(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to the Poster Session. Dr. Giovanni Luigi Pastorino presented the poster Circulating immune-biomarkers of response to neoadjuvant Sacituzumab Govitecan (SG) alone and with pembrolizumab (pembro) in muscle-invasive bladder cancer (MIBC): secondary analyses from SURE-01 and SURE-02 trials.
Dr. Pastorini began by highlighting the current treatment landscape in muscle-invasive bladder cancer (MIBC), emphasizing that bladder cancer is the 4th most commonly diagnosed malignancy among men. For patients with locally advanced disease (T2–T4N0M0), radical cystectomy remains the standard of care. While cisplatin-based neoadjuvant chemotherapy provides about a 5% improvement in 5-year overall survival, up to 50% of patients are deemed cisplatin-ineligible. Despite optimal management, over 40% of patients experience metastatic progression within two years, underscoring the unmet need for effective strategies in both cisplatin-eligible and ineligible populations, as well as potential bladder-sparing alternatives.
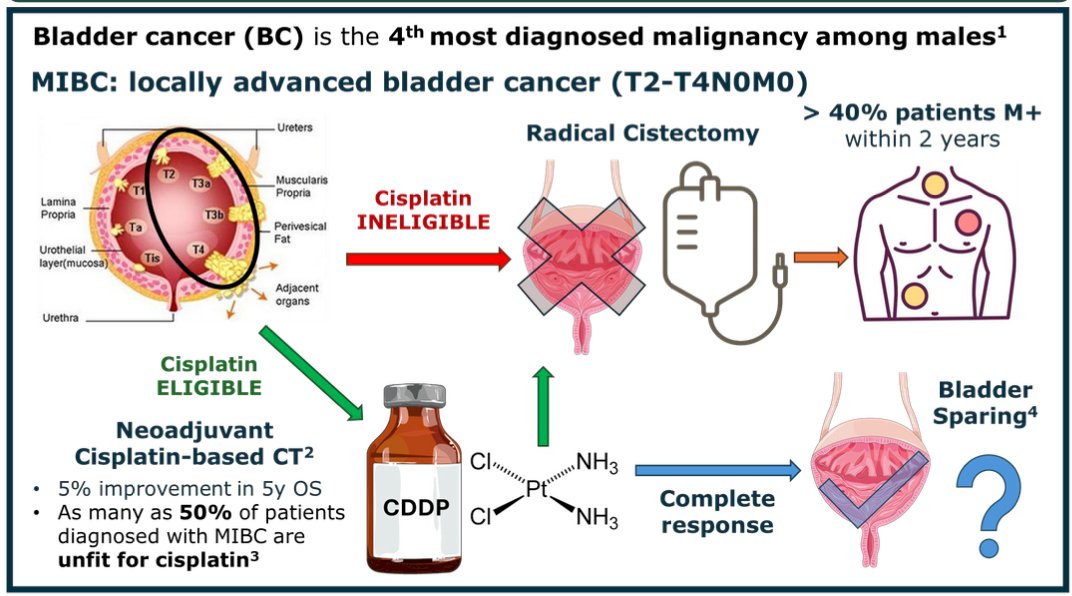
Sacituzumab govitecan (SG) has demonstrated efficacy in metastatic bladder cancer, both as monotherapy (TROPHY-U-01) and in combination with pembrolizumab ((TROPHY-U-01 cohort 3). Pembrolizumab has also shown strong activity in the perioperative setting, as seen in PURE-01. (1) However, no predictive biomarkers of response to SG or SG + pembrolizumab have been identified.
