(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to the Poster Session. Dr. Richard Cathomas presented the poster Perioperative chemo-immunotherapy with Durvalumab for operable muscle-invasive urothelial carcinoma (MIUC): final analysis of the single arm phase II trial SAKK 06/17.
Dr. Cathomas began by noting that the primary analysis of SAKK 06/17 had been previously published and met its primary endpoint of 2-year event-free survival (EFS). Since then, a phase 3 trial with a similar perioperative design using durvalumab also demonstrated significant improvements in EFS, pathological complete response (pCR), and overall survival (OS). (1) He presented the final analysis of SAKK 06/17, with a median follow-up of 64 months.
SAKK 06/17 was a single-arm, open-label, multicenter phase II trial that enrolled 57 patients with resectable muscle-invasive bladder cancer (MIBC). Patients received four cycles of neoadjuvant gemcitabine/cisplatin combined with durvalumab, followed by radical cystectomy and adjuvant durvalumab. The primary endpoint was 2-year event-free survival (EFS).
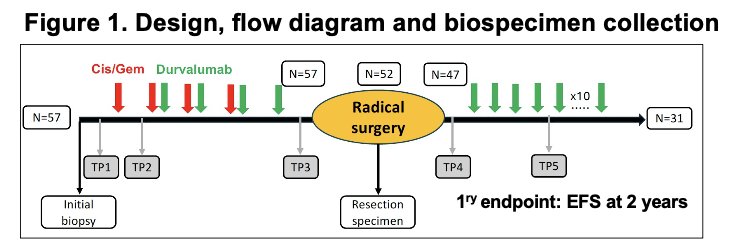
The median age was 68 years, with 79% male and 97% bladder primaries. Most patients had cT2 disease (70%), with cN1 in 16%. Translational analyses included next-generation sequencing of 90 genes, cytokine profiling, and T-cell receptor repertoire assessment to explore immune and genomic correlates of treatment response.
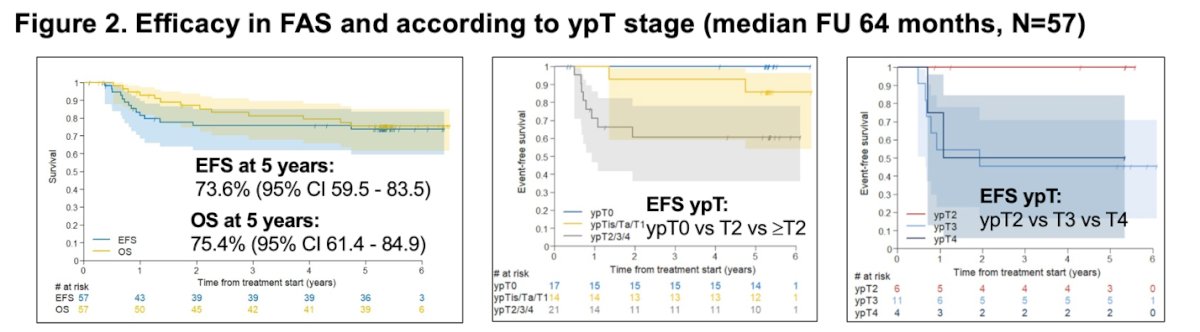
At a median follow-up of 64 months, the final analysis showed durable long-term outcomes, with a 5-year event-free survival rate of 73.6% and overall survival of 75.4%. Outcomes were strongly associated with pathological stage after neoadjuvant therapy, patients achieving ypT0 or ypT1 status demonstrated markedly better EFS compared to those with ≥ypT2 disease, confirming the prognostic relevance of pathological downstaging in this cohort.
Cytokine profiling in 20 patients revealed distinct immune patterns between responders and non-responders. Patients achieving pCR showed transient increases in myeloid-related cytokines (CXCL1, CXCL2, CXCL12, CCL13) after neoadjuvant therapy, followed by elevations in effector T-cell–associated cytokines (CXCL9, CXCL10) post-adjuvant durvalumab. These findings suggest that treatment-induced immune activation and effective T-cell recruitment may underlie durable pathological responses.
