(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st, 2025 was host to a presidential symposium. Dr. Andrea Necchi discussed the RC48-C016 trial of disitamab vedotin + toripalimab (DV+T) versus chemotherapy as 1st line therapy in patients with locally advanced or metastatic urothelial carcinoma (la/mUC) with HER-2 expression, previously presented by Dr. Jun Guo.
Dr. Necchi began by noting that only 5-10% of patients are diagnosed with de novo metastatic urothelial carcinoma, with 50% of patients with la/mUC progressing from earlier stages. To date, based on evidence from clinical trials, the longest median overall survival is observed with enfortumab vedotin + pembrolizumab (EV+P) at 31.5 months.1 In contrast to other trials in this space evaluating other systemic therapy regimens that included ‘all comers’ (e.g., gemcitabine + cisplatin +/- nivolumab, maintenance avelumab, M-VAC, gemcitabine + carboplatin),2,3 pre-screening for HER2 IHC expression was required for enrollment in to the RC48-C016 trial.
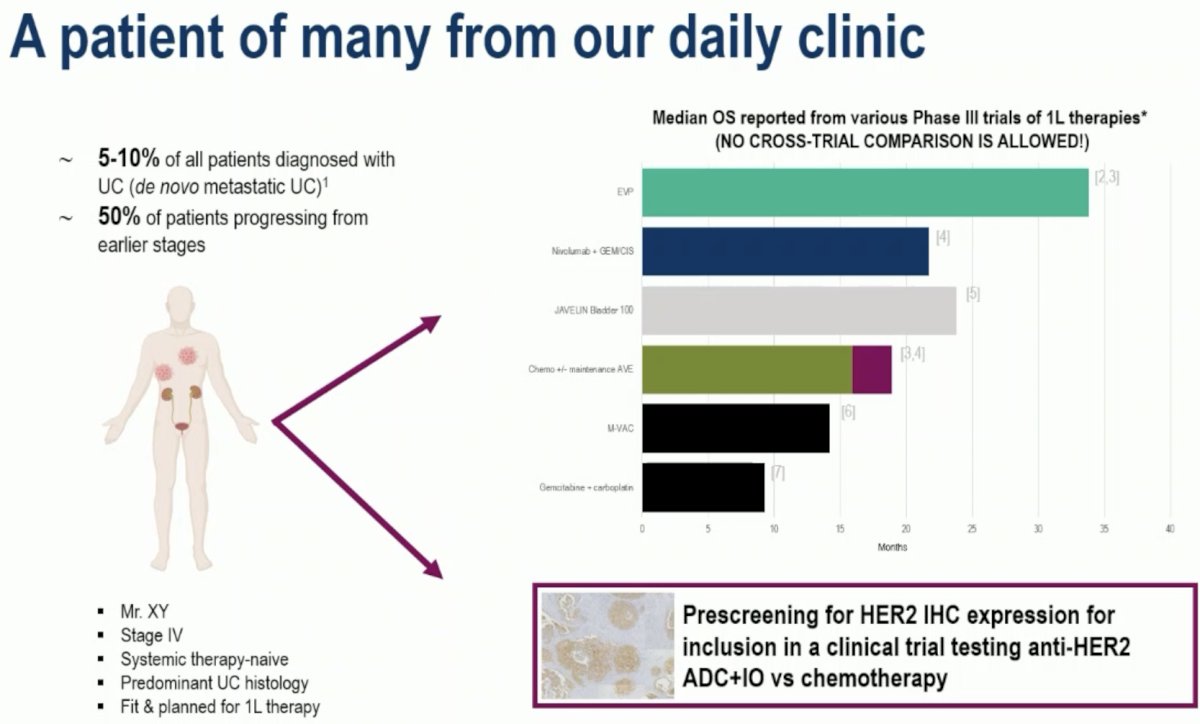
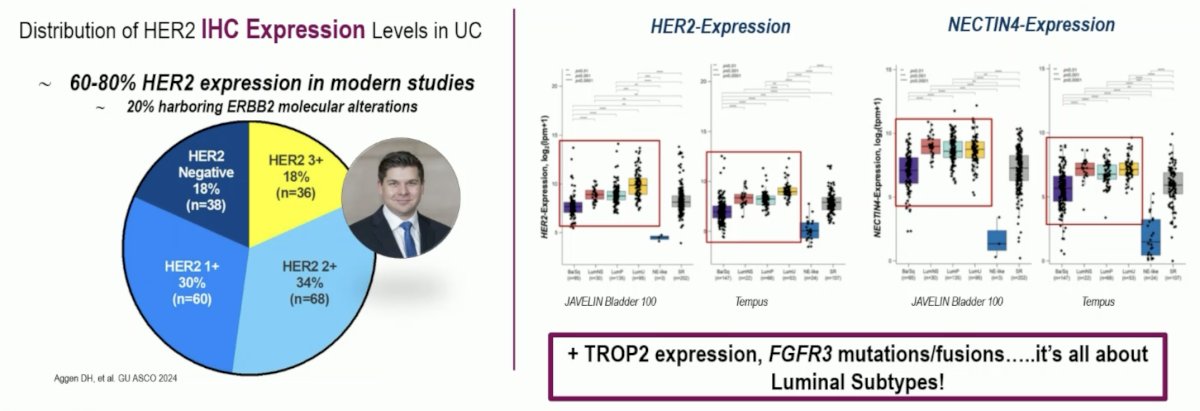
Dr. Necchi remarked that, in his opinion, HER2 is a suitable target for antibody-drug conjugates (ADCs) in urothelial cancers. 60-80% of tumors express HER2 in modern studies, and ~20% harbor ERBB2 molecular alterations. Additionally, these tumors tend to be positive for TROP2 expression and FGFR3 mutations/fusions, which reflect a predominant luminal subtype.
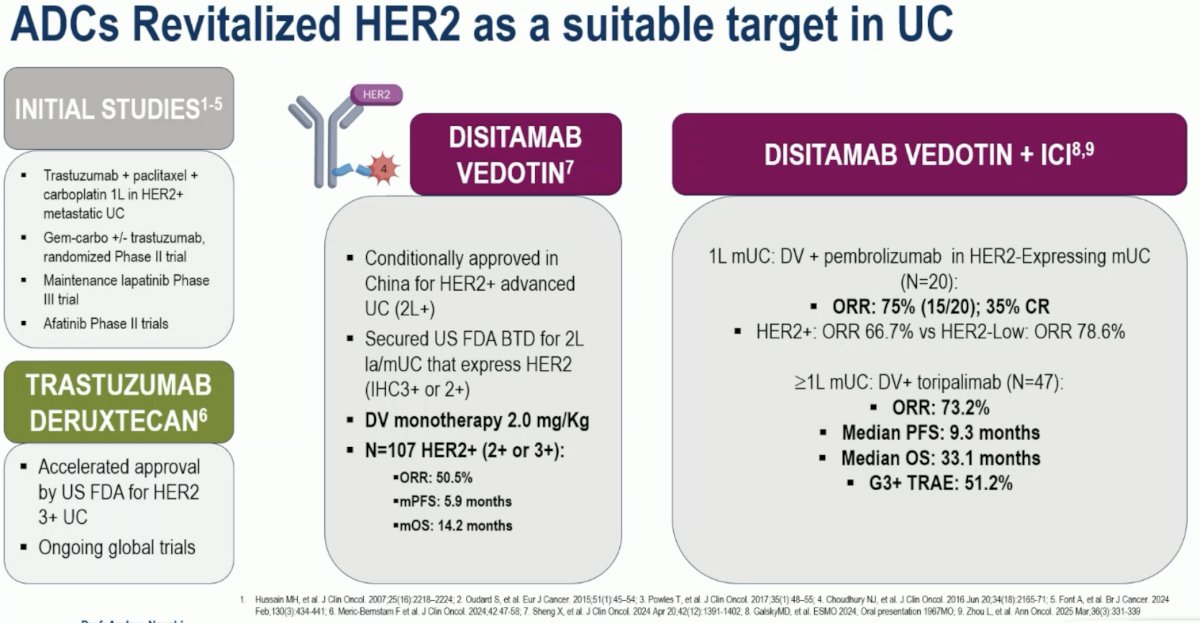
Numerous studies have evaluated HER2-targeted antibody-drug conjugates (ADCs) in urothelial cancer. The initial studies evaluated trastuzumab + paclitaxel + carboplatin as 1st line therapy for patients with HER2+ metastatic urothelial carcinoma.4 Trastuzumab deruxtecan was granted accelerated approval by the US FDA for HER2 3+ urothelial carcinoma and is being evaluated in ongoing global trials.5 Disitamab vedotin was initially conditionally approved in China for HER2+ advanced urothelial carcinoma in the ≥2nd line setting. It has secured US FDA breakthrough designation for the treatment of 2nd line la/mUC that express HER2. DV monotherapy has demonstrated an objective response rate (ORR) of 51% in 107 patients with HER2+ la/mUC, with median progression-free (PFS) and overall survivals (OS) of 5.9 and 14.2 months, respectively.6
The combination of DV+T has been evaluated in a small trial of 20 patients with HER-2 expressing mUC treated in the 1st line setting. The ORR was 75%, with a 35% complete response (CR) rate.7 In another trial evaluating DV+T in the ≥1st line mUC setting, this combination was associated with an ORR of 73%, with a median PFS and OS of 9.3 and 33.1 months, respectively.8
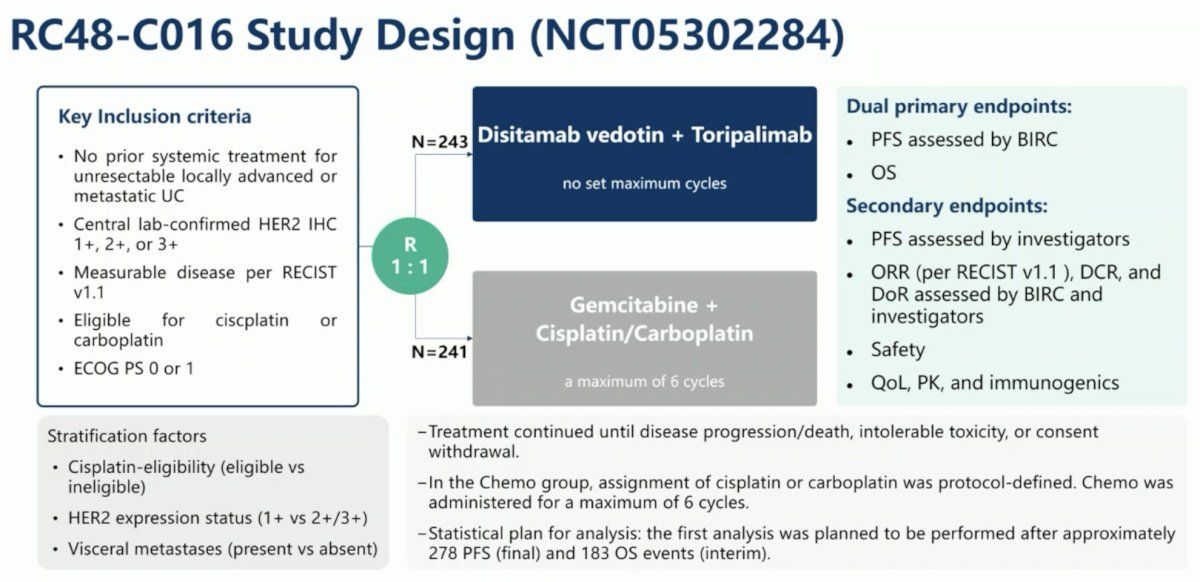
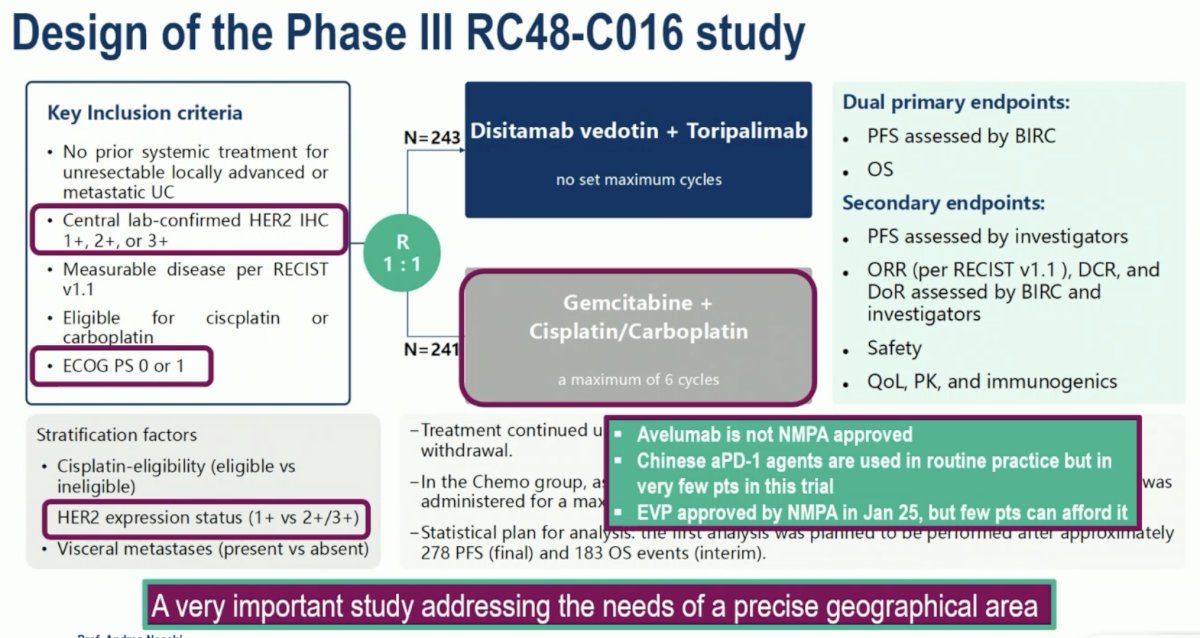
The study design of RC48-C016 is illustrated below. The key inclusion criteria were as follows:
- Treatment-naïve patients with unresectable la/mUC
- IHC 1+, 2+, or 3+
