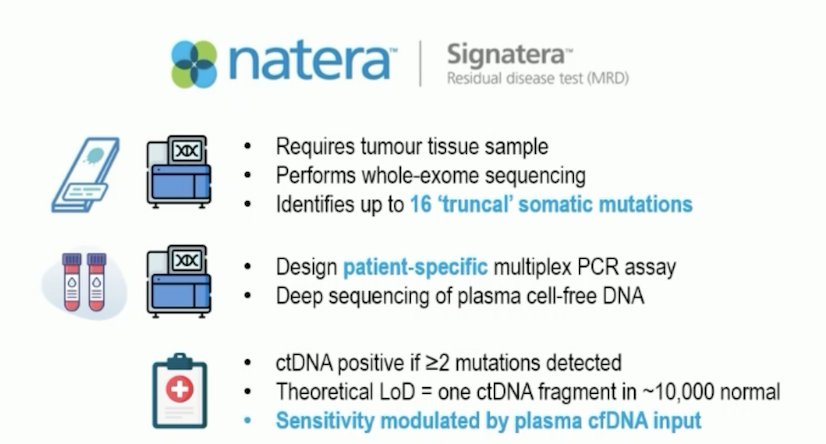
Dr. Wyatt noted that ctDNA detected in muscle invasive bladder cancer is associated with disease relapse. The negative IMvigor010 trial2 tested adjuvant atezolizumab in muscle invasive bladder cancer, but a prespecified ctDNA analysis suggested an overall survival benefit in ctDNA positive patients:3

The headline from today’s presentation is: IMvigor011 provides level 1 evidence for intervening on the basis of a positive plasma ctDNA test. This is the first completed randomized phase III trial to test treating because of a ctDNA+ result in muscle invasive bladder cancer, with dual wins in disease free survival and overall survival. Additionally, it sets serial plasma ctDNA assessment apart from conventional clinicopathologic risk tools used in other designs, such as the CheckMate-2744 and AMBASSADOR5 trials. IMvigor011 also advances the concept of adjuvant therapy in muscle invasive bladder cancer from “treat most” to “treat those with molecular evidence of disease.”
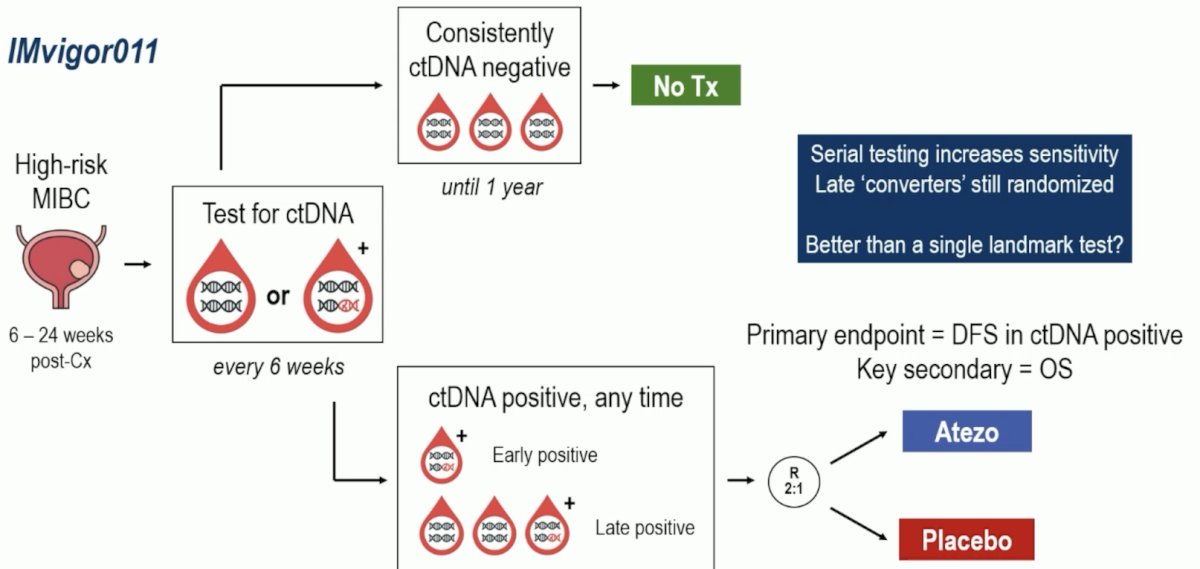
Dr. Wyatt emphasized that one of the strengths of IMvigor011 is the serial blood testing to clarify ctDNA status. Serial testing increased the sensitivity of late ctDNA+ converters and allowed these patients to still be randomized:
In 357 patients who persistently tested ctDNA−, the disease free survival rate was 95.4% at the end of the 1-year monitoring period and 88.4% at 2 years. Similarly, those patients who were persistently ctDNA- had a 1 year overall survival rate of 100% and 2 year rate of 97.1%:
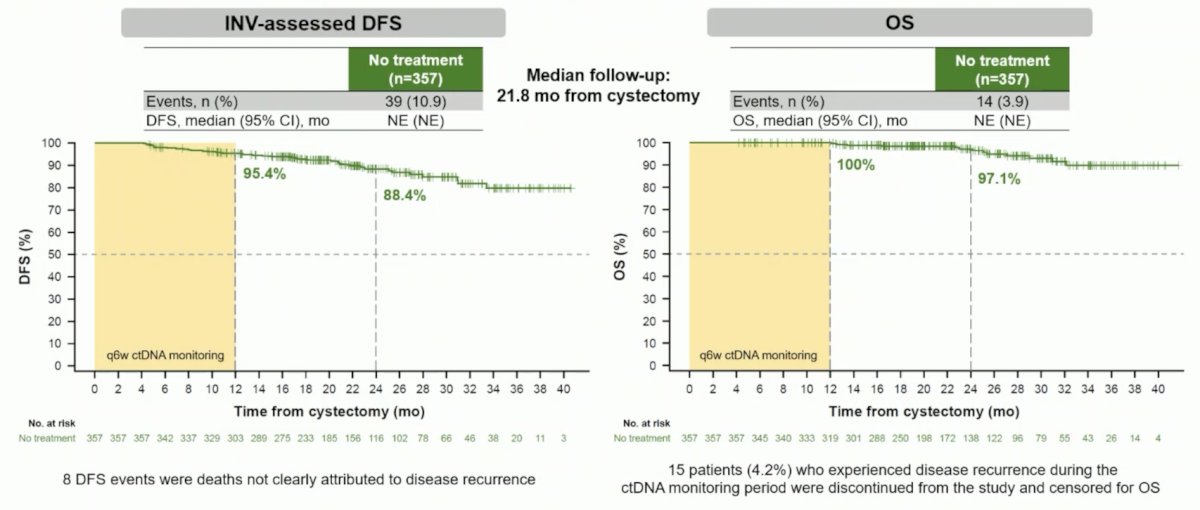
Dr. Wyatt notes that this shows there are excellent outcomes with surveillance alone, avoiding treatment toxicity and cost, but there is still a “non-zero” risk of recurrence or death for these patients.
Do we need to boost the ctDNA test detection sensitivity? A higher theoretical sensitivity is possible with new technology (and more blood), and tissue genome-informed testing is promising. However, it is unclear if tumor naïve tests will have equivalent or higher sensitivity:

