(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany was host to the Poster Session. Dr. Patrizia Giannatempo presented the poster Impact of Dose Reductions on the Efficacy of Erdafitinib (Erda) in Patients (Pts) with Advanced or Metastatic Urothelial Carcinoma (mUC): A Post-hoc Analysis of the Phase 3 THOR Study Cohort-1 Evaluating Erda versus Chemotherapy (Chemo).
Dr. Giannatempo began by noting that erdafitinib, a pan-fibroblast growth receptor (FGR) inhibitor, is approved for patients with unresectable or metastatic urothelial carcinoma (mUC) harboring susceptible FGFR3 alterations who have progressed on or after at least one prior PD-(L)1 inhibitor. This approval was based on the phase 3 THOR study, which demonstrated a significant overall survival (OS) benefit for erdafitinib compared to investigator’s choice of chemotherapy. At a median follow-up of 15.9 months, median OS was 12.1 months with erdafitinib versus 7.8 months with chemotherapy (HR 0.64; 95% CI 0.47–0.88; P=0.005). (1)
In THOR, dose reductions of erdafitinib were allowed to manage adverse events, and this analysis aimed to evaluate the impact of those dose reductions on efficacy outcomes.1
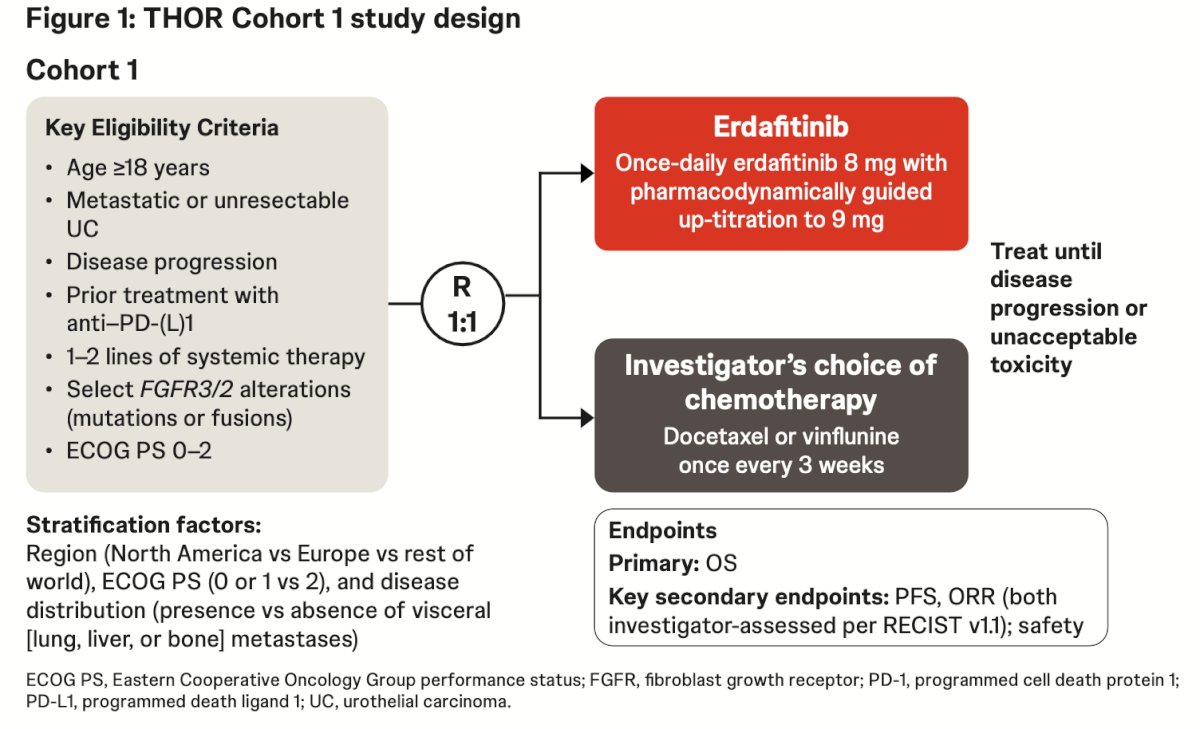
Birefly, THOR was a phase 3, randomized, open-label, global study enrolling adults with advanced or metastatic urothelial carcinoma harboring FGFR3/2 alterations who had progressed after 1–2 prior systemic therapies, including a PD-(L)1 inhibitor. Patients were randomized 1:1 to receive erdafitinib (8 mg daily with optional uptitration to 9 mg) or investigator’s choice of chemotherapy (docetaxel or vinflunine). This exploratory analysis assessed overall survival (OS), progression-free survival (PFS), and objective response rate (ORR) according to the number of erdafitinib dose reductions (0, 1, or ≥2), with dose reduction defined as any decrease from 8 mg to ≤6 mg. The study schema is shown below