- Eligible for platinum-based chemotherapy
- Excellent performance status
Eligible patients underwent 1:1 randomization to:
- Disitamab vedotin + toripalimab (no set maximum cycles)
- Gemcitabine + cisplatin/carboplatin (maximum: 6 cycles)
The dual primary endpoints were:
- PFS, by blinded independent central review (BICR)
- OS
Dr. Necchi made several key comments regarding the study design of this trial:
- Patients were required to have central lab-confirmed HER2 IHC expression (1+/2+/3+)
- All patients were required to have an excellent performance status (ECOG 0-1)
- Avelumab is not approved in China as maintenance therapy following platinum-based chemotherapy
- EV+P is approved by the National Medial Products Administration (NMPA) in China, but only a few patients can afford this regimen
He remarked that this is ‘a very important study addressing the needs of a precise geographical area’.
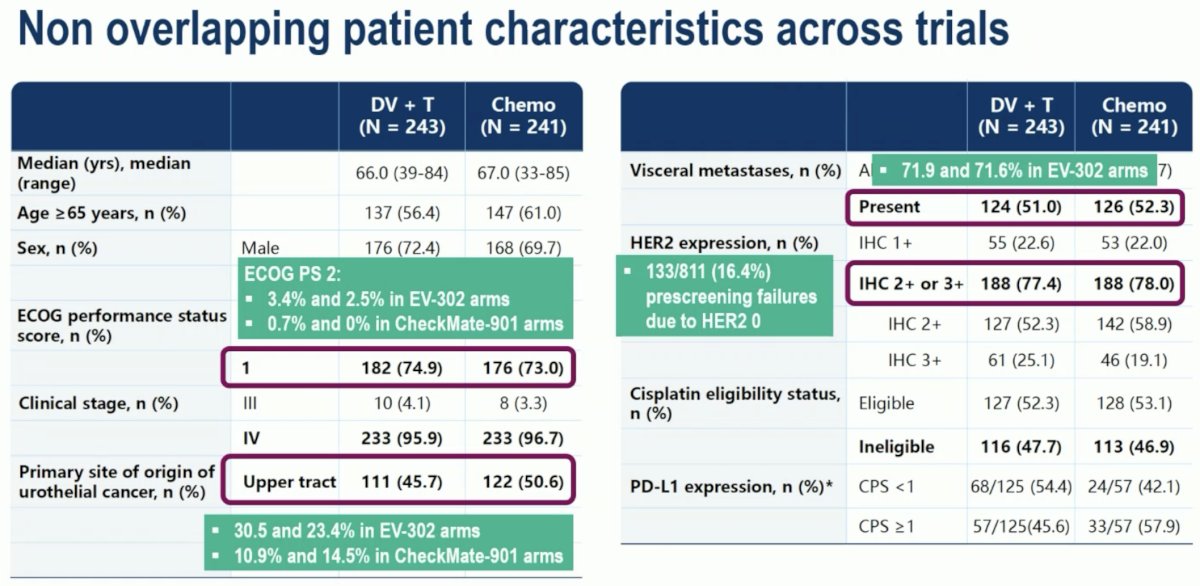
There were several key study population characteristics that were unique to this trial:
