(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress, held in Berlin, Germany, between October 17th and 21st, was host to the session Presidential Symposium 1. Dr. Jonathan Rosenberg discussed the late-breaking abstract: Perioperative (enfortumab vedotin (EV) plus pembrolizumab (pembro) in participants (pts) with muscle-invasive bladder cancer (MIBC) who are cisplatin-ineligible: The phase 3 KEYNOTE-905 study.
Dr. Rosenberg emphasized that for the first time, it has been shown that enfortumab vedotin plus pembrolizumab provides substantial clinical benefit for patients with MIBC who are cisplatin-ineligible or who decline cisplatin. The regimen can be delivered safely without increased surgical mortality, and adjuvant therapy is generally well tolerated. However, he noted that further work is needed to clarify the relative contribution of each treatment phase.
Given that nearly half of MIBC patients are cisplatin-ineligible per Galsky criteria due to renal impairment, poor performance status, neuropathy, or cardiac dysfunction, this combination offers an important therapeutic option for a population unable to receive optimal cisplatin-based therapy.2
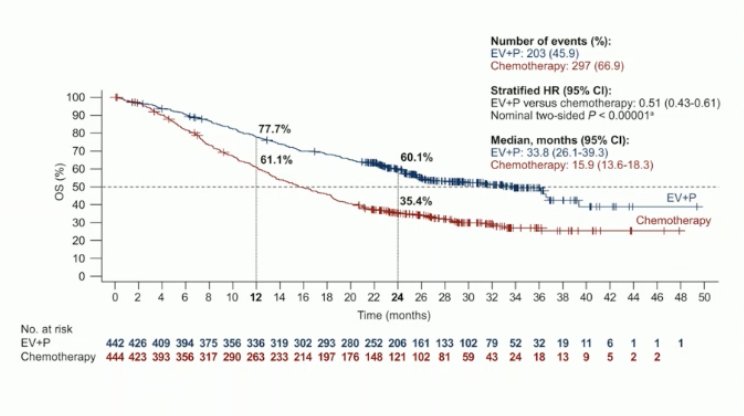
The EV-302 trial established enfortumab vedotin plus pembrolizumab as the new standard of care for patients with locally advanced or metastatic urothelial carcinoma, regardless of cisplatin eligibility. The combination significantly improved survival outcomes compared to chemotherapy, with consistent benefit across subgroups and, as Dr. Rosenberg noted, may even offer the potential for cure in select metastatic patients.1 These results provided the scientific rationale for evaluating the regimen in the perioperative setting in KEYNOTE-905.
Patients who are ineligible for cisplatin often present with significant comorbidities that contribute to competing risks of death, making EFS an appropriate primary endpoint in this population. Until now, adjuvant nivolumab has been the only approved perioperative therapy, established as standard of care in the United States since 2021 based on CheckMate 274, and in Europe for PD-L1–positive patients since 2022.4
Dr. Rosenberg emphasized that KEYNOTE-905 enrolled a distinctly different perioperative population compared to prior bladder cancer trials older patients, a higher proportion with ECOG 2 status, and nearly 80% who were cisplatin-ineligible, most commonly due to renal impairment underscoring the trial’s relevance to real-world clinical practice.