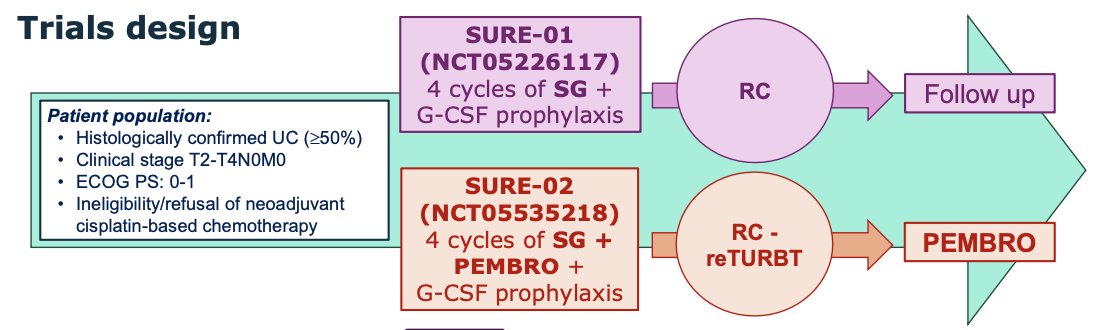
The SURE trials aim to evaluate these agents in cisplatin-ineligible patients with muscle-invasive bladder cancer (T2–T4N0M0, ECOG 0-1). SURE-01 (NCT05226117) tests four cycles of SG plus G-CSF prophylaxis before radical cystectomy, while SURE-02 (NCT05535218) combines SG + pembrolizumab followed by surgery or re-TURBT and adjuvant pembrolizumab. The study designs are shown below.
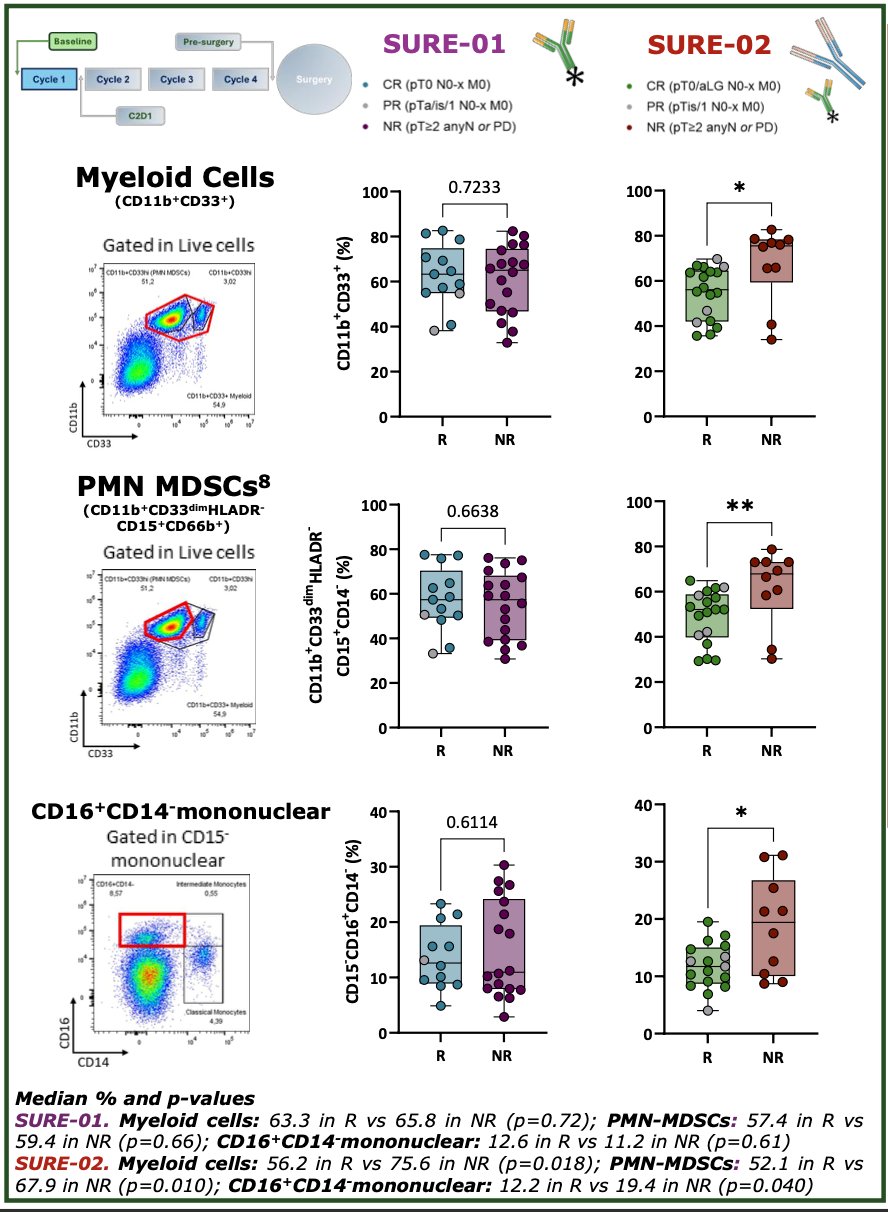
For this analysis, peripheral blood samples were collected at baseline, during treatment cycles, and prior to surgery from patients enrolled in the SURE-01 and SURE-02 trials. Major responders (ypT≤1N0M0) were compared with non-responders (ypT≥2 or with nodal/metastatic progression) at each timepoint. Multiparametric flow cytometry was performed on fresh samples using a 13-marker myeloid-targeted antibody panel (including MERTK, LOX-1, CD11b, CD14, CD15, CD16, and CD33, among others), acquired via CytoFLEX LX and analyzed with FlowJo software. Statistical analyses included unpaired t-tests or Mann-Whitney tests for independent comparisons and paired t-tests or Wilcoxon tests for longitudinal analyses. Results reflect data updated through June 2025.
At baseline, a lower proportion of PMN-MDSCs and CD16⁺CD14⁻ mononuclear cells was associated with major response in patients treated with SG + pembrolizumab, but not in those receiving SG monotherapy. In the SURE-02 cohort, responders had significantly fewer myeloid cells (56.2% vs 75.6%, p=0.018), PMN-MDSCs (52.1% vs 67.9%, p=0.010), and CD16⁺CD14⁻ mononuclear cells (12.2% vs 19.4%, p=0.040) compared to non-responders. In contrast, in the SURE-01 cohort (SG alone), no significant differences were observed between responders and non-responders across these cell subsets.
In the longitudinal analysis, an increase in CD16⁻ immature PMNs was observed among non-responders treated with SG monotherapy between baseline and C2D1, while responders in both treatment arms demonstrated a reduction in these cells from baseline to pre-surgery. A lower percentage of post-treatment immature PMNs correlated with major response to SG monotherapy. Specifically, in SURE-01, responders showed a significant decrease in immature PMNs from baseline to pre-surgery (p=0.009), whereas non-responders had an increase (p=0.036). In SURE-02, responders also exhibited a decline in immature PMNs (p=0.039). Overall, these findings suggest that reduced circulating immature PMNs and increased monocyte differentiation are linked to better response, particularly in patients receiving pembrolizumab.
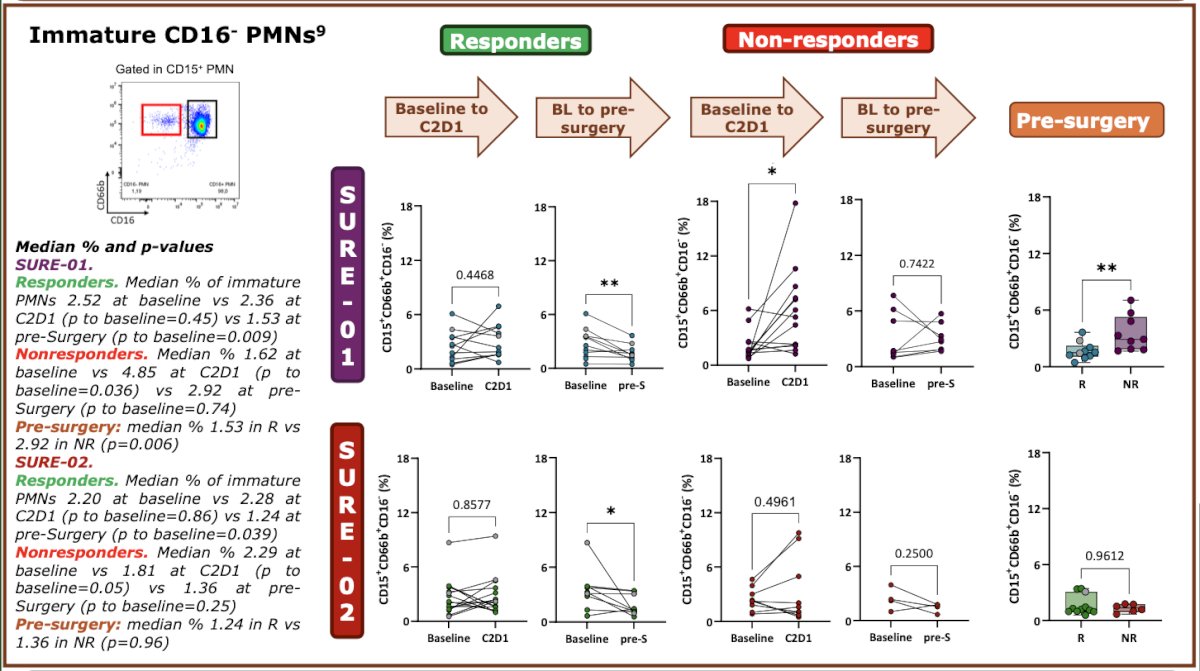
Moreover, immature PMNs, which can accumulate under chronic inflammation and exhibit immunosuppressive activity, were reduced in responders across both treatment arms. Monocytes appeared to contribute to anti-tumor immunity by migrating to tissues and differentiating into antigen-presenting cells. Importantly, pre-treatment circulating immune signatures were associated with response to pembrolizumab, while response to both regimens correlated with lower levels of immature PMNs. Additionally, higher post-treatment percentages of circulating monocyte subsets were linked to response in patients receiving SG monotherapy.
Dr. Pastorino emphasized that, prior to surgery, a higher percentage of classical (CD14⁺CD16⁻) and intermediate (CD14⁺CD16⁺) monocytes was associated with a major response to SG monotherapy. Specifically, responders showed significantly higher proportions of classical monocytes (median 10.6% vs 2.2%, p=0.044) and intermediate monocytes (1.36% vs 0.39%, p=0.045) compared with non-responders, suggesting that expansion of these monocyte subsets may play a role in effective immune activation in response to treatment.

Dr. Pastorino concluded by highlighting the next steps for the SURE program, which include completing study cohort analyses and expanding biomarker research through integration with tumor mutational burden (TMB), transcriptomic, genomic, and radiomic data to refine response prediction. Further work will focus on evaluating circulating PBMCs alongside the tumor microenvironment and conducting in vitro immunosuppression assays to functionally assess immune cell subsets associated with resistance to therapy.
Presented by: Giovanni Luigi Pastorino, Medical Oncology Department, IRCCS San Raffaele Hospital, Milan, Italy
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Referene:
- Loriot Y, Petrylak DP, Rezazadeh Kalebasty A, Fléchon A, Jain RK, Gupta S, Bupathi M, Beuzeboc P, Palmbos P, Balar AV, Kyriakopoulos CE, Pouessel D, Sternberg CN, Tonelli J, Sierecki M, Zhou H, Grivas P, Barthélémy P, Tagawa ST. TROPHY-U-01, a phase II open-label study of sacituzumab govitecan in patients with metastatic urothelial carcinoma progressing after platinum-based chemotherapy and checkpoint inhibitors: updated safety and efficacy outcomes. Ann Oncol. 2024 Apr;35(4):392-401. doi: 10.1016/j.annonc.2024.01.002. Epub 2024 Jan 18. PMID: 38244927.