- None of the patients had ECOG performance status 0-2
- EV-302: 2.5–3.4% of patients
- CheckMate-901: 0–0.7%
- Nearly 50% of patients in RC48-C016 had upper tract disease
- EV-302: 23.4–30.5%
- CheckMate-901: 10.9–14.5%
- Only 51-52% of patients had visceral metastases
- EV-302: 71.6-–71.9%
- 16.4% of la/mUC patients were pre-screening failures due to HER2 non-expression
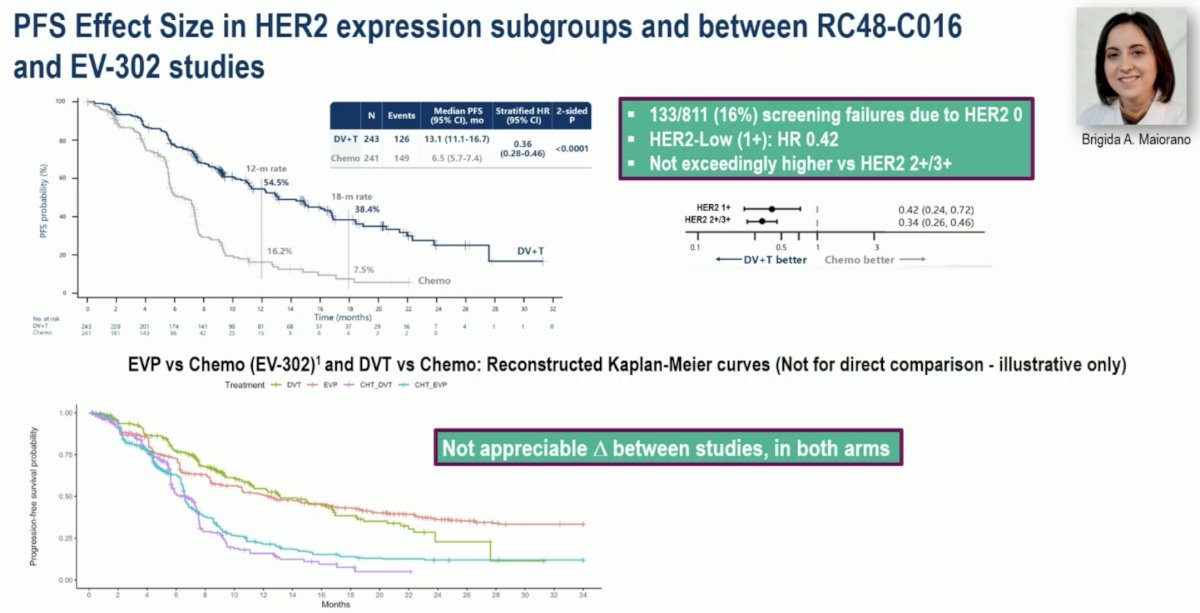
Dr. Necchi noted that the magnitudes of effect (i.e., HRs) for PFS were similar for HER-2 high-expressing (2+/3+) and low-expressing (1+) tumors (HRs: 0.34 and 0.42, respectively). Additionally, there were no appreciable differences in the magnitude of benefit for EV+P versus chemotherapy and DV+T versus chemotherapy, questioning the value of opting for biomarker-selected (i.e., HER2+) regimens, such as DV+T, particularly when 16% of patients will be ineligible for this treatment and EV+P is widely available with a similar relative benefit.