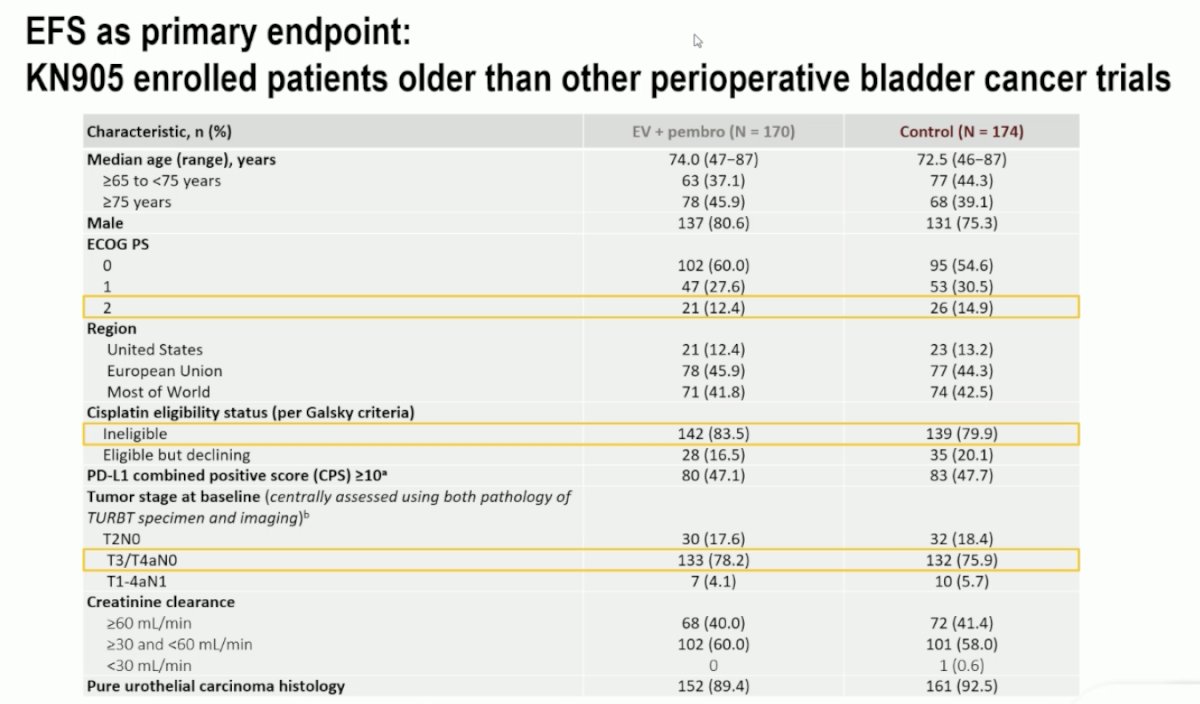
Dr. Rosenberg emphasized that KEYNOTE-905 enrolled an older and more comorbid population than previous perioperative bladder cancer trials, with a median age of 74 years in the experimental arm and nearly half of patients aged ≥75. By comparison, median ages were 63–66 years in cisplatin-eligible trials such as NIAGARA and VESPER, and 65–69 years in mixed-eligibility studies including CheckMate 274, AMBASSADOR, and EV-302.3-6 These findings underscore that perioperative EV + pembrolizumab is both feasible and safe even in older patients typically excluded from cisplatin-based regimens.
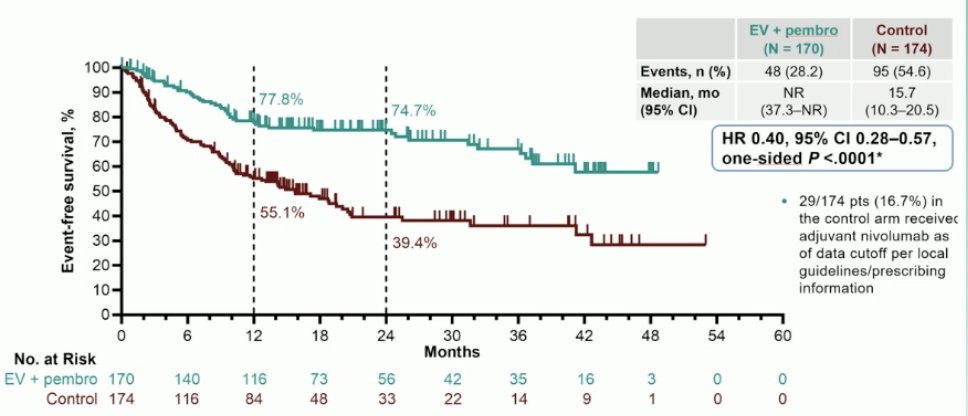
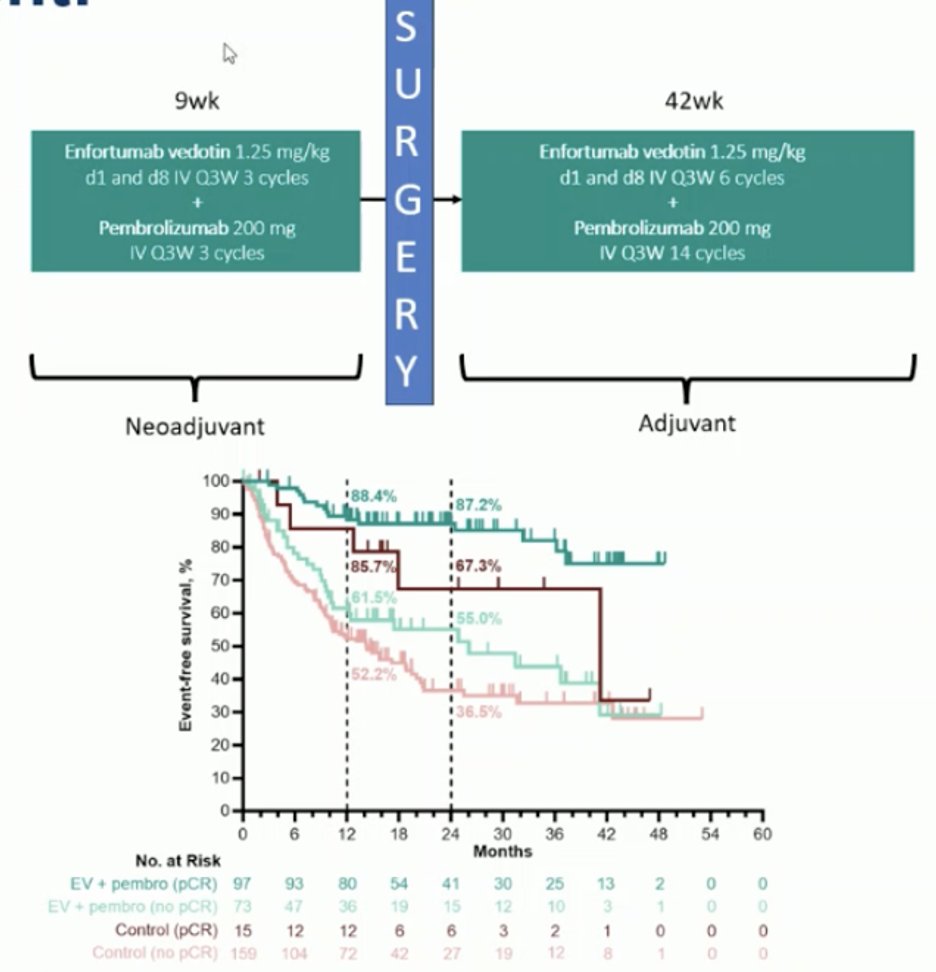
There was a dramatic improvement in EFS favoring EV + pembrolizumab (HR 0.40, 95% CI 0.28–0.57; p < 0.0001), with early and sustained separation of the curves. Dr. Rosenberg noted that in an older, comorbid population, EFS benefit must be interpreted in the context of treatment tolerability, ability to deliver therapy, and the magnitude of overall survival improvement.
Surgery was feasible in patients receiving EV + pembrolizumab, with 87.6% undergoing RC compared to 89.7% in the control arm, rates comparable to those seen in the cisplatin-eligible NIAGARA trial.3 Grade 5 adverse events during surgery were low and numerically lower with EV + pembrolizumab (2.7% vs 5.7%). Grade ≥3 AEs were more frequent in the EV + pembrolizumab arm (71.3% vs 45.9%), consistent with prior EV data and expected in this frailer population. Overall, toxicity remained manageable and did not compromise surgical feasibility.
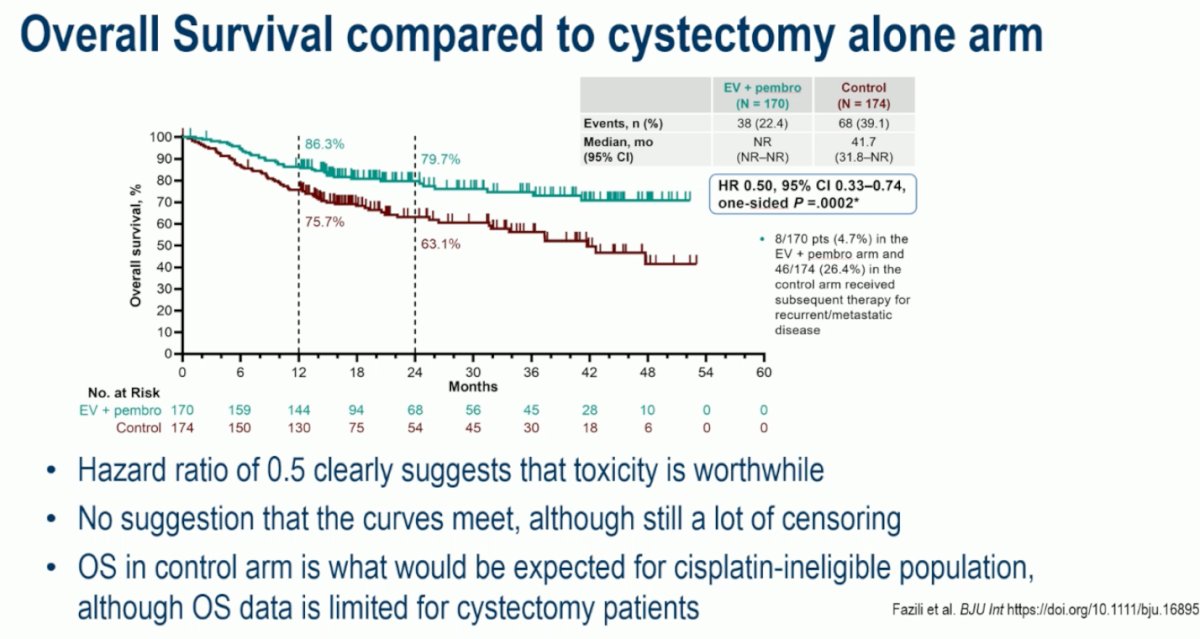
Dr. Rosenberg noted that the OS hazard ratio of 0.5 strongly supports the clinical value of EV + pembrolizumab despite its toxicity profile. There was no indication that the survival curves would converge, although follow-up remains ongoing. He highlighted that OS outcomes in the control arm align with what is typically seen in cisplatin-ineligible patients, a population for which robust OS data following cystectomy are limited. (7)
Dr. Rosenberg highlighted that the pathologic complete response rate with EV + pembrolizumab exceeded 50% in this randomized phase 3 trial, setting a new benchmark in the perioperative treatment of MIBC. When analyzed per protocol, the pCR rate reached 63.6% a level not previously observed in this setting. He noted that these data raise important questions about whether such high response rates could open the door for future bladder-preservation strategies, though the potential impact of field cancerization remains an important consideration that warrants further investigation.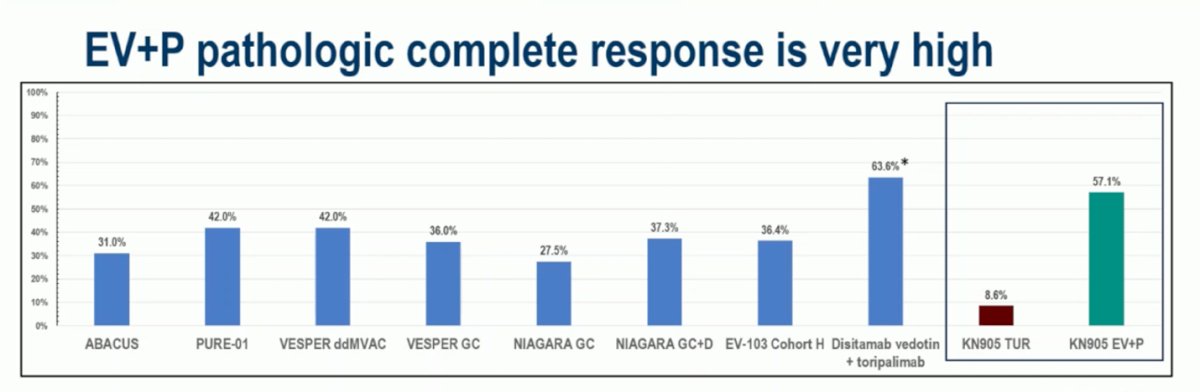
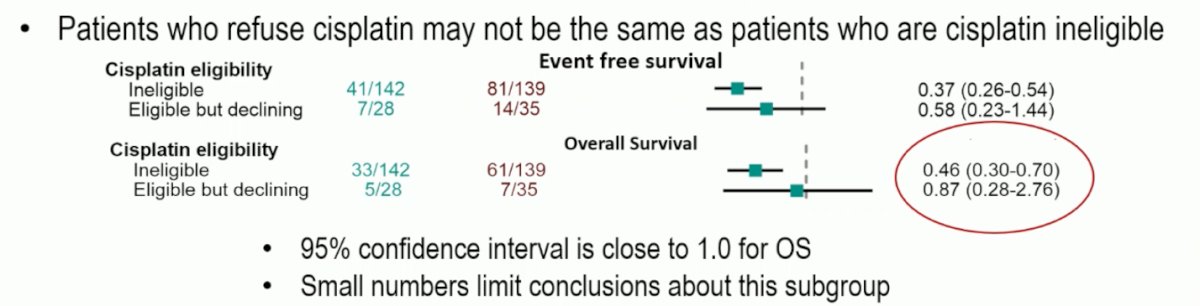
Dr. Rosenberg acknowledged several limitations of KEYNOTE-905, including that adjuvant immunotherapy was not routinely administered in the control arm, as nivolumab only became available midway through the trial received by 16.7% of control patients, depending on local access, reimbursement, and eligibility. Additionally, many patients in the control group likely did not have access to EV + pembrolizumab upon relapse, which could have influenced OS outcomes. He noted that patients who decline cisplatin represent a small and distinct subgroup yet emphasized that these limitations do not detract from the overall strength and impact of the trial’s findings.
Moreover, adjuvant EV + pembrolizumab was administered in 67% of patients who completed surgery, and most of those who started adjuvant therapy were able to complete it. He emphasized that this rate aligns with real-world practice, where a substantial proportion of patients do not proceed to adjuvant treatment due to postoperative recovery, comorbidities, or logistical barriers. Compared to NIAGARA (3), where 81% of surgical patients received adjuvant durvalumab, this highlights that while feasible, the adjuvant component of perioperative therapy may be more challenging to deliver outside of clinical trial settings.
Dr. Rosenberg emphasized that understanding the relative contribution of the neoadjuvant and adjuvant hases of therapy is critical as the field moves forward with perioperative EV + pembrolizumab. Emerging ctDNA data may help refine this question, particularly whether adjuvant therapy is necessary in patients who are ctDNA-negative or achieve pCR after surgery. He noted that, at present, these remain unanswered but essential questions for future trial design and clinical practice.
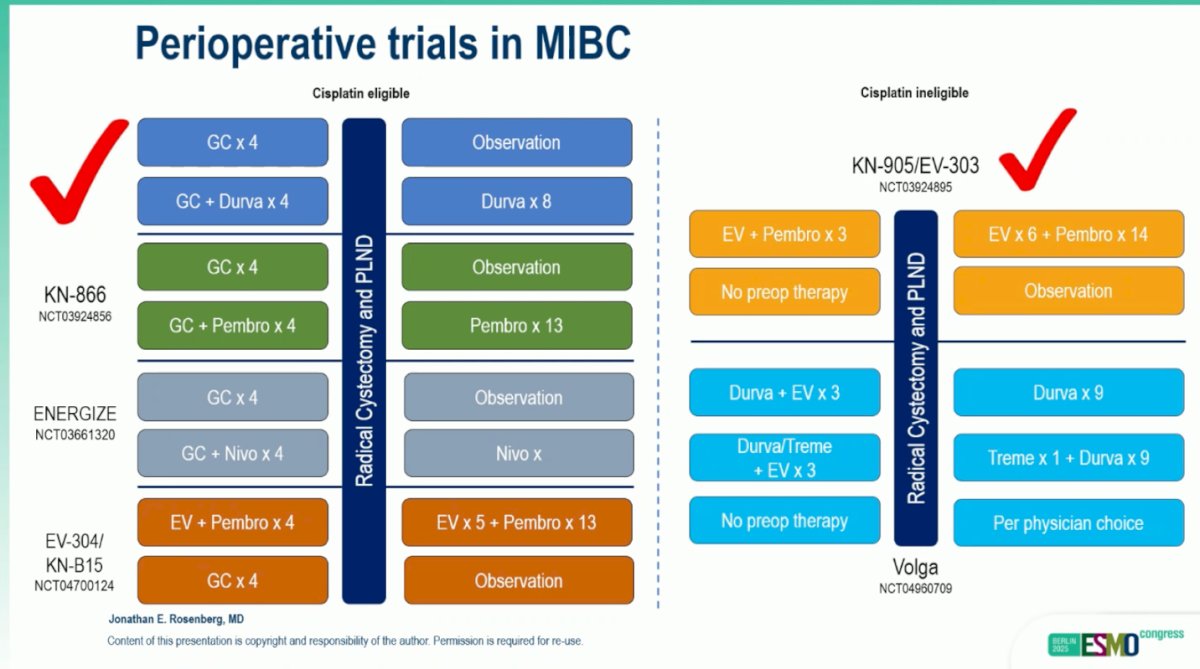
Dr. Rosenberg highlighted the evolving perioperative treatment landscape in MIBC, noting that KEYNOTE-905/EV-303 represents the first phase 3 trial to demonstrate an OS benefit in the cisplatin-ineligible setting. He contrasted this with ongoing studies in cisplatin-eligible populations, such as KN-866, ENERGIZE, and EV-304/KN-B15, emphasizing how these complementary trials will help define the role of immunotherapy and antibody–drug conjugates across the full spectrum of MIBC. A summary of perioperative trials in MIBC is outlined below.
Looking ahead, trial design should test how much perioperative therapy is truly needed and for whom. Pragmatic, ctDNA-guided, adaptive studies could randomize patients after neoadjuvant therapy and surgery by pCR/ctDNA status—de-escalating or omitting adjuvant therapy for pCR/ctDNA-negative patients, and intensifying for high-risk or ctDNA-positive patients. Parallel bladder-preservation cohorts with predefined salvage RC should be prospectively studied to quantify organ-preserving survival.
Finally, Dr. Rosenberg emphasized that an important unanswered question is the optimal first-line treatment for metastatic disease following prior perioperative EV + pembrolizumab. Key considerations include the appropriate interval between completion of EV and/or pembrolizumab before considering re-treatment, and whether rechallenge with immunotherapy at relapse offers meaningful benefit. For now, in patients who relapse early, platinum-based chemotherapy remains the standard of care. He emphasized that future trials directly comparing novel agents or combinations against platinum-based therapy in patients relapsing after EV + pembrolizumab are urgently needed.
Dr. Rosenberg closed his discussion by commending the investigators for completing this ambitious phase 3 study. He underscored that achieving hazard ratios of 0.4–0.5 for both EFS and OS in an older, cisplatin-ineligible population represents a remarkable advance in the field. As data mature, understanding how much benefit is derived from the neoadjuvant versus adjuvant phase will be key to optimizing future trial design. Enfortumab vedotin plus pembrolizumab now stands as a potential new standard of care for patients with muscle-invasive bladder cancer who are unable or unwilling to receive cisplatin-based therapy.
Presented by: Jonathan Rosenberg, MD, Chief, Genitourinary Oncology Service, Division of Solid Tumor Oncology, Enno W. Ercklentz Chair, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
References:
- Powles T, Valderrama BP, Gupta S, Bedke J, Kikuchi E, Hoffman-Censits J, Iyer G, Vulsteke C, Park SH, Shin SJ, Castellano D, Fornarini G, Li JR, Gümüş M, Mar N, Loriot Y, Fléchon A, Duran I, Drakaki A, Narayanan S, Yu X, Gorla S, Homet Moreno B, van der Heijden MS; EV-302 Trial Investigators. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar 7;390(10):875-888. doi: 10.1056/NEJMoa2312117. PMID: 38446675.
- Galsky MD, Hahn NM, Rosenberg J, Sonpavde G, Hutson T, Oh WK, Dreicer R, Vogelzang N, Sternberg CN, Bajorin DF, Bellmunt J. Treatment of patients with metastatic urothelial cancer "unfit" for Cisplatin-based chemotherapy. J Clin Oncol. 2011 Jun 10;29(17):2432-8. doi: 10.1200/JCO.2011.34.8433. Epub 2011 May 9. PMID: 21555688.
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Galsky MD, Witjes JA, Gschwend JE, Milowsky MI, Schenker M, Valderrama BP, Tomita Y, Bamias A, Lebret T, Shariat SF, Park SH, Agerbaek M, Jha G, Stenner F, Ye D, Giudici F, Dutta S, Askelson M, Nasroulah F, Zhang J, Brophy L, Bajorin DF. Adjuvant Nivolumab in High-Risk Muscle-Invasive Urothelial Carcinoma: Expanded Efficacy From CheckMate 274. J Clin Oncol. 2025 Jan;43(1):15-21. doi: 10.1200/JCO.24.00340. Epub 2024 Oct 11. PMID: 39393026; PMCID: PMC11687940.
- Pfister C, Gravis G, Fléchon A, Soulié M, Guy L, Laguerre B, Mottet N, Joly F, Allory Y, Harter V, Culine S; VESPER Trial Investigators. Randomized Phase III Trial of Dose-dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin, or Gemcitabine and Cisplatin as Perioperative Chemotherapy for Patients with Muscle-invasive Bladder Cancer. Analysis of the GETUG/AFU V05 VESPER Trial Secondary Endpoints: Chemotherapy Toxicity and Pathological Responses. Eur Urol. 2021 Feb;79(2):214-221. doi: 10.1016/j.eururo.2020.08.024. Epub 2020 Aug 28. PMID: 32868138.
- Apolo AB, Ballman KV, Sonpavde G, Berg S, Kim WY, Parikh R, Teo MY, Sweis RF, Geynisman DM, Grivas P, Chatta G, Reichert ZR, Kim JW, Bilen MA, McGregor B, Singh P, Tripathi A, Cole S, Simon N, Niglio S, Ley L, Cordes L, Srinivas S, Huang J, Odegaard M, Watt C, Petrylak D, Hoffman-Censits J, Wen Y, Hahn O, Mitchell C, Tan A, Streicher H, Sharon E, Moon H, Woods M, Halabi S, Perez Burbano G, Morris MJ, Rosenberg JE. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2025 Jan 2;392(1):45-55. doi: 10.1056/NEJMoa2401726. Epub 2024 Sep 15. PMID: 39282902; PMCID: PMC11698643.
- Fazili, Adnan N., et al. "IP24-34 CISPLATIN INELIGIBLE PATIENTS WITH MUSCLE-INVASIVE BLADDER CANCER DEMONSTRATE POOR LONG-TERM SURVIVAL FOLLOWING IMMEDIATE RADICAL CYSTECTOMY: A MULTI-INSTITUTIONAL ANALYSIS." Journal of Urology 213.5S (2025): e1278.