(UroToday.com) The 2025 ESMO annual meeting featured a Presidential Symposium session and a presentation by Dr. Thomas B. Powles discussing results from IMvigor011, a phase 3 trial of ctDNA-guided adjuvant atezolizumab versus placebo in muscle invasive bladder cancer. Although radical cystectomy with or without neoadjuvant therapy is curative for many patients with muscle invasive bladder cancer, ~50% will develop disease recurrence, which is associated with poor prognosis. Adjuvant immunotherapy is recommended but has yet to achieve a significant survival advantage. Thus, due to variable outcomes after cystectomy, there is a need to differentiate patients who are destined to relapse from those who are not.
Growing evidence suggests that ctDNA-based detection of molecular residual disease is strongly prognostic after cystectomy. Focusing treatment on patients who test ctDNA+ potentially enriches for immunotherapy benefit while sparing patients who test ctDNA– from unnecessary treatment and toxicities. Previously, adjuvant atezolizumab did not provide significant disease free survival or overall survival benefit to unselected patients with muscle invasive bladder cancer in the phase 3 IMvigor010 study.1,2 However, exploratory analyses demonstrated that patients who tested ctDNA+ after cystectomy benefited from adjuvant atezolizumab (overall survival HR 0.59), while patients who tested ctDNA– did not (overall survival HR 1.38).3 At ESMO 2025, Dr. Powles and colleauges reported the primary analysis of the global, randomized, double-blind, phase 3 IMvigor011 trial studying ctDNA-guided atezolizumab versus placebo in this setting.