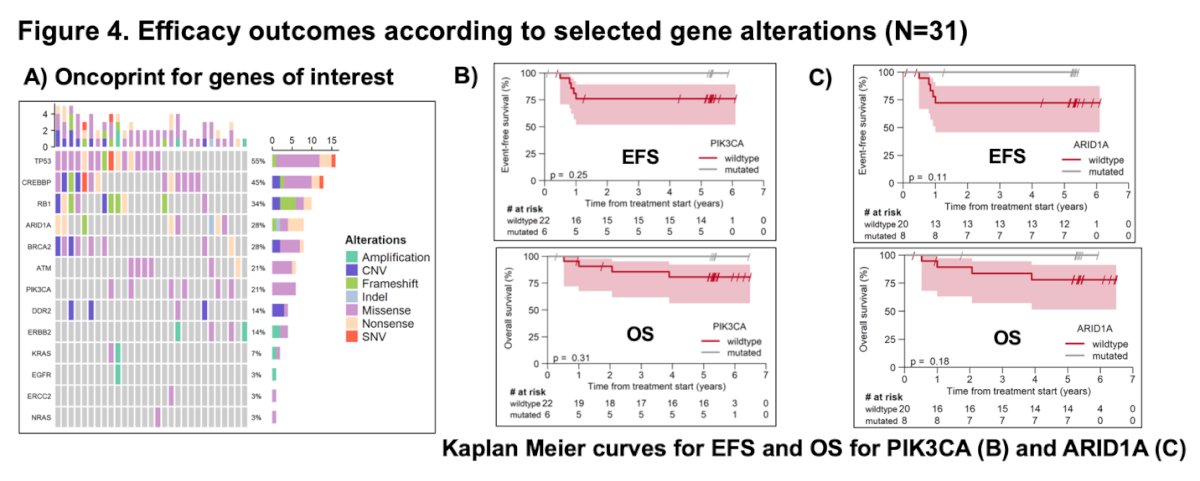
Moreover, Dr Cathomas reported that genomic profiling of 31 patients identified frequent alterations in TP53 (55%), ARID1A (26%), and PIK3CA (23%). Exploratory analyses suggested that mutations in PIK3CA and ARID1A were not significantly associated with differences in event-free or overall survival, though both genes showed numerically shorter survival trends compared to wild-type cases. These findings highlight the heterogeneity of molecular drivers in MIBC and the need for larger datasets to clarify the prognostic impact of specific genomic alterations in the context of perioperative chemo-immunotherapy.
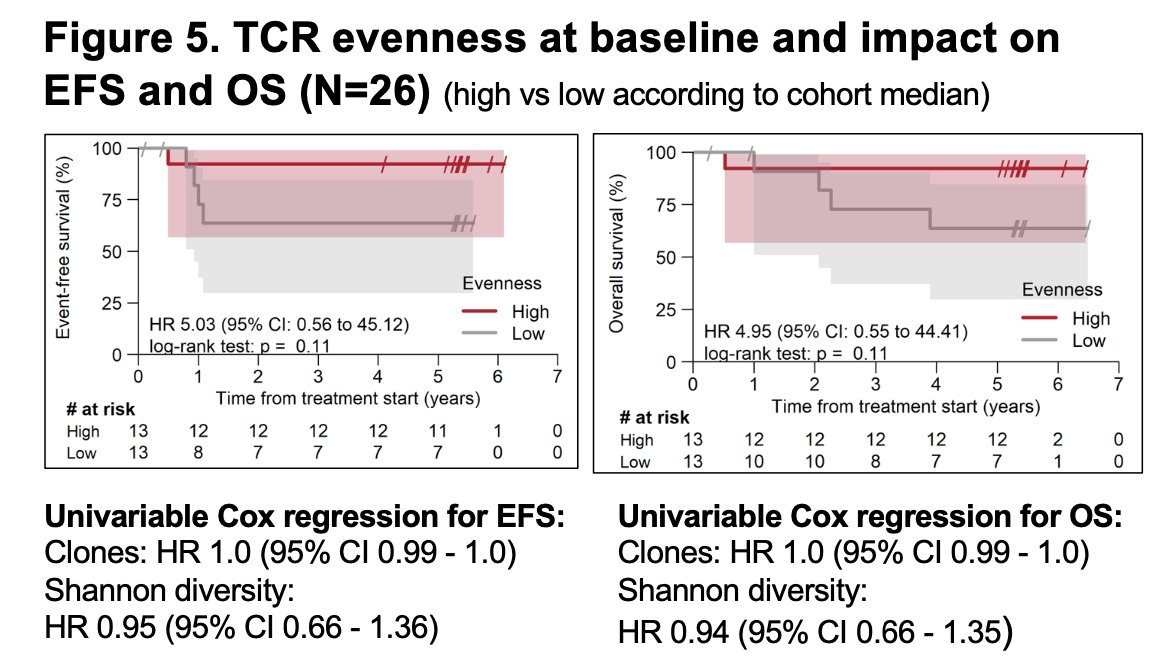
Lastly, the investigators found that patients with higher baseline T-cell receptor (TCR) evenness, a measure of balanced T-cell clone distribution tended to have longer event-free and overall survival compared to those with lower evenness, although this did not reach statistical significance (p = 0.11). While exploratory, these findings suggest that greater TCR diversity may reflect a more adaptable antitumor immune repertoire, potentially contributing to improved long-term outcomes with perioperative chemo-immunotherapy.
Dr. Cathomas concluded his presentation with the following key remarks:
- Perioperative chemo-immunotherapy with durvalumab maintained durable efficacy, with high EFS and OS after a median follow-up exceeding 5 years.
- Biomarker analyses from SAKK 06/17 provide valuable insights into the biological mechanisms driving response in MIUC.
- No distinct predictive marker was identified, although several findings were hypothesis-generating.
- Ongoing translational studies aim to further characterize immune dynamics through multiparameter spatial analyses of the tumor microenvironment.
Presented by: Richard Cathomas, MD, Head of the Divison of Oncology/Hematology at the Kantonsspital Graubünden, Chur, Switzerland
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Reference: