(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to the Poster Session. Dr. Richard Cathomas presented the poster Intravesical recombinant BCG followed by perioperative chemo-immunotherapy (chemo-IO) for patients with muscle-invasive bladder cancer (MIBC): interim analysis of SAKK 06/19 study.
Dr. Cathomas began by emphasizing that integrating immunotherapy into the perioperative management of muscle-invasive bladder cancer (MIBC) is both feasible and effective, with evidence showing improvements in event-free and overall survival, as well as higher pathological complete response rates, though these remain below 40%.1,2
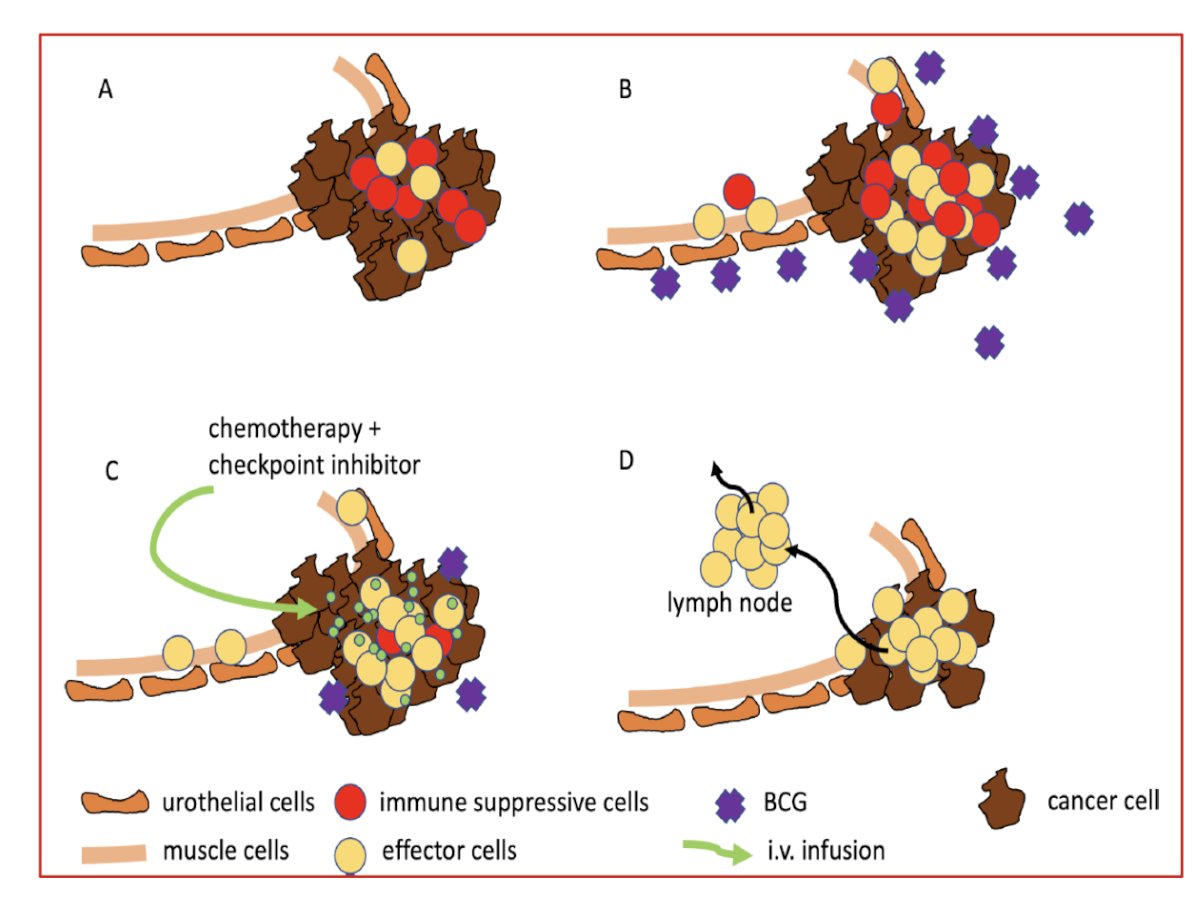
He explained that intravesical BCG, long used in non–muscle-invasive disease, induces local inflammation and activates both innate and adaptive immune responses. Building on this concept, a novel recombinant BCG vaccine (VPM1002BC) has been developed and demonstrated favorable safety and promising efficacy in BCG-exposed NMIBC patients in the SAKK 06/14 trial.3
The figure below illustrates how intravesical VPM1002BC is proposed to enhance anti-tumor immunity when combined with systemic chemo-immunotherapy. By inducing local immune activation within the bladder and promoting effector cell recruitment, this approach aims to generate a stronger systemic immune response capable of improving tumor clearance and overall treatment efficacy in MIBC.
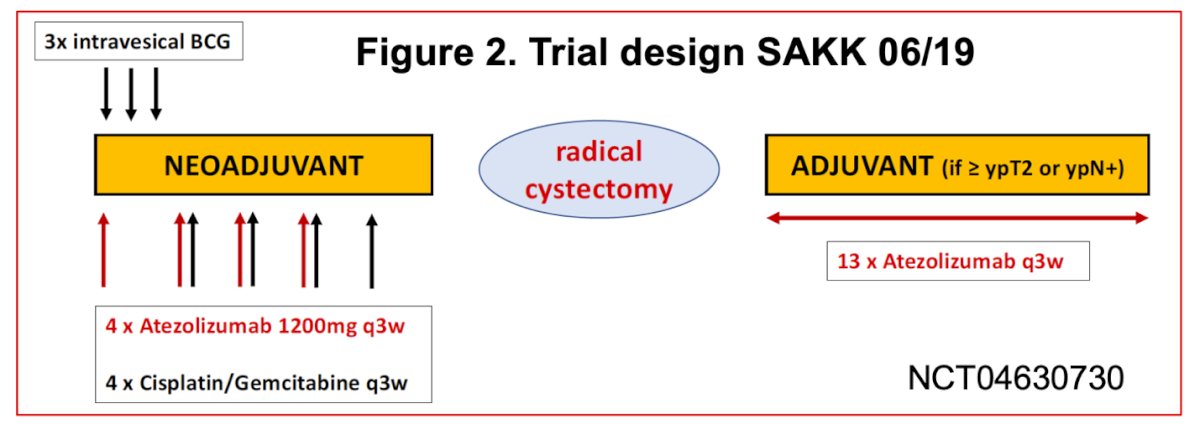
The phase II SAKK 06/19 trial (NCT04630730) is an open-label, single-arm study enrolling patients with operable pT2 or cT2–T4a cN0–1 MIBC eligible for cisplatin-based therapy. Patients received three intravesical instillations of BCG followed by four cycles of neoadjuvant gemcitabine/cisplatin plus atezolizumab before radical cystectomy. Those with residual disease (≥ypT2 or ypN+) were offered 13 additional cycles of adjuvant atezolizumab. The primary endpoint is pathological complete remission (pCR) at cystectomy, with secondary endpoints including event-free survival, overall survival, recurrence-free survival, response rate, and treatment feasibility. The study schema is shown below.
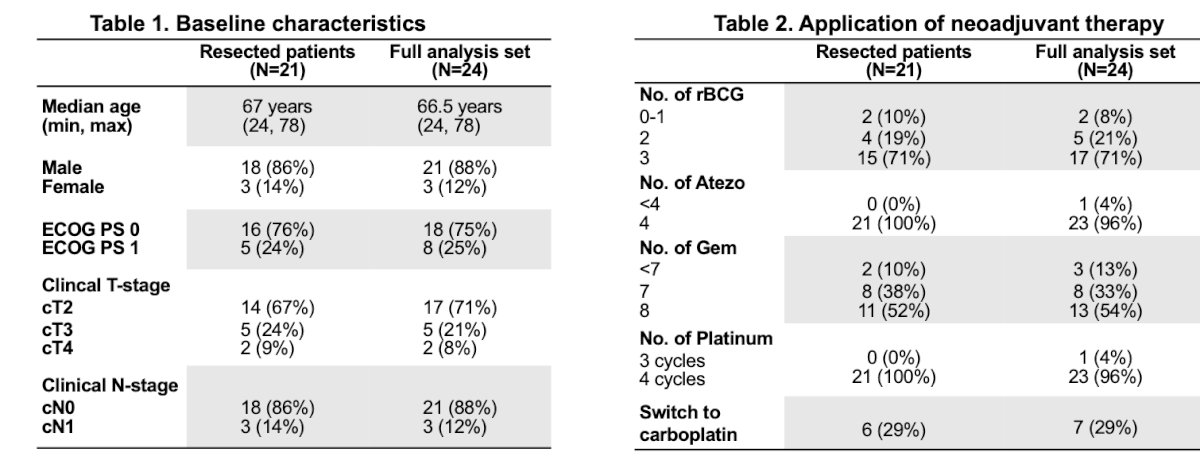
A total of 47 patients were enrolled between April 2022 and April 2025, with accrual temporarily suspended due to an out-of-specification batch of VPM1002BC. The interim analysis included 24 patients in the full analysis and safety set, of whom 21 underwent radical cystectomy (3 opted for bladder-sparing therapy). The median age was 67 years, and most patients were male (86–88%) with ECOG 0–1 and cT2N0 disease.
Nearly all patients completed four cycles of atezolizumab and platinum-based chemotherapy, with 29% requiring a switch to carboplatin. Compliance with the planned three intravesical BCG instillations was high (71%). Surgery was performed laparoscopically in 76% of patients, open in 14%, and mixed in 10%. Urinary diversion consisted of neobladder in 57% and ileal conduit in 43%. Among 21 evaluable patients, at least 9 achieved a pCR.
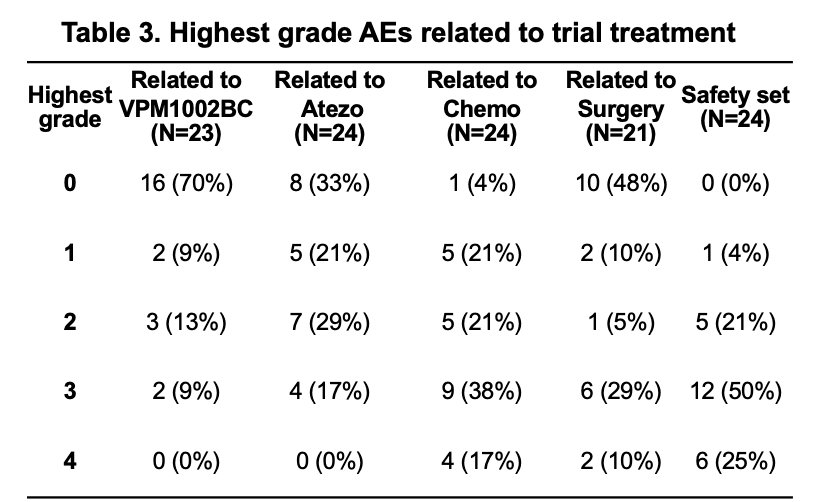
Treatment-related adverse events were generally manageable. Most events related to intravesical VPM1002BC were grade 0–2, with only 9% experiencing grade 3 events. Atezolizumab was associated with grade 3 events in 17% of patients, and chemotherapy in 38%. Surgical complications were primarily grade 0–3, with 10% experiencing grade 4 events. Overall, half of the patients in the safety set experienced grade 3 and 25% grade 4 adverse events, indicating acceptable tolerability across treatment components.
Dr. Cathomas concluded his presentation by emphasizing that the combination of intravesical recombinant BCG (VPM1002BC) with perioperative chemo-immunotherapy was both feasible and well-tolerated, with no unexpected toxicities observed. The interim analysis met the predefined efficacy and safety criteria, supporting continuation of the trial into stage 2.
Presented by: Richard Cathomas, MD, Head of the Divison of Oncology/Hematology at the Kantonsspital Graubünden, Chur, Switzerland
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
Reference:
- Szabados B, Rodriguez-Vida A, Durán I, Crabb SJ, Van Der Heijden MS, Pous AF, Gravis G, Herranz UA, Protheroe A, Ravaud A, Maillet D, Mendez-Vidal MJ, Suárez C, Linch M, Prendergast A, Tyson C, Mousa K, Castellano D, Powles T. Toxicity and Surgical Complication Rates of Neoadjuvant Atezolizumab in Patients with Muscle-invasive Bladder Cancer Undergoing Radical Cystectomy: Updated Safety Results from the ABACUS Trial. Eur Urol Oncol. 2021 Jun;4(3):456-463. doi: 10.1016/j.euo.2020.11.010. Epub 2021 Feb 18. PMID: 33612455.
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Petrausch U, Spahn M, Schneider M, Hayoz S, Rentsch CA, Rothschild S, Omlin A, Cathomas R. Novel sequential treatment strategy for patients with muscle-invasive bladder cancer (MIBC): intravesical recombinant BCG, followed by neoadjuvant chemoimmunotherapy, radical cystectomy plus pelvic lymphadenectomy and adjuvant immunotherapy - protocol of a multicentre, single arm phase 2 trial (SAKK 06/19). BMJ Open. 2023 Jun 7;13(6):e067634. doi: 10.1136/bmjopen-2022-067634. PMID: 37286312; PMCID: PMC10255003..