Patients with muscle invasive bladder cancer and no radiographic evidence of disease enrolled in surveillance within 6–24 weeks of cystectomy and underwent serial ctDNA monitoring for up to one year after surgery. Eligible patients who tested ctDNA+ were randomized 2:1 to atezolizumab 1,680 mg or placebo every 4 weeks for 12 cycles or up to 1 year:
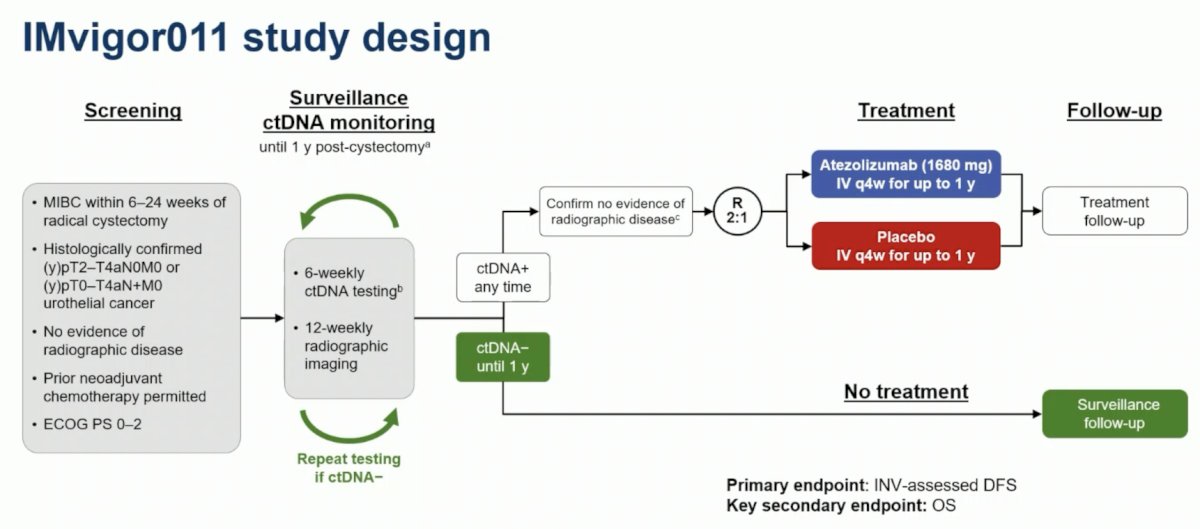
The primary endpoint was investigator-assessed disease free survival. Overall survival was a secondary endpoint with alpha control. Patients who persistently tested ctDNA− received no treatment. The statistical analysis plan included an overall Type I error (alpha) of 0.05 (2-sided), with the surveillance population planned to enroll up to 800 patients to randomize ~240 patients who tested ctDNA+. IMvigor011 had 80% power to detect a hazard ratio for disease free survival of 0.64 with 178 disease free survival events, and 60% power to detect a hazard ratio for overall survival of 0.66 with 130 overall survival events. An interim analysis of overall survival was performed at the time of the disease free survival primary analysis with the use of a hierarchical procedure. The boundary for overall survival statistical significance was determined based on the Lan-DeMets implementation of the O'Brien-Fleming use function. The CONSORT diagram highlighting patient disposition is noted in the following figure:

Overall, 761 patients were enrolled in surveillance, and the remaining 250 eligible patients who tested ctDNA+ were randomized (atezolizumab, n = 167; placebo, n = 83). The baseline demographics and characteristics for the randomized ctDNA+ patients and the persistently ctDNA- patients is as follows:

At a median follow-up of 16.1 months, patients in the atezolizumab arm had statistically significant improvements in disease free survival (HR 0.64, 95% CI 0.47, 0.87; p = 0.0047) versus the placebo arm:

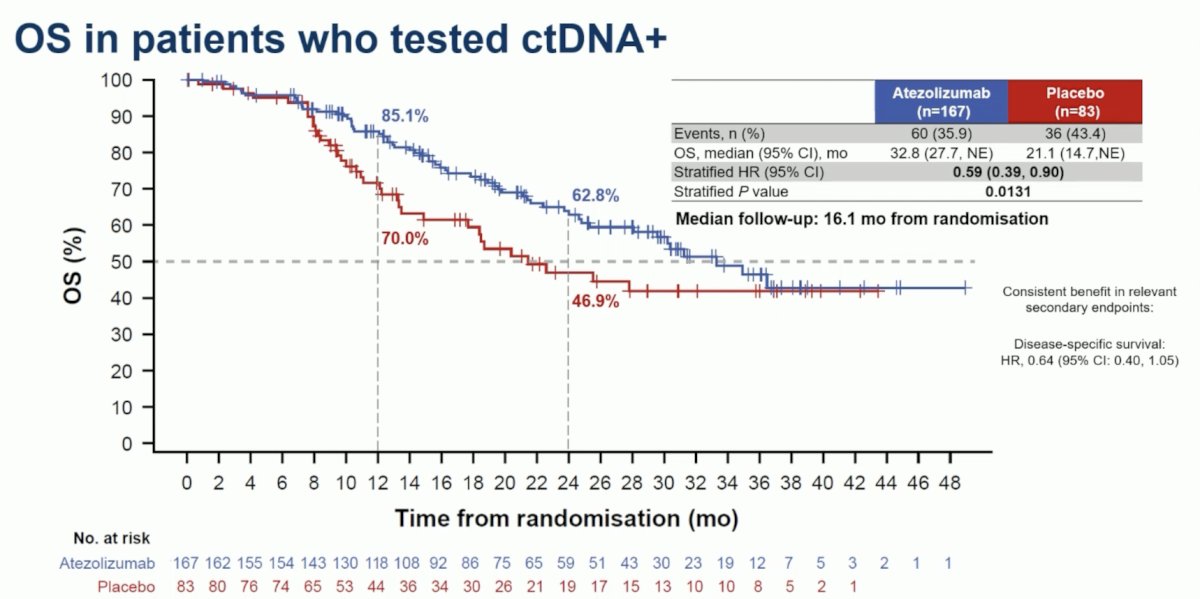
Additionally, patients in the atezolizumab arm had statistically significant improvements in overall survival (HR 0.59, 95% CI 0.39, 0.90; p = 0.0131) versus the placebo arm:
Across patient subgroups, adjuvant atezolizumab was generally associated with improved disease free and overall survival:

Disease free and overall survival in subgroups based on timing of ctDNA+ testing also favored adjuvant atezolizumab, however with several of the confidence intervals not statistically significant:

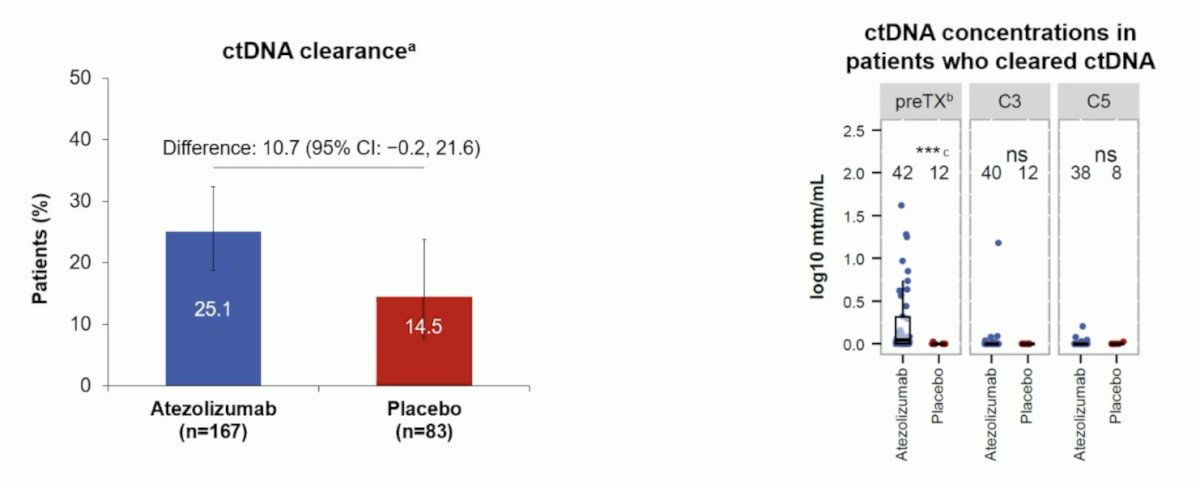
The results for ctDNA clearance and concentrations at cycle 3 and cycle 5 are highlighted in the following figure:
In 357 patients who persistently tested ctDNA−, the disease free survival rate was 95.4% at the end of the 1-year monitoring period and 88.4% at 2 years. Similarly, those patients who were persistently ctDNA- had a 1 year overall survival rate of 100% and 2 year rate of 97.1%:

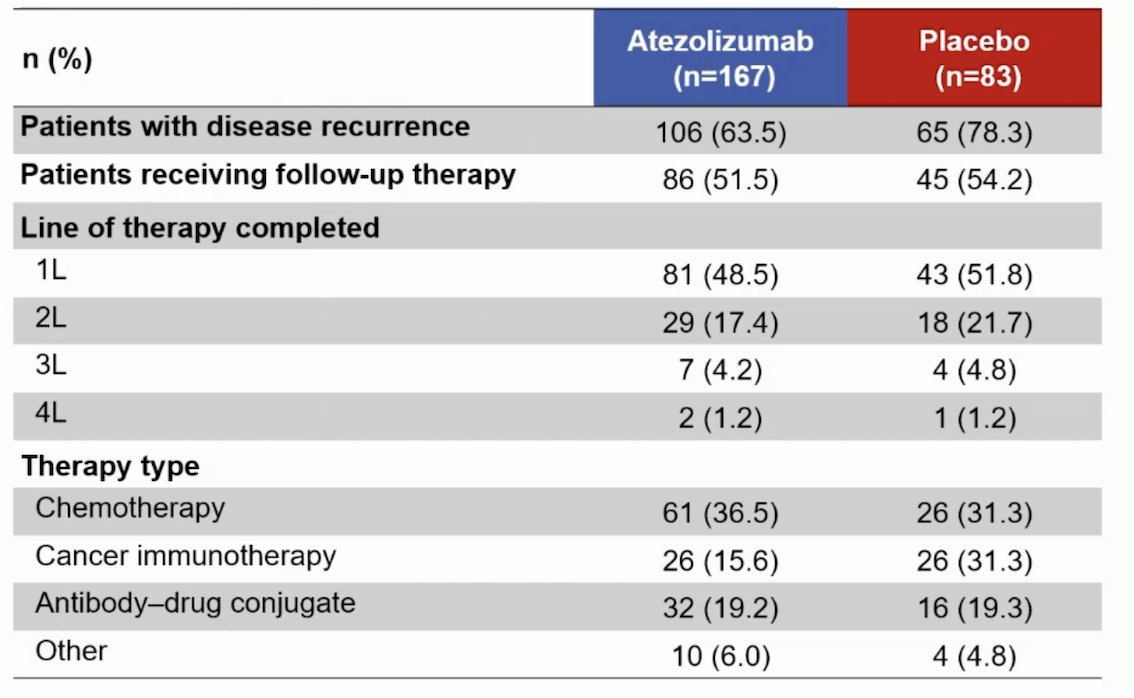
In the adjuvant atezolizumab arm, 63.5% of patients had disease recurrence compared to 78.3% in the placebo arm, with >50% of patients receiving follow-up therapy. This was most commonly chemotherapy in the atezolizumab arm (36.5%) and chemotherapy (31.3%) or immunotherapy (31.3%) in the placebo arm:
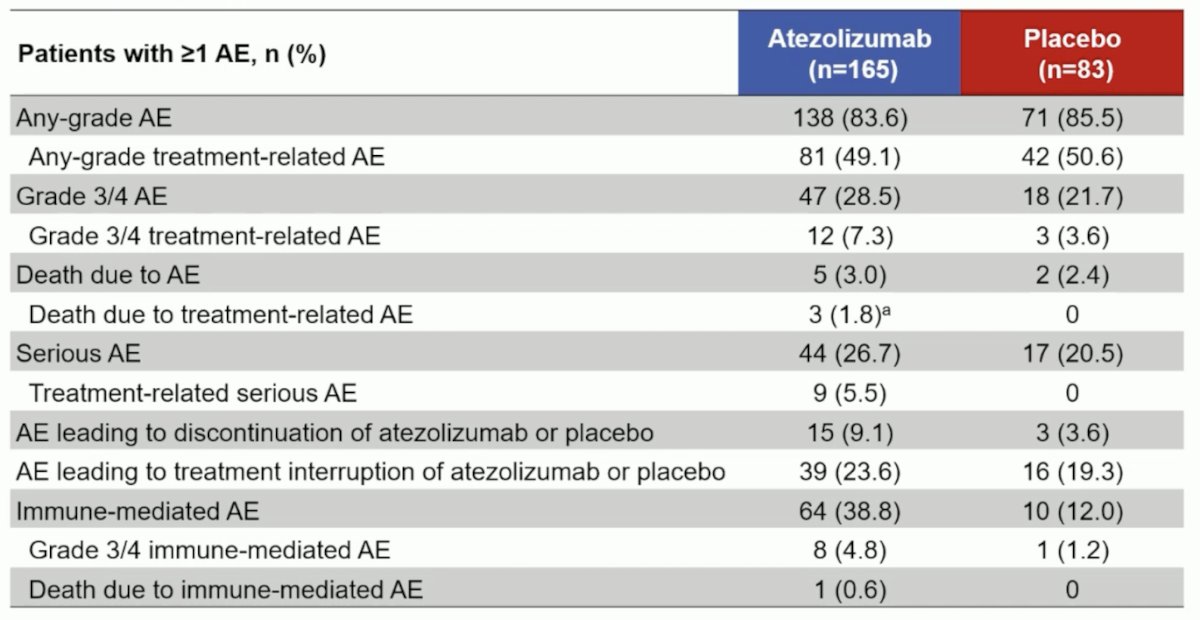
There were 28.5% of patients who received atezolizumab (n = 165) versus 21.7% who received placebo (n=83) that had Grade 3/4 adverse events (treatment-related, 7.3% versus 3.6%). Moreover, there were 3.0% of atezolizumab patients versus 2.4% of placebo patients that had fatal adverse events (treatment-related, 1.8% versus 0%):
