(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany was host to the Poster Session. Dr. Benjamin Pradere presented the e-poster Economic evaluation of first-line (1L) treatment strategies for locally advanced or metastatic urothelial carcinoma (la/mUC): Toward optimizing value-based care.
Dr. Pradere began by highlighting that bladder cancer represents the fifth most common malignancy in France, with between 8,300 and 9,500 new cases and over 5,000 deaths annually. Five-year survival rates remain dismal in the metastatic setting, dropping to approximately 5%.
They noted that la/mUC poses not only a clinical challenge but also a significant economic burden, particularly given its poor long-term outcomes. Recent regulatory advances in France have expanded first-line treatment options for platinum-eligible patients, including the approval of EV+P (enfortumab vedotin plus pembrolizumab) in 2024 following the positive results of the EV-302 trial.1 Meanwhile, avelumab maintenance therapy after platinum-based chemotherapy remains an established option, supported by real-world French data from the AVENANCE study.2 Given the varying costs and evolving therapeutic landscape, this study aimed to estimate the economic value of these modern first-line treatments in la/mUC.
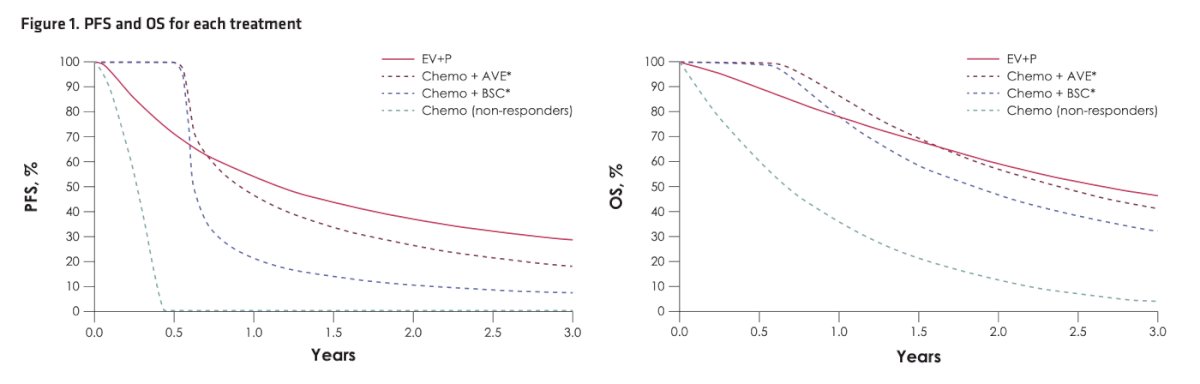
The investigators developed a health economic model to compare the costs and clinical outcomes of two first-line strategies for la/mUC—EV+P versus chemotherapy ± maintenance over a 3-year period. Mean treatment duration, PFS, and OS were estimated using restricted mean survival time, derived from parametric survival analyses. For the chemotherapy-based approach, the model differentiated between three subgroups: patients with controlled disease who received avelumab maintenance (chemo + AVE), those with controlled disease but no maintenance (chemo + best supportive care), and those with uncontrolled disease post-induction (non-responders).
Consistent with the JAVELIN Bladder 100 trial,2 patients in the chemo + AVE and chemo + BSC groups were assumed to remain progression-free and alive for approximately 5.2 and 5.3 months, respectively, before transitioning to trial-based survival outcomes. For the non-responder subgroup, PFS and OS projections were based on the control arm of the KEYNOTE-361 trial. As illustrated in the figure below EV+P demonstrated superior PFS and OS compared to all chemo-based regimens, maintaining higher survival probabilities across the 3-year horizon.
To estimate results for each strategy, the investigators averaged costs and clinical outcomes across subgroups, weighted by the proportion of patients in each disease state. These assumptions were validated through expert consultation with three French medical oncologists and urologists.
Based on their inputs, the model assumed that 72% of patients receiving induction chemotherapy remained progression-free and eligible for maintenance therapy, of whom 81% received AVE. Consequently, among all first-line patients, 58% received chemo + AVE, 14% received chemo + best supportive care (BSC), and 28% had non-responsive disease.