What remains unknown is what an acceptable false-negative rate is and how often we should retest. There may be diminishing returns with increasing test sensitivity, as some disease is inherently low ctDNA shedding, albeit with the best prognosis, but unknown disease biology.
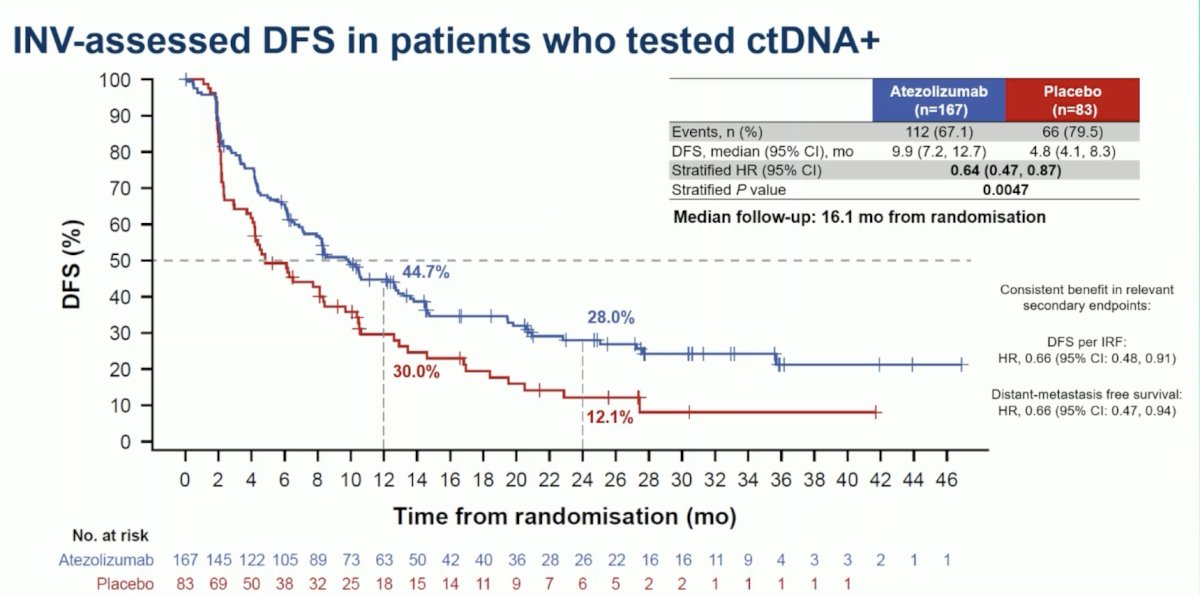
In IMvigor011, at a median follow-up of 16.1 months, patients in the atezolizumab arm had statistically significant improvements in disease free survival (HR 0.64, 95% CI 0.47, 0.87; p = 0.0047) versus the placebo arm:
Additionally, patients in the atezolizumab arm had statistically significant improvements in overall survival (HR 0.59, 95% CI 0.39, 0.90; p = 0.0131) versus the placebo arm:

Dr. Wyatt notes that the subgroups are largely consistent with the intention to treat results, but PD-L1 status and ctDNA+ early versus late are relevant. For example, ~30% of patients took >20 weeks post-radical cystectomy to become ctDNA positive, which may lead to less disease free survival benefit:

Is late positivity associated with lower ctDNA level and more ‘indolent disease’? Dr. Wyatt emphasized that in the future we should abandon a binary ctDNA status and rather move to a continuous variable, as low ctDNA can hover around the detection limit. Where the IMvigor011 results fit into the perioperative muscle invasive disease landscape will be up for debate, given the now plethora of data in this disease space: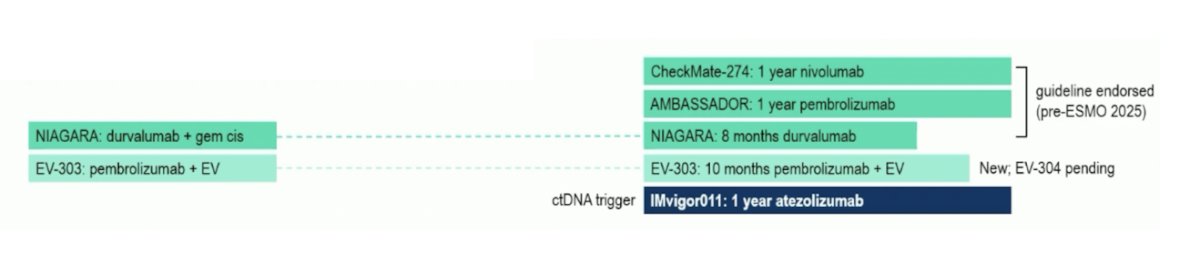
But, what Dr. Wyatt sees is an opportunity for ctDNA to influence immunotherapy decisions across several time points in the disease space:

Dr. Wyatt emphasized that there are several bumps on the road to adoption of ctDNA testing, including (i) limited access to ctDNA tests outside the United States, (ii) we do not know what the cost-effectiveness of ctDNA-guided treatment versus a treat-all strategy is, and (iii) the optimal ctDNA test strategy across the perioperative setting unknown. This could be tumor-informed (ie. Signatera), but this is not equivalent to tumor-naïve assays. Moreover, analytic and clinical validity of hospital laboratory-developed tests must be established, and there is a need to optimize logistics of tissue selection (pre- versus post-neoadjuvant chemotherapy, upper tract urothelial carcinoma, etc) and retrieval. Can hospital molecular pathology labs implement ctDNA detection tests? Yes, but it is more difficult than conventional ‘genomic testing’ and may require commercial out-of-box solutions. Additionally, there needs to be a sufficient case volume to make this viable, which may be leveraged with pan-cancer applicability. This will also require oncology collaboration to establish analytical and clinical validity of any new test.
Dr. Wyatt concluded his discussant presentation of IMvigor011 with several conclusions and open questions:
- Conclusions:
- This is the strongest evidence to date for intervening with adjuvant systemic therapy on the basis of detecting plasma ctDNA
- This data represents excellent outcomes in serial ctDNA-negative muscle invasive bladder cancer (consistent with colorectal cancer)
- Open questions:
- Is this effect therapy-agnostic?
- What is the optimal ctDNA test characteristics for muscle invasive bladder cancer?
- When should we test, how often should we test, and how sensitive is a test?
- What is the biology and therapy vulnerability of ctDNA low shedding disease?
Presented by: Alexander W. Wyatt, PhD, D.Phil, Assistant Professor, Department of Urologic Sciences, University of British Columbia, Senior Research Scientist, Vancouver Prostate Centre, Vancouver, BC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
References:
- Diehl F, Schmidt K, Choti MA, et al. Circulating mutant DNA to assess tumor dynamics. Nat Med. 2008 Sep;14(9):985-990.
- Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): A multicentre, open-label, randomized, phase 3 trial. Lancet Oncol. 2021 Apr;22(4):525-537.
- Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021 Jl;595(7867):432-437.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021 Jun 3;384(22):2102-2114.
- Apolo AB, Ballman KV, Sonpavde G, et al. Adjuvant pembrolizumab versus observation in muscle-invasive urothelial carcinoma. N Engl J Med. 2025 Jan 2;392(1):45-55.