Dr. Powles concluded his presentation discussing IMvigor011 with the following take home points:
- Adjuvant atezolizumab demonstrated statistically significant disease free survival and overall survival improvements versus placebo in patients with muscle invasive bladder cancer identified as ctDNA+ through serial molecular residual disease testing
- The clinical benefit with atezolizumab was generally consistent across key subgroups, including patients excluded from prior adjuvant trials (e.g. those with pT2N0 disease), which suggests that ctDNA status enhances risk determination beyond classical surgical pathological staging
- Similar efficacy was observed in patients with ctDNA+ status at baseline and those who converted to ctDNA+ status with repeated testing
- Patients who persistently tested ctDNA– had low risk of recurrence and death
- The atezolizumab safety profile was tolerable, with no new findings
- These findings indicate that serial ctDNA monitoring can identify patients with muscle invasive bladder cancer who benefit from adjuvant atezolizumab while sparing patients who persistently test ctDNA– from unnecessary treatment
Following Dr. Powles presentation of IMvigor011, the manuscript was concomitantly published in the New England Journal of Medicine.
Presented by: Thomas B. Powles, MBBS, MRCP, MD, Barts Cancer Centre, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): A multicentre, open-label, randomized, phase 3 trial. Lancet Oncol. 2021 Apr;22(4):525-537.
- Powles T, Assaf ZJ, Degaonkar V, et al. Updated overall survival by circulating tumor DNA status from the phase 3 IMvigor010 trial: adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma. Eur Urol. 2024;85(2):114-122.
- Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021 Jl;595(7867):432-437.