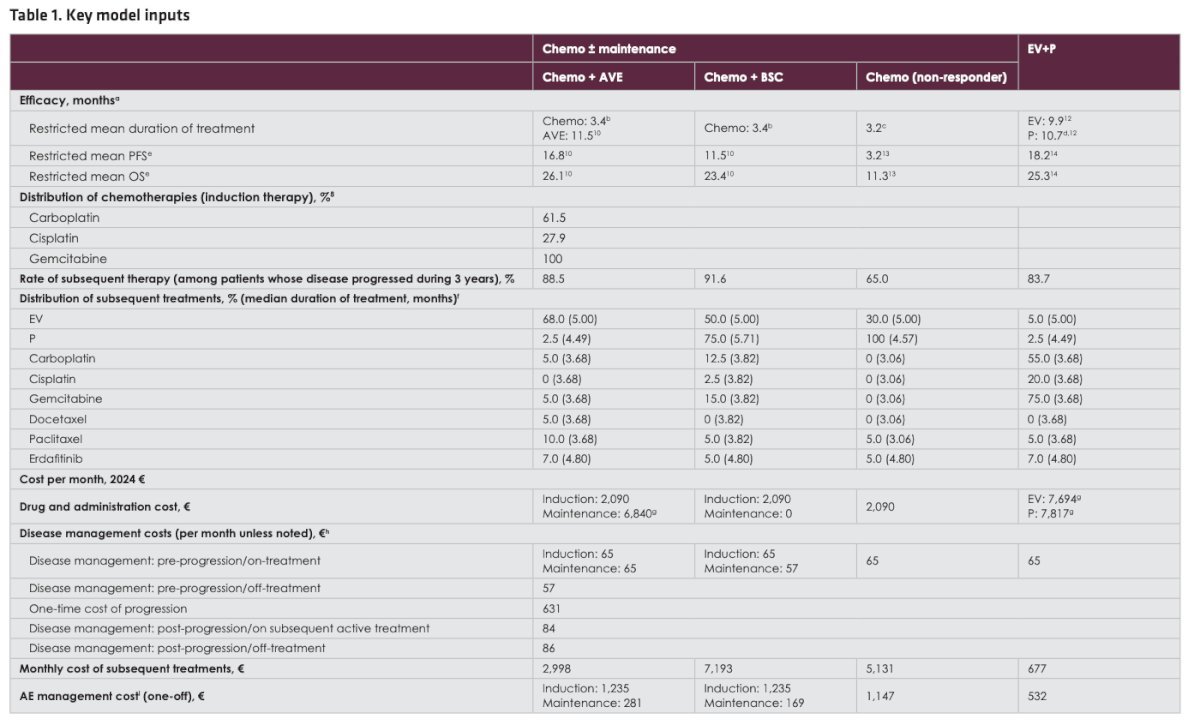
The cost model, expressed in 2024 euros, incorporated drug acquisition and administration, disease management (excluding hospitalization), adverse event management, and subsequent therapy expenses. These data were informed by pivotal trials JAVELIN Bladder 100, EV-302, and KEYNOTE-361 (1-3) and supplemented with pricing from public French databases and literature sources.
Subsequent treatments included pembrolizumab, EV, erdafitinib, and standard chemotherapy, with distribution informed by trial evidence and expert opinion. As summarized in Table 1, model outcomes included:
- 3-year total cost of care per patient
- Cost per month of progression-free and overall survival
- Incremental cost per additional 3-year survivor
- Estimated number of treatable patients and potential survivors within a fixed budget.
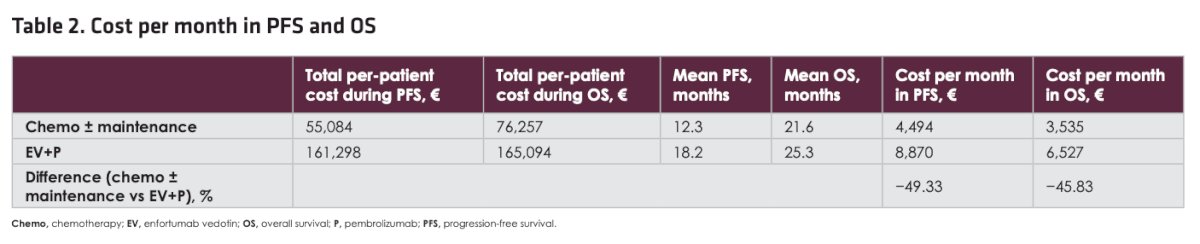
As illustrated in the figure below, the 3-year total cost of care per patient was 54% lower with chemo ± maintenance (€76,257) compared with EV+P (€165,094). This difference was primarily driven by higher drug acquisition costs associated with EV+P. In contrast, patients receiving chemo ± maintenance incurred relatively higher costs related to adverse event management and subsequent therapy use.