A similar pattern was observed for OS:
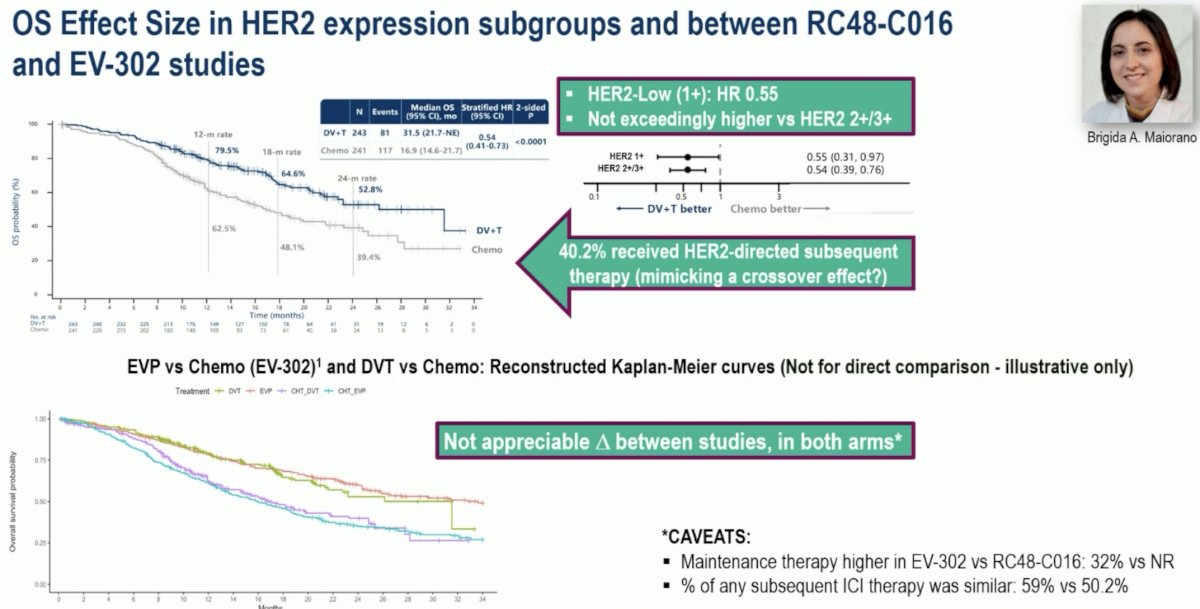
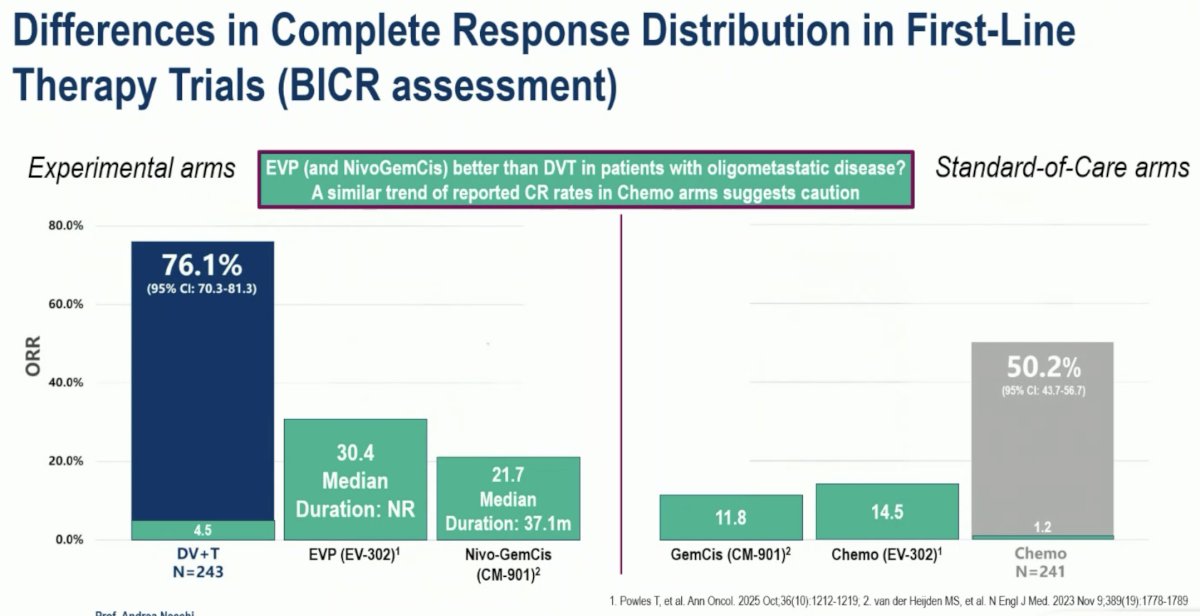
Notably, only 4.5% of patients achieved a CR with DV+T, which pales in comparison to EV+P (30.4%) and nivolumab + gemcitabine + cisplatin (21.7%).