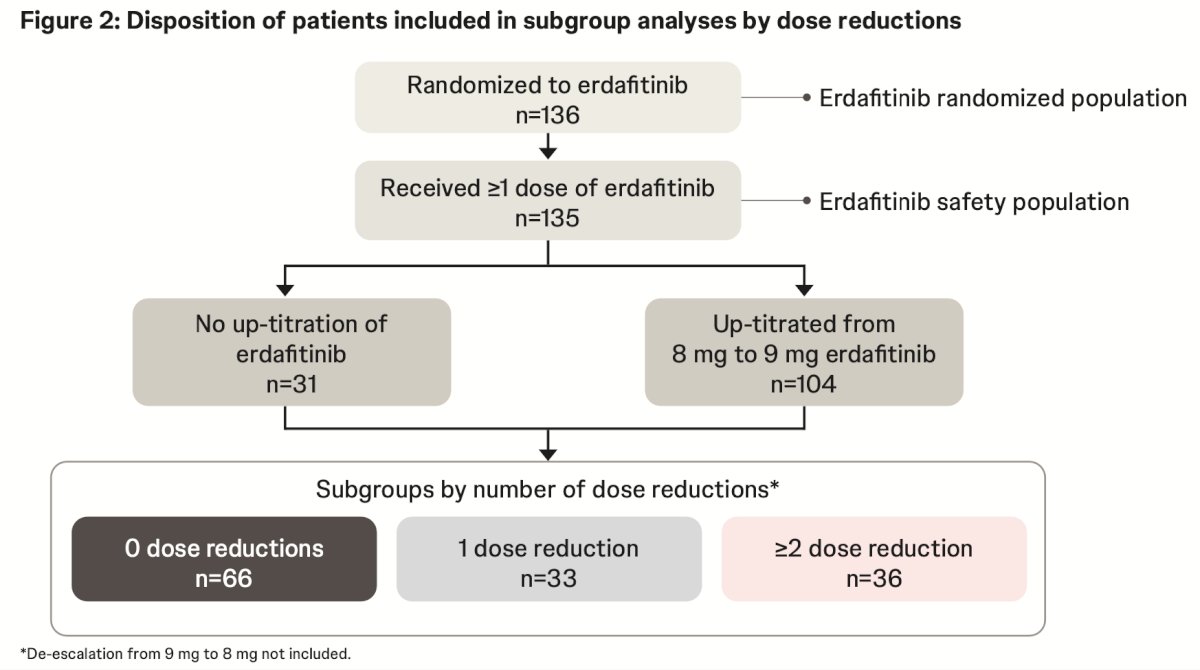
For this analysis, data were evaluated using the clinical cutoff of January 15, 2023. Among 136 patients randomized to erdafitinib in Cohort 1, 66 (48.5%) had no dose reductions, 33 (24.3%) had one dose reduction, and 36 (26.5%) had two or more. Of the 104 patients who up-titrated from 8 mg to 9 mg, 47.2% required at least one dose reduction, while among those who did not up-titrate, 71% required at least one reduction. Overall, dose reductions were common and occurred across both titration groups, as summarized in Figure 2.
Baseline demographics and clinical characteristics were generally comparable across patients with 0, 1, or ≥2 erdafitinib dose reductions. Median age ranged from 65 to 70 years across subgroups, and most patients were male, White, and had lower tract primary tumors with visceral metastases as illustrated in the table below.

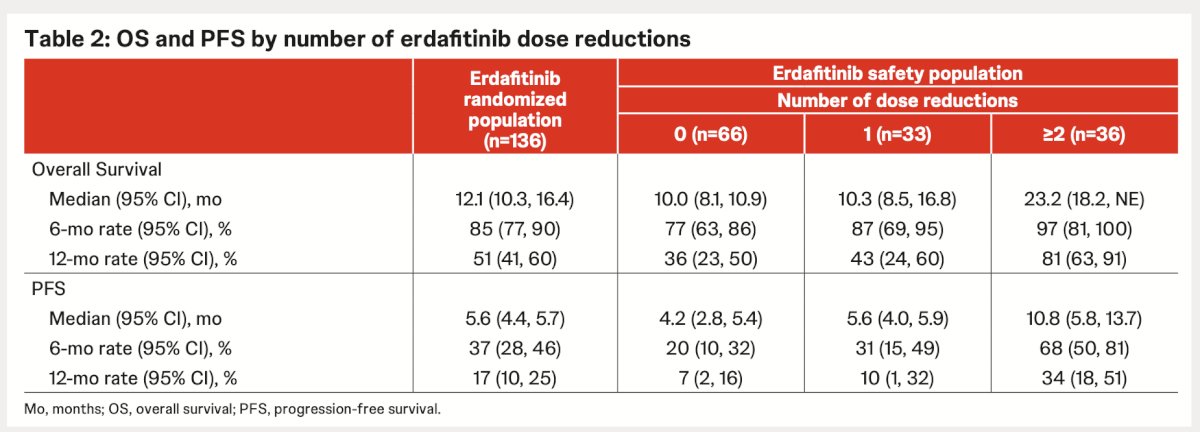
At a median follow-up of 15.9 months (18.0 months for erdafitinib and 14.9 months for chemotherapy), median OS in the erdafitinib group was 12.1 months compared to 7.8 months with chemotherapy. Median PFS was 5.6 months with erdafitinib versus 2.7 months with chemotherapy. Notably, within the erdafitinib-treated cohort, patients who required ≥2 dose reductions achieved the longest median OS (23.2 months) and PFS (10.8 months), suggesting that dose reductions did not negatively impact efficacy outcomes.
Unconfirmed ORR was 45.6% with erdafitinib compared to 11.5% with chemotherapy, while confirmed ORR was 35.3% versus 8.5%, respectively. Within the erdafitinib-treated group, higher response rates were observed among patients who required dose reductions, reaching 63.9% in those with ≥2 reductions compared to 33.3% in those without.

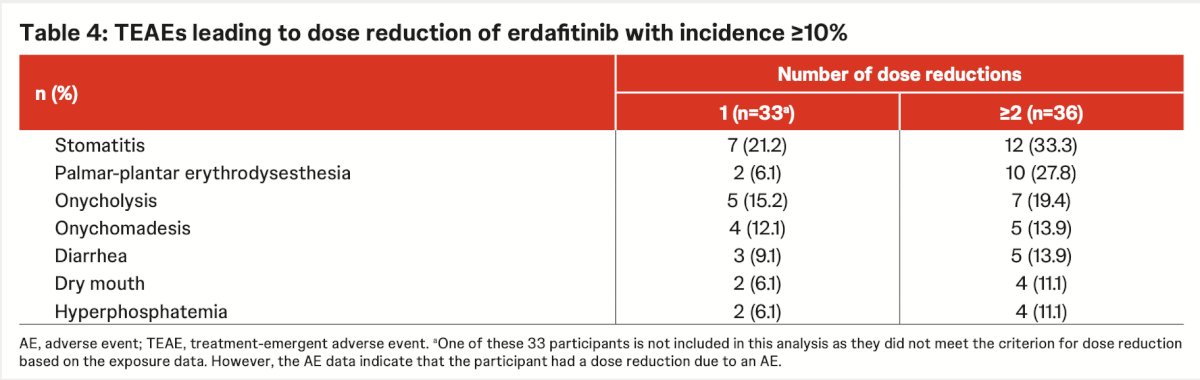
he most common treatment-emergent adverse events (TEAEs) leading to erdafitinib dose reductions were stomatitis, palmar-plantar erythrodysesthesia, and onycholysis. The mean treatment duration among patients who required dose reductions was similar to the overall safety population (283.8 vs 206.8 days). Stomatitis occurred in up to one-third of patients with ≥2 dose reductions, followed by palmar-plantar erythrodysesthesia (27.8%) and nail-related toxicities, indicating that these manageable adverse events were the primary drivers of dose modification.
Dr Giannatempo concluded her presentation with the following key takeaways:
- In the phase 3 THOR study (Cohort 1) involving patients with advanced or metastatic urothelial carcinoma, erdafitinib dose reductions due to treatment-emergent adverse events were frequent but did not appear to compromise efficacy, underscoring the value of proactive toxicity management to balance safety and outcomes.
• Approximately half of patients treated with erdafitinib required at least one dose reduction, most commonly due to stomatitis, palmar-plantar erythrodysesthesia, or onycholysis.
• Baseline demographic and clinical characteristics were similar among patients with 0, 1, or ≥2 dose reductions.
• Erdafitinib maintained its efficacy across all subgroups, with comparable OS, PFS, and ORR outcomes, despite frequent dose modifications.
Presented by: Patrizia Giannatempo, MD, Genitourinary Medical Oncology, Fondazione IRCCS - Istituto Nazionale dei Tumori. Milan, Italy.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Reference:
- Loriot Y, Matsubara N, Park SH, Huddart RA, Burgess EF, Houede N, Banek S, Guadalupi V, Ku JH, Valderrama BP, Tran B, Triantos S, Kean Y, Akapame S, Deprince K, Mukhopadhyay S, Stone NL, Siefker-Radtke AO; THOR Cohort 1 Investigators. Erdafitinib or Chemotherapy in Advanced or Metastatic Urothelial Carcinoma. N Engl J Med. 2023 Nov 23;389(21):1961-1971. doi: 10.1056/NEJMoa2308849. Epub 2023 Oct 21. PMID: 37870920.