Moreover, monthly costs during both PFS and OS were substantially lower with chemo ± maintenance compared to EV+P. The mean cost per month of PFS was €4,494 versus €8,870, and during OS, €3,535 versus €6,527, respectively, representing a 49% and 46% reduction in monthly costs for chemo ± maintenance.
The incremental cost per additional survivor at 3 years for EV+P compared with chemo ± maintenance was estimated at €543,604 over 3 years (or approximately €181,201 annually), reflecting the higher overall expenditure associated with the EV+P regimen despite its improved 3-year OS rate (46.5% vs 30.2%).

Lastly, as shown in Figure 3, under a fixed hypothetical €10,000,000 budget over a 3-year horizon, 131 patients could be treated with chemo ± maintenance compared to 61 patients with EV+P. Correspondingly, 40 patients would be alive at 3 years with chemo ± maintenance versus 28 with EV+P highlighting the greater population-level treatment reach and survival potential associated with the lower-cost strategy.

Dr. Pradere acknowledged several limitations of the analysis. Clinical parameters such as treatment duration, PFS, OS, and AE profiles were derived from clinical trials and assumed to reflect real-world practice in France. Costs and outcomes were based on different data sources—efficacy from clinical trials and cost-related factors such as disease management from published literature and local expert input. To reduce uncertainty, the model used a 3-year time horizon, so outcomes and costs beyond this period were not captured. Additionally, AEs and the efficacy of subsequent treatments were not explicitly included and given the evolving treatment landscape for la/mUC, the regimens used in the reference trials may not fully represent current real-world practice.
Dr. Pradere wrapped up their poster presentation with the following conclusions:
- Healthcare costs associated with treating la/mUC in France remain substantial.
- The estimated total cost of care per patient treated with chemo ± maintenance was €76,257 over 3 years 54% lower than with EV+P (€165,094).
- When adjusted for clinical outcomes, monthly costs during PFS and OS were lower with chemo ± maintenance (€4,494 and €3,535, respectively) compared to EV+P (€8,870 and €6,527, respectively).
- The incremental cost per additional survivor after 3 years for EV+P versus chemo ± maintenance was estimated at €543,604 over 3 years (€181,201 annually).
- Within a fixed 3-year budget, chemo ± maintenance would allow treatment of a higher number of patients and result in more survivors than EV+P.
- These findings highlight the economic burden of la/mUC treatment and support value-based care strategies that integrate cost considerations into shared treatment decision-making.
Presented by: Benjamin Pradere, MD, Department of Urology UROSUD, La Croix Du Sud. Quint-Fonsegrives, France.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Reference:
- Powles T, Valderrama BP, Gupta S, Bedke J, Kikuchi E, Hoffman-Censits J, Iyer G, Vulsteke C, Park SH, Shin SJ, Castellano D, Fornarini G, Li JR, Gümüş M, Mar N, Loriot Y, Fléchon A, Duran I, Drakaki A, Narayanan S, Yu X, Gorla S, Homet Moreno B, van der Heijden MS; EV-302 Trial Investigators. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar 7;390(10):875-888. doi: 10.1056/NEJMoa2312117. PMID: 38446675.
- Bellmunt J, Powles T, Park SH, Voog E, Valderrama BP, Gurney H, Ullén A, Loriot Y, Sridhar SS, Tsuchiya N, Sternberg CN, Aragon-Ching JB, Petrylak DP, Climent Duran MA, Tyroller K, Hoffman J, Jacob N, Grivas P, Gupta S. Avelumab First-line Maintenance for Advanced Urothelial Carcinoma: Long-term Outcomes from the JAVELIN Bladder 100 Trial in Patients with Nonvisceral or Lymph Node-only Disease. Eur Urol. 2025 Oct;88(4):331-338. doi: 10.1016/j.eururo.2025.05.017. Epub 2025 Jun 3. PMID: 40467365.
- Powles T, Csőszi T, Özgüroğlu M, Matsubara N, Géczi L, Cheng SY, Fradet Y, Oudard S, Vulsteke C, Morales Barrera R, Fléchon A, Gunduz S, Loriot Y, Rodriguez-Vida A, Mamtani R, Yu EY, Nam K, Imai K, Homet Moreno B, Alva A; KEYNOTE-361 Investigators. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021 Jul;22(7):931-945. doi: 10.1016/S1470-2045(21)00152-2. Epub 2021 May 26. PMID: 34051178.