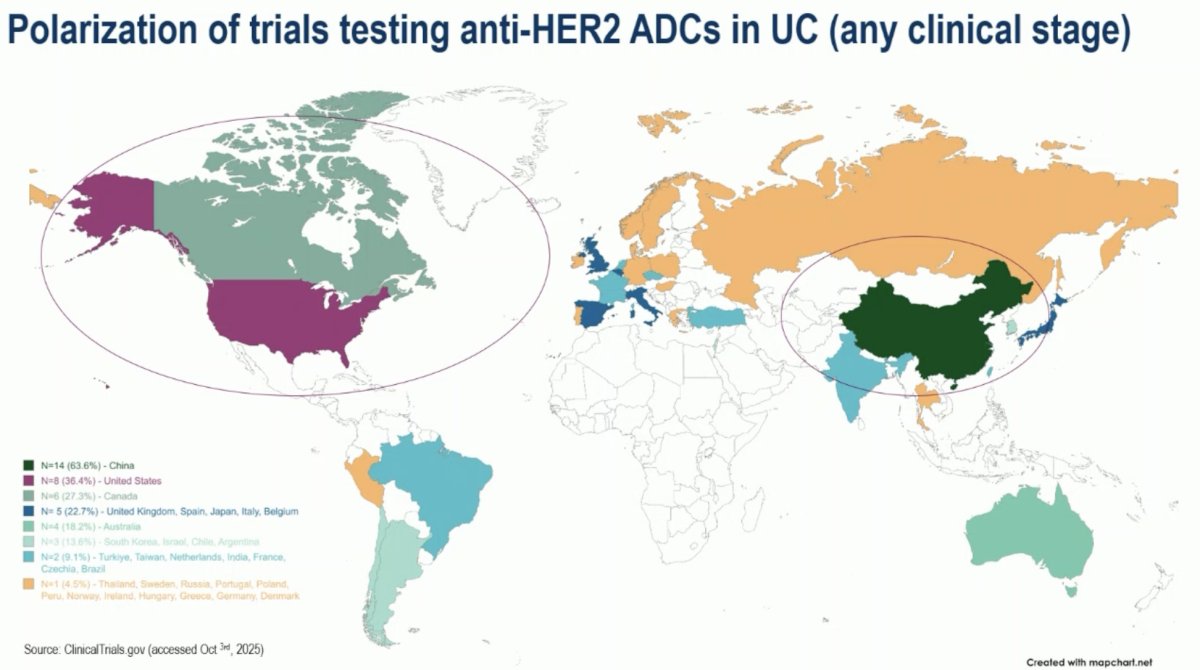
From a global perspective, there is a clear geographic polarization of trials testing anti-HER2 ADCs in urothelial carcinoma – particularly in North America and China.
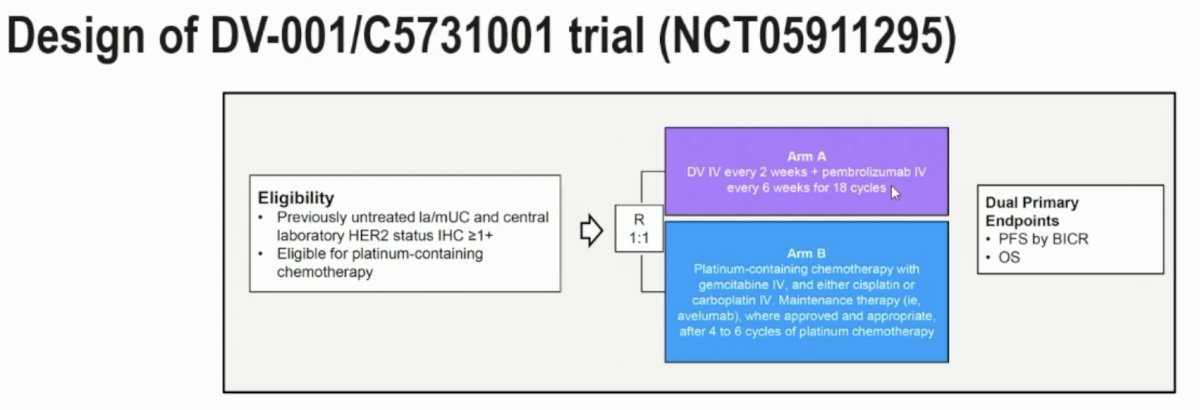
The ongoing DV-001/C5731001 trial (NCT05911295) is evaluating DV + pembrolizumab versus platinum chemotherapy followed by maintenance avelumab in patients with HER2-expressing la/mUC. Do we need to await the results of this trial prior to accepting front line DV + IO therapy on a global stage? Will pembrolizumab be as effective as toripalimab?
Dr. Necchi concluded his discussion of the RC48-C016 trial of disitamab vedotin + toripalimab in HER2-expressing locally advanced/metastatic urothelial carcinoma as follows:
- Treatment Efficacy:
- The combination of disitamab vedotin and toripalimab resulted in a statistically significant and clinically meaningful improvement in PFS and OS, versus chemotherapy, in patients with HER2+ locally advanced/metastatic urothelial carcinoma
- Disitamab vedotin + toripalimab is an additional therapeutic option for such patients
- Healthcare Resource Allocation and Patient Selection Strategies:
- There were more similarities than differences among the RC48-C016 and EV-302 trials
- Provided that enfortumab vedotin + pembrolizumab is available and reimbursable in a certain region, is it worth screening for HER2 expression?
- When? For whom? Is there any appreciable benefit for HER2 3+ vs HER2 low-expressing patients?
- More pronounced differences in therapeutic pathways are eagerly awaited using biomarker-based strategies
- The treatment landscape is rapidly evolving, and therapeutic attrition will impact access to novel therapies
- Geographical disparities in trials and drug approval allocation have become noteworthy in this disease space, representing an urgent call for more inclusive trials a=nd equitable access to novel therapies reflecting the standard-of-care.
Presented by: Andrea Necchi, MD, Chief of Genitourinary Medical Oncology, IRCCS San Raffaele Hospital and Scientific Institute, Professor of Oncology, Vita-Salute San Raffaele University, Milan, Italy
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. N Engl J Med. 2024;390(10):875-888.
- Powles T, Park SH, Voog E, et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N Engl J Med 2020; 383(13):1218-1230.
- van der Heijden MS, Sonpavde G, Powles T, et al. Nivolumab plus gemcitabine–cisplatin in advanced urothelial carcinoma. N Engl J Med. 2023;389(19):1778-1789.
- Hussain MH, MacVicar GR, Petrylak DP, et al. Trastuzumab, paclitaxel, carboplatin, and gemcitabine in advanced HER2/neu-positive urothelial carcinoma: results of a multicenter phase II National Cancer Institute trial. J Clin Oncol. 2007;25(16):2218-2224.
- Meric-Berstam F, Makker V, Oaknin A, et al. Efficacy and safety of trastuzumab deruxtecan in patients with HER2-expressing solid tumours: primary results from the DESTINY-PanTumor02 phase II trial. J Clin Oncol. 2024;42(1):47-58.
- Sheng X, Wang L, He W, et al. Efficacy and Safety of Disitamab Vedotin in Patients With Human Epidermal Growth Factor Receptor 2–Positive Locally Advanced or Metastatic Urothelial Carcinoma: A Combined Analysis of Two Phase II Clinical Trials. J Clin Oncol. 2024;42(12):1391-1402.
- Galsky MD, et al. Preliminary efficacy and safety of disitamab vedotin with pembrolizumab in treatment-naïve HER2-expressing locally advanced or metastatic urothelial carcinoma: RC48G001 Cohort C. ESMO 2024;13–17 Sept, Barcelona. Oral presentation #1967MO.
- Zhou L, Yang KW, Zhang S, et al. Disitamab vedotin plus toripalimab in patients with locally advanced or metastatic urothelial carcinoma (RC48-C014): a phase Ib/II dose-escalation and dose-expansion study. Ann Oncol. 2025;36(3):331-339.